Download presentation
Presentation is loading. Please wait.

1
Sara Meltzer, MD, FRCPC, FACP 2010
In-Hospital Management of Patients with Diabetes Sara Meltzer, MD, FRCPC, FACP 2010

2
In-Patient Diabetes Management Objectives:
Importance of Diabetes as a risk factor in hospital outcomes Review physiology of stress and insulin needs Aspects of glucose control in hospital Diet and Testing, Oral agents Insulin use Peri-operative care Emergency Room management Pump therapy – basics in case admitted

3
Objectives of presentation
Review physiology of stress and insulin needs Pre-op considerations Protocol concepts for IV insulin infusions for the OR Post-op on IV’s initially, then eating Emergency room concerns Pump therapy and what to do if someone on pump is admitted… May, 2008

4
Scope of the problem… Common and Increasing Costly:
Overall: > 8% Individuals 65+: > 15% 1 in 3 individuals born in 2000 will develop diabetes in their lifetime 25% of DM1 & 30% of DM2 admitted each year 49% of DM in discharge diagnoses from 1980 to Costly: Medical expenditures/patient 2.4x > non-diabetics 4.6 million DM-associated admissions costs in 2001; 17 million hospital days at > $ 40 billion (US) May, 2008
 May,")
5
Vascular Disease Outcomes in Patients with or without DM: OASIS Registry
8,013 patients with unstable angina or non-Q wave MI 95 hospitals in 6 countries (incl. Canada) Overall mortality 57% in presence of DM May, 2008 Malmberg, Circulation,2000
 Overall mortality. 57% in presence of DM. May, Malmberg, Circulation,2000.")
6
Vascular Disease Outcomes in Patients with or without DM: OACIS Registry
Figure 1. Long-term clinical outcomes among Non-diabetic and diabetic patients in the OACIS registry 8,013 patients with unstable angina or non-Q wave MI 95 hospitals in 6 countries (incl. Canada) Overall mortality increased 57% in presence of DM % of patients May, 2008 Malmberg, Circulation,2000
 Overall mortality increased 57% in presence of DM. % of patients. May, Malmberg, Circulation,2000.")
7
Canadian Acute Coronary Syndrome Registry
4,578 patients with acute coronary syndromes 9 Canadian provinces Yan, JACC, 2004 May, 2008

8
Digami Trial - Sweden 620 patients with DM & MI; mean follow-up 3.4 y.
306 intensive insulin; 314 controls One life saved for every 9 treated patients Death Rate: 138 (44%) in controls; 102 (33%) in the int. tx group (RR 0.72, P=0.011) Malmberg, BMJ, 1997 May, 2008
 in controls; 102 (33%) in the int. tx group. (RR 0.72, P=0.011) Malmberg, BMJ, May,")
9
Stoke patients… 2 - 4 x risk of CVA compared to non-diabetics
(Framingham Study, Paris Prospective Study, Whitehall Study, MRFIT, Rancho Bernardo Study) Hyperglycemia present in 40% of CVA admissions Both ischemic and hemorrhagic CVA have 3X 30-day mortality risk when admission glucose>6-8 mM (Capes, Stroke, 2001, 32-Study Meta-Analysis) Return to work post-CVA 76% if normal admission glucose, vs. 43% if glucose > 6.7 mM (Pulsinelli, Am J Med, 1983) Persistent in-hospital glucose > 7 infarct expansion and functional recovery May, 2008
 Hyperglycemia present in 40% of CVA admissions. Both ischemic and hemorrhagic CVA have 3X 30-day mortality risk when admission glucose>6-8 mM. (Capes, Stroke, 2001, 32-Study Meta-Analysis) Return to work post-CVA 76% if normal admission glucose, vs. 43% if glucose > 6.7 mM. (Pulsinelli, Am J Med, 1983) Persistent in-hospital glucose > 7 infarct expansion and functional recovery. May,")
10
In-Patient Diabetes Management : Objectives
Importance of Diabetes as a risk factor in hospital outcomes Review physiology of stress and insulin needs Aspects of glucose control in hospital Diet and Testing, Oral agents Insulin use Peri-operative care Emergency Room management Pump therapy – basic concepts in case admitted

11
Hyperglycaemia in the Hospital Setting
Pathophysiology Growth hormone Cortisol Catecholamines Glucagon Insulin Glucose May, 2008

12
Considerations in Assessment of Peri-operative Stress
Metabolic stress response Stress hormones & peptides Glucose Insulin Immune dysfunction FFA Ketones Lactate Reactive O2 species Infection dissemination Transcription factors Cellular injury/apoptosis Inflammation / Tissue damage Altered tissue/wound repair Acidosis / Infarction/ischemia Secondary mediators Prolonged hospital stay Disability Death Clement, NEJM 2004 May, 2008

13
Optimal Insulin replacement – Why bother?
Surgical or illness related stress causes insulin needs to increase Insulin is the BEST ANABOLIC HORMONE we have and if the amount available is inadequate for metabolic needs… CATABOLISM occurs. Hyperglycemia increases chances of infections In patients severely ill in ICU, even glucose values > 6mmol/L can be associated with poorer outcomes. May, 2008

14
Insulin secretion Proinsulin Insulin released in equimolar
amounts with C - peptide (90-97%) Pro-insulin & conversion products (3 -10 %) Released into portal circulation Basal secretion is approximately 1 unit / hour In response to food, increases fold Average insulin release about 40 units/day May, 2008
 Pro-insulin & conversion products (3 -10 %) Released into. portal circulation. Basal secretion is approximately 1 unit / hour. In response to food, increases fold. Average insulin release about 40 units/day. May,")
15
Insulin Needs in Hospital
May, 2008

16
Surgical Site Infections Correlation with peri-operative glucose
Surgical Site Infection without DM – 5.3% Surgical Site Infection with DM – 11.2% Adjusted OR 1.80 Adj OR 12.1 May, 2008 Ata et al Arch Surg Sept p858

17
In-Patient Diabetes Management: Objectives
Importance of Diabetes as a risk factor in hospital outcomes Review physiology of stress and insulin needs Aspects of glucose control in hospital Diet and Testing, Oral agents Insulin use Peri-operative care Emergency Room management Pump therapy – basic concepts in case admitted

18
Before the OR Evaluate for concurrent illness and risks related to them e.g. Silent cardiovascular disease (women and men) Autonomic and/or peripheral neuropathy Hypertension/ renal disease Co-existent other autoimmune disease in type 1’s (hypothyroid, Addisons?) Adjust diet to provide optimal nutrition May, 2008
 Adjust diet to provide optimal nutrition. May,")
19
Concept of Diet for Diabetes
Not equal to “ Don’t eat sugar”! Adequate for caloric and nutritional needs Spread carbohydrate (CHO) intake from food throughout day Balance sources from fruits/vegetables and starches with needed protein & fat Insulin must match carbohydrate intake May, 2008
 intake from food throughout day. Balance sources from fruits/vegetables and starches with needed protein & fat. Insulin must match carbohydrate intake. May,")
20
Diet orders… Clarity is very important!
Order ‘diabetic diet’ once eating Clear fluids will often put sugars up as well… try to have it given in 30g servings at meal & snack times… eg. 6 oz apple juice or ginger ale (15g) + 1 jello (15g) Full fluids also better served Q3H and as 30g feeds, if possible... e.g. 1c cream soup (15g) + 1c eggnog (15g) May, 2008
 + 1 jello (15g) Full fluids also better served Q3H and as 30g feeds, if possible... e.g. 1c cream soup (15g) + 1c eggnog (15g) May,")
21
Carbohydrate Intake Peri-operatively
If eating, must consider timing of insulin with meals, size and frequency If on tube feeds – continuous or interrupted? – must plan insulin appropriately If on IV fluids, must provide adequate calories to avoid catabolism and ketone formation, roughly 5g per hour i.e. D5W or D5NS or ½ (~ 2 oz of orange juice only!) If on Total Parental Nutrition – requirements for insulin increase as calories are continuous and similar to when eating May, 2008
 If on Total Parental Nutrition – requirements for insulin increase as calories are continuous and similar to when eating. May,")
22
Capillary Blood Glucose Testing
Clinical Status of Patients Options for CBGM Patients actively treated, often with changes in dietary or CHO intake Q1-4h for patients on IV insulin Q 2-6h for patients on continuous feeds AC meals and HS for patients eating AC and PC meals, HS and 03h for patients requiring excellent control e.g. pregnancy Patients with stable diabetes on insulin or oral agents eating consistent meals with minimal changes in diet plan Routinely AC breakfast and AC supper Once or twice weekly, AC meals and HS Long-term care patients with diabetes which is unstable or DM1 AC meals and HS in order to adjust insulin dose Long-term care patients on insulin or oral agents who are stable AC bkft daily; PC breakfast, lunch, supper in rotation if on oral agents AC meals and HS in rotation: once weekly AC (ante-cebum ) = before meal and PC (post-cebum ) = after meal in Latin May, 2008
 = before meal and PC (post-cebum ) = after meal in Latin. May,")
23
Humulin R Humulin N Humulin R Humulin N Nov. 15 8u 6-2 4u 10u 7.2 5.4
9.3 10.5 16h 2.7 OJ given 2.7 Humulin N 16u Nov. 16 Humulin R 8+2 10u 11.4 Humulin N

24
Oral Agents: Effects and Mechanisms of Action
Diet & Sulfonylureas Metformin a-Glucosidase TZD Insulin Exercise and Glitinides Inhibitors 1° mech ↓ insulin resist ↑ insulin secretion ↓ hepatic output ↓ CH2O absorpt ↑ insulin sens ↑[insulin] HgbA1c↓ Agents Avoiding McD Glyburide Metformin Acarbose Rosiglitazone Gliclazide Miglitol Pioglitzone Glimepiride Repaglinide Nateglinide Adverse Injury Hypoglycemia GI upset GI upset Edema ↓ glucose Effects Wt gain Lactic acidosis Wt gain

25
The Stable Hospitalized Diabetic Patient
Can sometimes continue home regimen, including oral agents, as long as: 1. Stable or improving medical status 2. Predictable nutritional intake 3. Frequent CBG monitoring 4. Sufficient glycemic control May, 2008

26
Insulin Routes of Administration
Subcutaneous variable absorption variable duration of action all formulations may be given this route Intramuscular all can be given, hurts more, faster action Intravenous faster action (T 1/2 = < 5 min.) very consistent action high levels of circulating insulin can be established Intra-peritoneal used in peritoneal dialysis portal levels >> systemic - more physiologic used in implanted pumps… trouble with omental blocking May, 2008
 very consistent action. high levels of circulating insulin can be established. Intra-peritoneal. used in peritoneal dialysis. portal levels >> systemic - more physiologic. used in implanted pumps… trouble with omental blocking. May,")
27
Regular insulin - half life
If given IV…. T ½ = min. If given IM… T ½ = hours If given IP… T ½ = hours If given SC … T ½ = 6 hours May, 2008

28
Insulin Types & Action Profiles: Short-acting
May, 2008

29
Insulin Types & Action Profiles: Intermediate and Long-acting
Name Onset (h) Peak action (h) Duration of action (h) NPH Human Novolin NPH Humulin NPH 1 – 3 5 – 10 16 – 18 Glargine Lantus 4 – 6 8 – 16 20 – 36 Detemir Levemir 2 – 4 6 – 12 May, 2008
 Peak action (h) Duration of action (h) NPH. Human. Novolin NPH Humulin NPH 1 – 3. 5 – – 18. Glargine. Lantus 4 – 6. 8 – – 36. Detemir. Levemir 2 – 4. 6 – May,")
30
Factors influencing insulin action
Blood Flow Site abd>>arm>>leg lipodystrophy Depth Exercise Ambient temperature Smoking Dissociation Rate Species human>pork Type zinc “heavy” >> crystals formed>>albumin bound>> protamine >> crytalline >> monomeric Concentration Volume Jet injection May, 2008

31
Insulin orders... Clarity counts!
For patient on IV’s Best option = iv insulin with adjustment 2nd best option is Q6H regular SC or R ac meals and NPH at HS For patients who are eating but unstable: HS and Regular pre-meal … both with adjustment scale For patients who are eating but unstable amounts: HS and Regular pre-meal if needed + Rapid acting post-meal … only adjust pre-meal regular with sliding scale For patients who are eating and stable: Regular AC meals and NPH at HS, adjusted with sliding scale… may be able to reduce testing frequency but should still cover all parts of the day May, 2008

32
Insulin Therapy: Temporary use...
Pregnancy… can’t use pills! Surgery … increased need. Medication such as steroids which dramatically increase insulin needs. Concurrent illness … eg. MI or CVA… better peri-event sugar control improves morbidity and mortality. Good sugar control helps patients recover and leave hospital faster! May, 2008

33
Other Indications for Insulin Therapy in Type 2
Development of severe hyperglycemia with ketones Uncontrolled weight loss. Renal or hepatic disease with contraindications to use of oral agents Allergy or hypersensitivity to oral agents Latent autoimmune disease in adults - type 1 1/2 (?) May, 2008
 May,")
34
Concept of BASAL insulin needs
Any person, eating or not requires insulin to live… 24 hours a day! Basal needs (no food): often lower levels between 12 am and 4 am, an increase prior to awaking until about 8 am, then often about u/hr. In response to food, proportion of insulin release closely relates to CHO content of the meal +/- presence of protein & fat in it. May, 2008
: often lower levels between 12 am and 4 am, an increase prior to awaking until about 8 am, then often about u/hr. In response to food, proportion of insulin release closely relates to CHO content of the meal +/- presence of protein & fat in it. May,")
35
Insulin replacement for Type 1
In type 1… no insulin of their own without injections… never leave them without insulin coverage! May, 2008

36
Insulin replacement for Type 2
Type 2 on diet: if not eating, can often keep fasting glucose normal… may not need basal Type 2 on oral agents: if not eating… usually needs additional amounts of insulin to keep normal sugars, even without eating. Type 2 on insulin: often some remaining basal insulin but needs coverage even if not eating to have good glucose entry into cells. May, 2008

37
Establishing “basal” needs – i. e
Establishing “basal” needs – i.e. amount needed if no significant carbohydrate intake Establish known total daily dose (TDD) i.e. sum of all insulin taken in a normal day Determine what ½ of that amount is… approximate amount of insulin needed if no CHO intake Determine the necessary hourly rate of this “base need” [i.e. [(TDD/2)] 24 = X u/h Set up an IV insulin infusion with this hourly rate as a starting point and allow adjustment up or down until target range is reached May, 2008
 i.e. sum of all insulin taken in a normal day. Determine what ½ of that amount is… approximate amount of insulin needed if no CHO intake. Determine the necessary hourly rate of this base need [i.e. [(TDD/2)] 24 = X u/h. Set up an IV insulin infusion with this hourly rate as a starting point and allow adjustment up or down until target range is reached. May,")
38
May, 2008

39
Patients taking insulin who are NPO or Pre-op:
Items of the order sheet are based on the following premises… Patients should receive glucose IV at ~ 5g/h in order to provide essential minimum calories to avoid ketosis of fasting. Can be done using D10W at 50cc/h if fluid status is a problem, or D5W or for most patients. Capillary blood glucose should be measured frequently initially Q1H and subsequently decreasing frequency depending on stability of blood sugar, with a minimum frequency of Q4H. Intravenous insulin should always be REGULAR insulin (either Humulin R or Novolin Toronto – be precise to avoid confusion). May, 2008
. May,")
40
Patients taking insulin who are NPO or Pre-op:
Premise which permits determination of the initial insulin infusion rate: This is usually based on a simple calculation of the basal insulin requirements. Approximately half of the insulin given every day covers the meals – the other half covers the basal needs. Therefore, calculate ½ of the total daily dose (TDD) of insulin to allow coverage of basal needs, converted to units/hour. i.e. ½ TDD ÷ 24 = starting insulin infusion rate. If the infusion rate is < 1.0units/h – use 10units/250ml NS (1unit = 25ml.) If the infusion rate is ≥ 1.0 units/h – use 25units/250ml NS (1unit / 10ml) May, 2008
 of insulin to allow coverage of basal needs, converted to units/hour. i.e. ½ TDD ÷ 24 = starting insulin infusion rate. If the infusion rate is < 1.0units/h – use 10units/250ml NS (1unit = 25ml.) If the infusion rate is ≥ 1.0 units/h – use 25units/250ml NS (1unit / 10ml) May,")
41
Establishment of basal infusion rate:
May, 2008

42
Adjustments to Insulin Infusion Rate:
If CBG (mmol/L) is: ≤ Stop insulin infusion temporarily; continue glucose infusion at previous rate and give 20ml of D50W IV push over 2-3 minutes. Inform MD. Recheck CBG in10 min. & repeat D50W until CBG ≥6mmol/L, then resume the insulin infusion at ½ previous rate. 4.1 – Decrease insulin infusion rate by (indicate with checkmark) □ half of current rate (for fractions of a ml., decrease to nearest whole number) □ ______ units/hr. (i.e. _______ ml/hr). 7.1 – Continue the current insulin infusion rate. 10.1 – Increase current infusion rate by ____units/hr (i.e. ___ml/hr). 14.1 – Increase current infusion rate by ____units/hr. (i.e. ___ml/hr). > Increase current infusion rate by ____units/hr. (i.e. ___ml/hr). and inform MD. May, 2008
 is: ≤ 4.0 Stop insulin infusion temporarily; continue glucose. infusion at previous rate and give 20ml of D50W IV push. over 2-3 minutes. Inform MD. Recheck CBG in10 min. & repeat D50W until CBG ≥6mmol/L, then resume the. insulin infusion at ½ previous rate. 4.1 – 7.0 Decrease insulin infusion rate by (indicate with checkmark) □ half of current rate (for fractions of a ml., decrease to nearest whole number) □ ______ units/hr. (i.e. _______ ml/hr). 7.1 – 10.0 Continue the current insulin infusion rate – 14 Increase current infusion rate by ____units/hr (i.e. ___ml/hr) – 18 Increase current infusion rate by ____units/hr. (i.e. ___ml/hr). > 18 Increase current infusion rate by ____units/hr. (i.e. ___ml/hr). and inform MD. May,")
43
Post-operative orders once ready to resume full fluids
Re-order “diabetic diet …X….Kcal/day” In patients normally on oral agents, re-order once patient is eating may need lower doses as intake may be poor may need “insulin adjustment scale” or “sliding scale” for values above 8 or 10 mmol/L In patients normally on insulin, restart subcutaneous insulin dose at least minutes prior to the discontinuation of the IV, even if at a lower dose than prior to admission… May, 2008

44
Returning to eating Once patient ready to return to meals, likely not eating well, so work in reverse… i.e. Hourly dose given X 24 = approximate present “basal needs” which can be distributed to be given prior to meals and HS in the proportion of: Use insulin adjustment scale to correct for food and relative proportion errors Adjust base dose daily based on previous day’s needs until control achieved and on normal diet Time Breakfast Lunch Supper HS NPH or basal % Regular/rapid % % % May, 2008

45
Insulin orders – patient eating
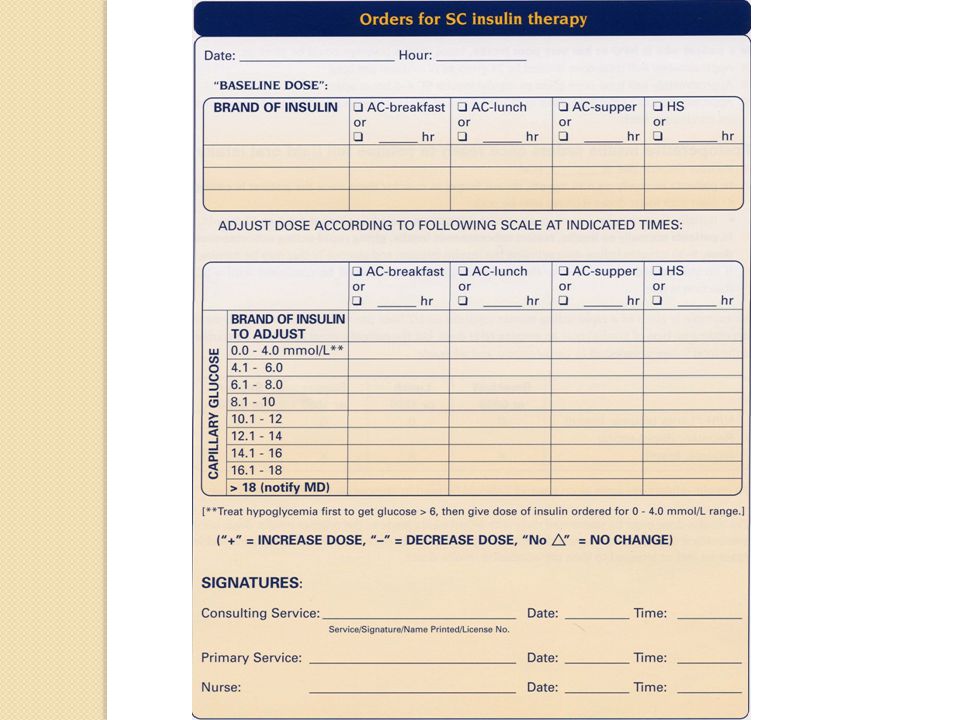
Ordered baseline dose (Indicate clearly type and brand of insulin) Breakfast or 0600h Lunch or 12h Supper or 18h HS or 22h NPH/glargine/detemir 0% 40% Regular/lispro/aspart/glusine 25% 15% 20% Example of insulin adjustment scale for pre-meal or HS insulin adjustment If capillary blood glucose is: ≤ 4 mmol/L Treat for low blood sugar; decrease ordered dose by 4units 4.1 – 6.0 mmol/L Decrease ordered dose by 2 units 6.1 – 10.0 mmol/L Give ordered baseline dose 10.1 – 12.0 mmol/L Increase ordered dose by 2 units 12.1 – 14.0 mmol/L Increase ordered dose by 4 units 14.1 – 16.0 mmol/L Increase ordered dose by 6 units 16.1 – 18.0 mmol/L Increase ordered dose by 8 units > 18.0 mmol/L Increase ordered dose by 10 units; inform MD November, 2010
 Breakfast or 0600h. Lunch or 12h. Supper or 18h. HS or 22h. NPH/glargine/detemir. 0% 40% Regular/lispro/aspart/glusine. 25% 15% 20% Example of insulin adjustment scale for pre-meal or HS insulin adjustment. If capillary blood glucose is: ≤ 4 mmol/L. Treat for low blood sugar; decrease ordered dose by 4units. 4.1 – 6.0 mmol/L. Decrease ordered dose by 2 units. 6.1 – 10.0 mmol/L. Give ordered baseline dose – 12.0 mmol/L. Increase ordered dose by 2 units – 14.0 mmol/L. Increase ordered dose by 4 units – 16.0 mmol/L. Increase ordered dose by 6 units – 18.0 mmol/L. Increase ordered dose by 8 units. > 18.0 mmol/L. Increase ordered dose by 10 units; inform MD. November,")
47
Additional considerations once eating:
IV insulin – Regular is preferred, as analogues have no advantage if not SC and are more expensive. Once eating, if previously on analog insulins, can re-start. Monitor glucose at least every h; ideally, pre-meals. In situation where changes of need may occur rapidly, use of aspart (Novorapid®) or lispro (Humalog®) SC may be easier, since it can be given with the meal. Rapid acting analogs, however, only lasts 4-6h, not 6-8h as “regular” does. Initially CBG testing would be ordered as 0600, 1200, and 2400 but, if switched to eating, adjust timing to meal delivery & 2200 hr. May, 2008
 or lispro (Humalog®) SC may be easier, since it can be given with the meal. Rapid acting analogs, however, only lasts 4-6h, not 6-8h as regular does. Initially CBG testing would be ordered as 0600, 1200, 1800 and 2400 but, if switched to eating, adjust timing to meal delivery & 2200 hr. May,")
48
Patients going for tests
Adjust timing of tests to facilitate insulin and diet needs whenever possible. If patient likely to be gone at a snack time or may have lunch delays by waiting times in X-ray, etc… send juice and a snack with them. Reassess patient on return from test with capillary blood glucose & adjust therapy as needed. May, 2008

49
“Sliding Scales” – why such a bad reputation?
Inappropriately, they are used alone….as the only insulin ordered… To work, the sliding scale should only help fix the “ordered dose” The information from the adjustments used in the sliding scale should be used to help correct the “base dose” the next day. May, 2008

50
Sliding scale in hospital
May, 2008

51
Insulin adjustment scale for patients at home or for insulin sensitive type 1
May, 2008

52
In-Patient Diabetes Management:Objectives
Importance of Diabetes as a risk factor in hospital outcomes Review physiology of stress and insulin needs Aspects of glucose control in hospital Diet and Testing, Oral agents Insulin use Peri-operative care Emergency Room management Pump therapy – basic in case admitted

53
ER or Hospital Management - Challenges to Care:
Meals are : irregular, or missed completely rarely the same as normal diet or on time Capillary Blood Glucose Monitoring is: Done irregularly, not always in relation to meals Difficult to arrange hourly for IV infusions due to nursing staff limitations on occasion. Staff changes are frequent, thus less continuity of care. Patient’s participation in self care may be severely limited. Patient, by definition, will be ill and inter-current illness often substantially changes insulin requirements… often increasing them due to the psychological and physiological stresses. May, 2008

54
Evaluation in the Emergency Room….
Usual treatment often gives valuable insight into how patient’s care should be done Is patient able to eat normally? Is patient NPO or on IV infusion? Does patient normally take insulin? - If so, need to know: what kinds of insulin, type and exact name how much, and at what times? DETAILED EXACT INFO needed!!! May, 2008

55
ER IV insulin infusions – pros and cons
In some ER situations, due to staffing issues, hourly CPG to adjust an IV protocol initially may not be possible. Use an insulin adjustment scale as one would use normally pre-meal using ¼ of total daily dose [TDD] as top limit of sliding scale for highest glucose values. To calculate dosage to use for basal needs if not eating… Calculate Total Daily Dose (TDD) divide by 2 (since ½ insulin for food) Divide this amount over the day % overnight and the rest split in 3 with a bit more at breakfast than lunch as regular or analogue pre-meal or 0600, 1200, 1800 hours and NPH at HS. e.g % - 15% - 20% can be given pre-meal regular or RA % as longer acting evening insulinspre May, 2008
 divide by 2. (since ½ insulin for food) Divide this amount over the day - 40 % overnight and the rest split in 3 with a bit more at breakfast than lunch as regular or analogue pre-meal or 0600, 1200, 1800 hours and NPH at HS. e.g. 25% - 15% - 20% - 0 can be given pre-meal regular or RA % as longer acting evening insulinspre. May,")
56
Continue usual diet and pills Is glucose stable and well controlled?
Patient with DM in ER Normally on diet ± oral agents Able to eat Not able to eat Give consistent glucose load by IV (~ 5 g/h) to avoid ketosis Eg. IV D5 W or 100cc/h or D10 50 cc/h if fluid an issue. Continue usual diet and pills Is glucose stable and well controlled? YES NO Initiate an IV insulin infusion with concept of giving 10 – 12 u/24 h. (or presumption of potential total insulin dose as 20 u/day) Ie. IV insulin to 0.4 u/h or Base dose ac meals & HS of : N R/RA with insulin adjustment scale. Monitor glucose as needed. Monitor glucose q 4-6 h as needed, no other therapy for DM likely needed. May, 2008
 to avoid ketosis. Eg. IV D5 W or 100cc/h or. D10 50 cc/h if fluid an issue. Continue usual diet and pills. Is glucose stable and well controlled YES. NO. Initiate an IV insulin infusion with concept of giving 10 – 12 u/24 h. (or presumption of potential total insulin dose as 20 u/day) Ie. IV insulin to 0.4 u/h or. Base dose ac meals & HS of : N R/RA with insulin adjustment scale. Monitor glucose as needed. Monitor glucose q 4-6 h as needed, no other therapy for DM likely needed. May,")
57
Patient with DM in ER Normally on insulin Able to eat Not able to eat
Give consistent glucose load by IV (~ 5 g/h) to avoid ketosis Eg. IV D5 W or 100cc/h or D10 50 cc/h if fluid volume is an issue. Continue usual diet and insulin if possible Is glucose stable and well controlled (ie < 10mmol/L)? If type 1, initiate IV or Q4-6 SC insulin regimen once glucose above 6 mmol/L and check for ketones. Monitor glucose q 4-6 h as needed, continuing therapy as planned. YES NO Ordered dose: Breakfast or 0600 Lunch or 1200 Supper or 1800 HS or 2400 NPH/lente/ultralente (source, brand) X Regular / Rapid acting EG. Insulin adjustment scale for rapid acting insulin before each meal: If capillary blood glucose is: ≤4.0 mmol/L Treat for low blood sugar; decrease ordered dose by 4 units 4.1–6.0 mmol/L Decrease ordered dose by 2 units 6.1–10.0 mmol/L Give ordered dose 10.1–12.0 mmol/L Increase ordered dose by 2 units 12.1–14.0 mmol/L Increase ordered dose by 4 units 14.1–18.0 mmol/L Increase ordered dose by 6 units >18.0 mmol/L Increase ordered dose by 8 units and inform physician Initiate insulin …either as an IV insulin infusion of base dose [total daily dose / 2] distributed over 24 hour as starting insulin dose for infusion… ie. IV insulin to start … @ (TDD/2) = X u/h (initial rate) & adjust or Base dose ac meals & HS of : N % R/RA 25% - 15% - 20% - 0 with insulin adjustment scale. Monitor glucose as needed. May, 2008
 to avoid ketosis. Eg. IV D5 W or 100cc/h or D10 50 cc/h if fluid volume is an issue. Continue usual diet and insulin if possible. Is glucose stable and well controlled (ie < 10mmol/L) If type 1, initiate IV or Q4-6 SC insulin regimen once glucose above 6 mmol/L and check for ketones. Monitor glucose q 4-6 h as needed, continuing therapy as planned. YES. NO. Ordered dose: Breakfast. or Lunch. or Supper or HS. or NPH/lente/ultralente. (source, brand) X. Regular / Rapid acting. EG. Insulin adjustment scale for rapid acting insulin before each meal: If capillary blood glucose is: ≤4.0 mmol/L. Treat for low blood sugar; decrease ordered dose by 4 units. 4.1–6.0 mmol/L. Decrease ordered dose by 2 units. 6.1–10.0 mmol/L. Give ordered dose. 10.1–12.0 mmol/L. Increase ordered dose by 2 units. 12.1–14.0 mmol/L. Increase ordered dose by 4 units. 14.1–18.0 mmol/L. Increase ordered dose by 6 units. >18.0 mmol/L. Increase ordered dose by 8 units. and inform physician. Initiate insulin …either as. an IV insulin infusion of base dose [total daily dose / 2] distributed over 24 hour as starting insulin dose for infusion… ie. IV insulin to start (TDD/2) = X u/h (initial rate) & adjust. or. Base dose ac meals & HS of : N % R/RA 25% - 15% - 20% - 0. with insulin adjustment scale. Monitor glucose as needed. May,")
58
In-Patient Diabetes Management Objectives:
Importance of Diabetes as a risk factor in hospital outcomes Review physiology of stress and insulin needs Aspects of glucose control in hospital Diet and Testing, Oral agents Insulin use Peri-operative care Emergency Room management Pump therapy – basic concepts in case admitted

59
The dilemma of pump patients…
That patient in Bed 3 is on an insulin pump – you take her! No, I can’t… I don’t know anything about pump therapy… Well neither does the doctor who’s on tonight – so what do we tell the patient? May, 2008

60
Core Concepts of Insulin Pump Prescriptions (~25% of type 1’s now on pumps!)
“Basal” = Basal dose – units per hour 24 – 04h …0.6u 04–07h …1.0u 07–12h …0.8u 12–18 …0.6u 18–24h …0.7u Bolus doses: Ratio of grams CHO covered by 1 unit of insulin 24–07h 1u/20g 07–11h 1u/8g 11–15h 1u/12g 15–20h 1u/10g 20-24h 1/15g Correction factor – the amount of glucose lowered by 1 u (in mmols) 24–07h 1u/3 07–11h 1u/1.5 11–15h 1u/2 15–20h 1u/2 20-24h 1/3 Basal = baseline dose = insulin amount given over 24 hours without food Bolus = dose given to cover food intake Total daily dose = insulin amount used as basal + bolus given for meals Insulin Sensitivity Factor (ISF) or Correction factor indicates mmol increments for sliding scale (often must be doubled if ill or stressed e.g. hospital i.e. mmol denominator must be decreased) May, 2008
 24–07h 1u/3. 07–11h 1u/ –15h 1u/2. 15–20h 1u/ h 1/3. Basal = baseline dose = insulin amount given over 24 hours without food. Bolus = dose given to cover food intake. Total daily dose = insulin amount used as basal + bolus given for meals. Insulin Sensitivity Factor (ISF) or Correction factor indicates. mmol increments for sliding scale (often must be doubled. if ill or stressed e.g. hospital i.e. mmol denominator must be decreased) May,")
61
The Type 1 on pump or who “carb counts”…
In order to order IV or alternative subcutaneous insulin doses … need to know the total daily dose (TDD) – pumps have that info in their minicomputers… ask the patient! For Patients who don’t know/can’t tell you their Total Daily Dose To determine basal total: Ask them (or review basal on the pump) to find basal rates by hour… calculate: [basal rates X numbers of hours at each] = total basal rate To determine meal amounts if carbohydrate counting: Ask them what their “normal” meal carbohydrate intake is, then ask them what they usually take to cover that… will often get relative doses for breakfast, lunch and dinner that way. If they are not able to tell you their usual meal CHO intake, assume 40g at breakfast and 50g for lunch and supper – multiply by ratio found under bolus wizard or EZ carbs eg 1u/8g at bkft = 5units Total Daily Dose = sum of basal rates + usual amount for each meal… May, 2008
 – pumps have that info in their minicomputers… ask the patient! For Patients who don’t know/can’t tell you their Total Daily Dose. To determine basal total: Ask them (or review basal on the pump) to find basal rates by hour… calculate: [basal rates X numbers of hours at each] = total basal rate. To determine meal amounts if carbohydrate counting: Ask them what their normal meal carbohydrate intake is, then ask them what they usually take to cover that… will often get relative doses for breakfast, lunch and dinner that way. If they are not able to tell you their usual meal CHO intake, assume 40g at breakfast and 50g for lunch and supper – multiply by ratio found under bolus wizard or EZ carbs eg 1u/8g at bkft = 5units. Total Daily Dose = sum of basal rates. + usual amount for each meal… May,")
62
Search for “micro” complications!
Nephropathy: Check albumin/creatinine ratio (> 2.0 men or 2.8 women = trouble) creatinine clearance by Cockcroft-Gault equation Urinalysis – for cells, protein, or signs of infection Retinopathy Be sure patient has been seen by competent ophthalmologist and eyes assessed within last year Neuropathy Test ankle jerks + 10g monofilament on toes Ask about erectile dysfunction, bowel problems, excess sense of fullness post-meal, postural hypotensive symptoms May, 2008
 creatinine clearance by Cockcroft-Gault equation. Urinalysis – for cells, protein, or signs of infection. Retinopathy. Be sure patient has been seen by competent ophthalmologist and eyes assessed within last year. Neuropathy. Test ankle jerks + 10g monofilament on toes. Ask about erectile dysfunction, bowel problems, excess sense of fullness post-meal, postural hypotensive symptoms. May,")
63
Search for “macro” risk factors or complications
Lipid profile at least yearly evaluation of LDL and HDL cholesterols, Triglycerides, apo-B. Cardiac assessment ECG + / - stress test Hypertension – assess and control to < 130/85 Peripheral Vascular Disease… Vascular flow assessments with doppler PRN Assess for bruits or intimal media thickening Foot care… Look at the foot – reflexes, monofilament, ulcers, redness, callouses and general state of care May, 2008

64
Make sure outpatient follow-up well established
Remember to use entire team… nursing, dietitian, family MD, social worker and community services, if needed. Plan appropriate steps long before day of discharge. Survival booklets available in English & French – order via Endocrinology office… May, 2008

65
Thank you for your attention… Questions ???
65

Similar presentations

>")





>")


 An Overview for Clinical Nurses NIH-NINDS U01 NSO69498.>")



. Who needs screening for DM? Age >45 Obese – BMI >25 1 st degree relative with DM Racial groups: –African American –Hispanic American.>")




