Download presentation
Presentation is loading. Please wait.

1
How to Complete a Clinically Relevant & Directed Neurologic Exam in ED CVA Patients Edward Sloan, MD, MPH Associate Professor Department of Emergency Medicine University of Illinois College of Medicine Chicago, IL 54 1 54

2
Global Objectives Improve pt outcome in stroke
Make consistent and reliable neuro Dx Provide rationale ED therapies Maximize ongoing learning Be comfortable with our clinical skills Minimize any unnecessary work 54 2 54

3
Session Objectives Present clinical case history
Consider acute stroke for a directed exam Ask clinically relevant questions Conduct a directed ED H&P Examine the NIH Stroke Scale (NIHSS) Review optimal ED documentation 54 2 54
 Review optimal ED documentation")
4
“Real” Session Objectives
State the bare minimum that must be done in order to get the job done. Allow you to forget about doing the rest. 54 2 54

5
Why Do This Exercise? How to proceed is unclear for many.
A uniformly applied minimal standard is better than a non-uniform approach. Once achieved, a minimal standard can be enhanced. This is a standard of care issue. 54 2 54

6
Some Perspective Stroke is a common ED problem.
Outcome from stroke can be devastating. Use of tPA in stroke is an important issue. Guidelines are being developed at the local and national level regarding CVA pts. The cornerstone of this activity remains the front line Emergency Physician. 54 2 54

7
A Disclaimer. Although I have listened to many lectures on the neurologic exam, I am not fully comfortable with this part of my practice. What I do in clinical practice may fall below the standard of care. Others also may fall short of a reasonable standard in doing a stroke neuro exam. 54 2 54

8
A Pledge. I will not simply create controversy.
I will attempt to clarify what are the important clinical questions. I will attempt to state which physical and neuro exam elements are useful and why. I will demonstrate a way in which the physical exam findings can be recorded in order to facilitate patient care. 54 2 54

9
A Clinical History A 62 year old female acutely developed aphasia and right sided weakness while in the grocery store. The store clerk immediately called 911, with the arrival of CFD paramedics within 9 minutes, at 6:43 pm. She arrived at the ED at 7:05 pm, completed her head CT at 7:25 pm, and obtained a neuro consult at 7:35 pm, approximately one hour after the onset of her symptoms. What are the next Rx steps? 54 3 54

10
ED Presentation What parts of the history and physical exam really matter? Why? In what way will the neurologic exam direct the ED diagnosis and therapy? What must be documented? Why? 54 3 54

11
Acute Neurologic Exam Questions
What general exam should be done? What neuro exam should be done? What exam findings guide therapy? What exam findings predict outcome? What is the NIH stroke scale? How can documentation be optimized? 54 4 54

12
Acute Ischemic Stroke: Etiology
Thrombotic, embolic, hypoperfusion Majority are vessel thrombosis Clot formation on diseased vessel 20% are embolic, from heart, great vessels Hypoperfusion with cardiogenic shock 5 17

13
Acute Ischemic Stroke: Syndromes
Anterior cerebral Middle cerebral Posterior cerebral Vertebrobasilar Basilar artery occlusion Cerebellar Lacunar Arterial dissection 5 17

14
Acute Ischemic Stroke H & P: Some Practical Questions
Does the neuro exam tell us anything the CT scan does not? Do we need to localize the CVA clinically? Isn’t a large ICH evident most often based on the pt’s mental status and overall appearance? Who checks for proprioception or a positive Rhomberg in a pt with a CVA? 5 17

15
Acute Ischemic Stroke H & P: Rationale for Exam Findings
To make the correct diagnosis To identify a stroke syndrome To identify CVA precipitants/etiology To determine further diagnostic tests To determine ED therapies To allow for proper documentation 5 17

16
Rationale for a Directed Neuro Exam: To Make the Correct Diagnosis
A complete neuro exam helps when Sx are vague, mild or confusing TIA, seizure or migraine variant setting Exam puts a name on non-persistent Sx Most acute stroke pts have obvious Sx What else causes L sided paralysis acutely? Doesn’t the constellation of Sx make the Dx? Which Dx must be immediately excluded? 5 17

17
To Make the Correct Diagnosis: A Stroke Differential Diagnosis
Hypertensive encephalopathy Subdural, epidural hematoma Meningitis, encephalitis, abcess, labarynthitis Seizure, SE, Todd’s paralysis Neoplasm Hypoglycemia, metabolic Migraine Peripheral nerve, Bell’s palsy Multiple sclerosis 5 17

18
Rationale for a Directed Neuro Exam: To Identify a Stroke Syndrome
The neurologic exam must establish: anterior or posterior circulation location. if the Dx is cerebellar hemorrhage. if the lesion is in the brain stem. if the lesion is in the spinal cord. There is no other requirement with regards to the acute Dx of the stroke pt. 5 17

19
To Identify a Stroke Syndrome: Anterior vs. Posterior Circulation
Markedly different presentations. Anterior circulation: Sx (motor, sensory) on the same body side Sx contralateral to the side of the CVA Visual field deficits, gaze abnormalities Aphasia, dysarthria, apraxia 5 17
 on the same body side. Sx contralateral to the side of the CVA. Visual field deficits, gaze abnormalities. Aphasia, dysarthria, apraxia")
20
To Identify a Stroke Syndrome: Anterior vs. Posterior Circulation
Minimal (transient) motor abnormality Marked sensory (LT, pinprick) abnormality Visual abn, oculomotor palsy Ataxia, hemiballism Vertebrobasilar system: CN, body motor deficits on alternating sides Hemiparesis, hemiplegia, dizziness, dim vision, dysarthria, dysphagia, vomiting 5 17
 motor abnormality. Marked sensory (LT, pinprick) abnormality. Visual abn, oculomotor palsy. Ataxia, hemiballism. Vertebrobasilar system: CN, body motor deficits on alternating sides. Hemiparesis, hemiplegia, dizziness, dim vision, dysarthria, dysphagia, vomiting")
21
Rationale for a Directed Neuro Exam: Cerebellar Hemorrhage
A specific clinical presentation: Nausea, vomiting, central vertigo Headache, nuchal rigidity Syncope, ataxia, inability to ambulate AMS when brainstem is compressed Pathologic respiratory pattern A true surgical emergency (evacuation). Often difficult to detect on CT. 5 17
. Often difficult to detect on CT")
22
Rationale for a Directed Neuro Exam: Brain Stem Lesion
A specific clinical presentation: Markedly abnormal vital signs Altered mental status, often coma Pupillary abnormalities Abnormal respirations Often with the need for immediate intubation A picture of critical illness 5 17

23
Rationale for a Directed Neuro Exam: Spinal Cord Lesion
Injury with unilateral or bilateral findings Complete spinal cord injury Partial syndromes Central, anterior, Brown-Sequard Cauda equina Tumor, abcess, epidural hematoma Disc disease/acute herniation No Hx, Px findings that suggest a CVA 5 17

24
Rationale for a Directed Neuro Exam: To ID Stroke Precipitant/Etiology
What is the etiology of the stroke? What findings suggest the need for a specific Rx or further Dx testing? Four stroke etiologies are noted: Thrombotic (atherosclerosis) Embolic Hemorrhage Subarachnoid hemorrhage 5 17
 Embolic. Hemorrhage. Subarachnoid hemorrhage")
25
To ID Stroke Precipitant/Etiology: Findings Suggesting Embolic CVA
Most often anterior circulation process Abrupt Sx onset, worst deficit at onset Carotid bruit: carotid artery occlusion and source of embolism A Fib: embolism source of MCA stroke Heart murmur: valve pathology, embolism 5 17

26
To ID Stroke Precipitant/Etiology: Findings Suggesting Thrombotic CVA
Most often posterior circulation process Gradual Sx onset, stepwise deficit Carotid bruit: evidence of atherosclerosis LV Heave: cardiac hypertrophy Aorta: AAA indicated vasculopathy Extremities: poor pulses, atherosclerosis 5 17

27
To ID Stroke Precipitant/Etiology: Findings Suggesting Hemorrhagic CVA
Impaired consciousness key element Abrupt Sx onset, usu max deficit early HTN, bradycardia Papilledema, hemorrhages 5 17

28
To ID Stroke Precipitant/Etiology: Findings Suggesting Subarachnoid
Impaired consciousness key element Varied Sx onset and deficit progression Severe headache, neck stiffness Retinal hemorrhages Meningismus 5 17

29
Rationale for a Directed Neuro Exam: To Determine Further Dx Tests
Very few further tests in the ED: EKG for dysrhythmia CXR to rule out tumor, CHF Contrast Head CT for abcess, tumor Angiography for suspected SAH, aneurysm CT, US for suspected large AAA ECHO for suspected acute cardiac lesions MRI, other tests rarely indicated 5 17

30
Rationale for a Directed Neuro Exam: To Determine ED Therapies
Very few specific ED therapies. Embolic, thrombotic CVAs: ASA, Heparin, tPA Hemorrhagic CVA Mannitol, decadron, phenytoins Operative intervention Subarachnoid hemorrhage Nimodipine, ?? OR 5 17

31
Rationale for a Directed Neuro Exam: To Allow for Proper Documentation
What was the clinical state of the pt when in our ED, and under our care? Did we complete exam sufficient to direct Rx that would optimize this pt’s care? Did our clinical Rx follow our exam? If necessary, could a NIHSS score be assigned in retrospect 5 17

32
Acute Stroke: Historical Elements
When did symptoms begin? Onset? Prior history of similar symptoms? When was the patient last seen normal? Risk factors? Medical hx that would preclude tPA use? 5 17

33
Acute Stroke: Physical Exam
Vital signs, pulse ox, accucheck HEENT: Pupils, papilledema, airway Neck: Bruits, nuchal rigidity Chest: Rales (CHF, aspiration) Cardiac: Gallop, murmur, dysrhythmias, ventricular heave 5 17
 Cardiac: Gallop, murmur, dysrhythmias, ventricular heave")
34
Acute Stroke: Physical Exam
Abd: Evidence of AAA Ext: Evidence of CHF, DVT, vascular Dx Skin: Evidence of infectious etiology Neuro: Mental status, CN, eye exam, motor, sensory, reflexes, cerebellar, visual, language, neglect 5 17

35
Neurologic Exam: Mental Status
Level of consciousness (AVPU) Alert Responds to verbal Responds to painful Unresponsive Glasgow Coma Scale (GCS) score Designed for trauma, TBI Still is a reproducible, systematic scale Delirium: AMS, inappropriate, wax/wane 5 17
 Alert. Responds to verbal. Responds to painful. Unresponsive. Glasgow Coma Scale (GCS) score. Designed for trauma, TBI. Still is a reproducible, systematic scale. Delirium: AMS, inappropriate, wax/wane")
36
Neurologic Exam: Cranial Nerves
Cranial Nerves: Anterior vs. posterior? Anterior: CN, body deficits on same side Posterior: CN and body deficits are on opposite sides of the body (alternating hemiplegia) Face motor, sensory (LT) only Gag reflex (intubation) Eye Closure (Bell’s palsy) 5 17
 Face motor, sensory (LT) only. Gag reflex (intubation) Eye Closure (Bell’s palsy)")
37
Neurologic Exam: Eye Exam
Pupils: location of brain stem lesion EOM: CN palsies, often not due to CVA Vertigo: assists with DDx of CVA 5 17

38
Neurologic Exam: Motor
Motor: upper & lower extremities Upper: Pronator drift, hand grasp Lower: Leg lift, foot push on hand 5 17

39
Neurologic Exam: Sensory
Sensory: Light touch OK, pinprick ?? No other sensory testing is indicated unless a posterior circulation infarct or a spinal cord syndrome is suspected No heat, vibration, proprioception 5 17

40
Neurologic Exam: Reflexes
Suggest UMN control of LMN Corneal, gag, DTRs all are normal Pathologic reflexes Babinski, Chadduck Clonus Unclear whether or not these add to our overall impression of CVA severity 5 17

41
Neurologic Exam: Cerebellar
Truncal ataxia perhaps useful Ataxic gait, Rhomberg: No Extremity tests not useful in paralysis Past-pointing Hand alternating movements 5 17

42
Neurologic Exam: Visual
Visual field deficit Homonomous hemianopsia Neglect of one side Preferential gaze 5 17

43
Neurologic Exam: Language
Dysarthria: Poor speech, motor dysfunction Aphasia: Disturbed language processing Expressive: can’t speak Receptive: can’t process the spoken word 5 17

44
Acute Neurologic Exam Answers
The Hx should lead to a provisional Dx. The Px exam should detect co-morbidity and suggest the stroke etiology. The neuro exam should confirm the Dx. Few exam findings specifically direct Rx or direct outcome. AMS, coma are the most important findings. The NIHSS directs your neuro exam. Standardization of your document is key. 54 4 54

45
Acute Ischemic Stroke H & P: Some Practical Answers
The exam directs us to a provisional Dx. We do localize the lesion by identifying the provisional stroke syndrome. The CT will identify a large ICH or ischemic stroke, but many times the CT is negative, in which case the exam is key. Completing all parts of the neuro exam is not necessary, use it to confirm your Dx. 5 17

46
Neuro Exam: Internet Sites
Search engine: Google Key words: Neurologic Exam Some web sites: medicine/StrokeSSM/ClinExamNeuro.htm 5 17

47
Neurologic Exam: NIH Stroke Scale
13 item scoring system, 7 minute exam Integrates neurologic exam components CN, motor, sensory, cerebellar, visual, language, LOC Maximum score is 42, signifying severe stroke Minimum score is 0, a normal exam Scores greater than are more severe 5 17

48
NIH Stroke Scale: Important Questions
Which elements are consistently collected? Which correlate with outcome? Which improve with tPA? Which suggest a complicated tPA course? Which parts overlap with one another? 5 17

49
NIH Stroke Scale: Practical Suggestions
Know the general categories of the NIHSS Let these 7 areas guide your exam Know how to score an approximate NIHSS Go to the web to score your exam fully 5 17

50
NIH Stroke Scale: Internet Calculator
Allows calculation on-line Will add values, provide total neurol/Residency/nihss.htm Other sites: 5 17

51
Neuro Exam in Stroke: Documentation
Know the key elements of provisional Dx Use Hx and Px to support your Dx Document pertinent positives, negatives State neuro exam in terms of the NIHSS 7 5 17

52
Neuro Exam in Stroke: Documentation
State exactly what you did CN: face motor- ok eye closure, mouth, tongue Cerebellar: no truncal ataxia with sitting State findings in terms of a clinical entity Weakness, aphasia c/w L anterior circ CVA Cerebellar findings not c/w cerebellar CVA 5 17

53
Neuro Exam Documentation: An Example from a Real Case (Hx)
Date: XXXX exam 57 yo male Per CFD, thru interpreter Pt was at friend’s house, attempted to stand up, could not due to weakness C/o mild headache now No trauma 5 17

54
Neuro Exam Documentation: An Example from a Real Case (Hx)
? Hx HTN ? Meds ? compliance No recent illness No other c/os The exact time of these events is not as of yet determined 5 17

55
Neuro Exam Documentation: An Example from a Real Case (Px)
Pt alert, NAD, VS noted Head: pup EOM OK + neglect of L visual field + mouth droop L + tongue dev to L + slurred speech Airway OK 5 17

56
Neuro Exam Documentation: An Example from a Real Case (Px)
Neck: supple, - bruit Chest: clear BSBE Cor: reg s Abd: soft, nt Ext: nt Neuro: 5 17

57
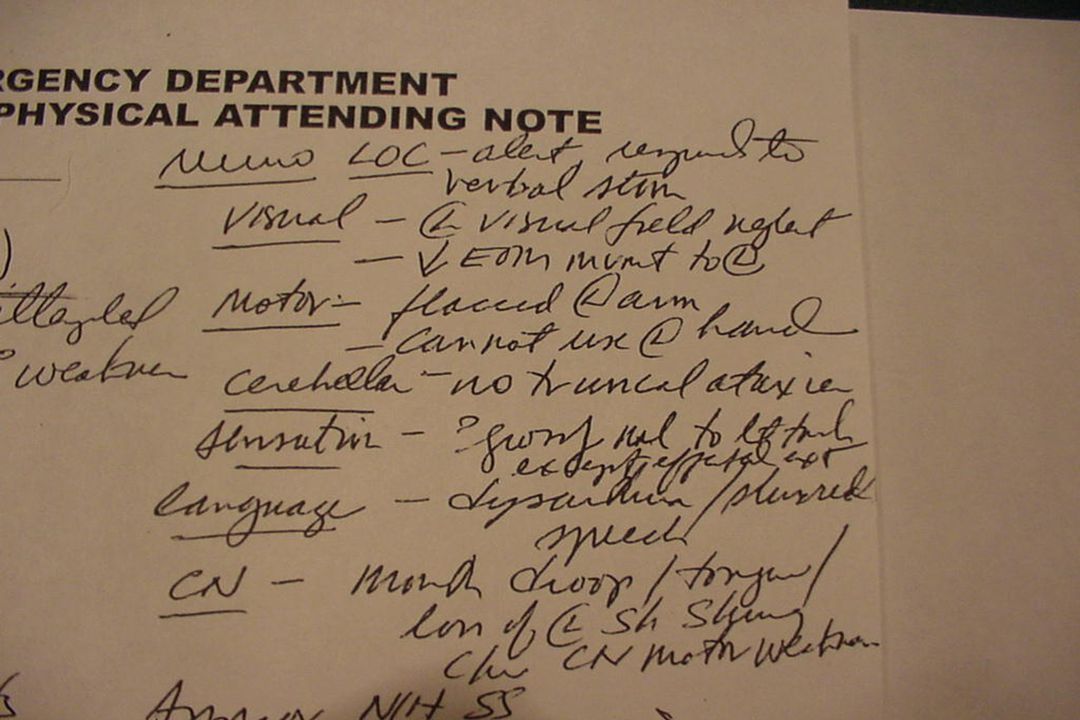
Neuro Exam Documentation: An Example from a Real Case (Px)
LOC: alert, responds to verbal stim Visual: L visual field neglect, dec EOM to L Motor: flaccid L arm, no use of L hand Cerebellar: no truncal ataxia Sensation: ? grossly nml to light touch except affected extremity Language: Dysarthria, slurred speech CN: mouth droop/tongue/loss of L sh shrug c/w CN motor weakness 5 17

58
Neuro Exam Documentation: An Example from a Real Case (Px)
Approx NIHSS: LOC 0 visual 2 CN 2 motor 3 Sens 1 neglect 1 Dysarthria 1 language 1 Approx total: 11 5 17

59
Neuro Exam Documentation: An Example from a Real Case (MDM)
Plan: w/u, including CT Neuro consult Contact witness to det exact time of sx onset Imp: Acute CVA with L sided sx Dx: CT shows parietal bleed Will Rx per neurosurg, admit ICU, stable 5 17

62
tPA in Acute Ischemic Stroke: Clinical & Documentation Issues
Document that tPA was considered If not used, state explicitly why the pt did not meet criteria or why it was deferred When explaining, tell the four key points: 30% greater chance of good outcome 10 fold greater risk of bleeding Same mortality rate, despite bleeding risk Explain why mortality is comparable 54 44 54

63
Clinical Case: Physical Exam
On exam, BP 116/63, P 90, RR 16, T 98, and pulse oximetry showed 99% saturation. The patient appeared alert, and was able to slowly respond to simple commands. The patient had a patent airway, no carotid bruits, clear lungs, and a regular cardiac rate and rhythm. The pupils were pinpoint, and there was neglect of the R visual field. There was facial weakness of the R mouth, and R upper and lower extremity motor paralysis. DTRs were 2/2 on the left and 0/2 on the right. Planter reflex was upgoing on the right and downgoing on the left. The patient’s estimated weight was 50 kg. 54 3 54

64
Acute Ischemic Stroke: Case Management
Complete directed H&P, with neuro exam Get the CT scan ASAP Call PMD, family, neurologist Find out the CT results Decide risk/benefit Discuss with pertinent decision makers 54 44 54

65
Acute Ischemic Stroke: Clinical Case: CT Results
54 44 54

66
Acute Ischemic Stroke: Clinical Case: CT Results
54 44 54
67
Acute Ischemic Stroke: Clinical Case: ED Management
CT: no low density areas or bleed No clear contra-indications to tPA NIH stroke scale: Neurologist said OK to treat No family to defer tPA use tPA administered without comp 54 44 54

68
Acute Ischemic Stroke: Clinical Case: tPA & Repeat Exam
tPA dosing: 8:21 pm, approx 1’45” after CVA sx onset Initial bolus: 5 mg slow IVP over 2 minutes Follow-up infusion: 40 mg infusion over 1 hour Repeat exam at 90 minutes: Repeat Px Exam: Increased speech & use of R arm, decreased mouth droop & visual neglect Repeat NIH stroke scale: 14-20 54 44 54

69
Acute Ischemic Stroke: Hospital Course & Disposition
Hospital Course: No hemorrhage, improved neurologic function Disposition: Rehab hospital Deficit: Near complete use of RUE, speech & vision improved, some residual gait deficit

70
Neurologic Exam in Stroke: Conclusions
The exam can and should be streamlined Focus on the provisional Dx Attempt to determine etiology, Dx, Rx Document in a brief, systematic manner State exactly what you did, how the findings relate to your provisional Dx and Rx 54 45 54

71
Neurologic Exam in Stroke: Recommendations
Know syndromes, focus neuro exam Learn to calculate an approximate NIHSS Document completely, but streamline Generalize this to process to your care of patients with other neuro emergencies Optimize outcome and your practice 54 46 54

72
Questions?? Edward Sloan, MD, MPH edsloan@uic.edu 312 413 7490
54 1 54
Similar presentations


 in Emergency Department Patients with Acute Stroke Edward Sloan, MD, MPH Professor Department of Emergency Medicine.>")















?>")

