Download presentation
Presentation is loading. Please wait.

1
Testicular tumors Mostafa El- Haddad

2
Anatomie Blood Supply? Lns distribution:
Cross over from Rt to Lt but not from Lt. to Rt. Scrotal Lymphatic's disruption.

3
Epidemiology Age: 20-35ys. Seminoma patient is older.
Don’t forget that yolk sac tumor can occur in children. Where? Social problem.

4
Etiology and Risk Factors
Intrauterine exposure to Estrogen. Un-descended testis: intra-abdminal > inguinal. Family history : very important. AIDS: RPL and stage is difficult to predict. Stage for stage is ok. Or c h id o p e x y d o e s n o t r e d u c e r i s k i n al l a g e g r o u ps b u t f a c i l i t a t e s e x a m i n a t i o

5
Intratubular neoplasm? How we detected?
Present in the contralateral testis in 10%. Bilateral testicular tumor do exist.

6
Pathology Germ Cell tumors. Supporting Cell tumors. Lymphoma.
Metastasis including sanctuary site.

7
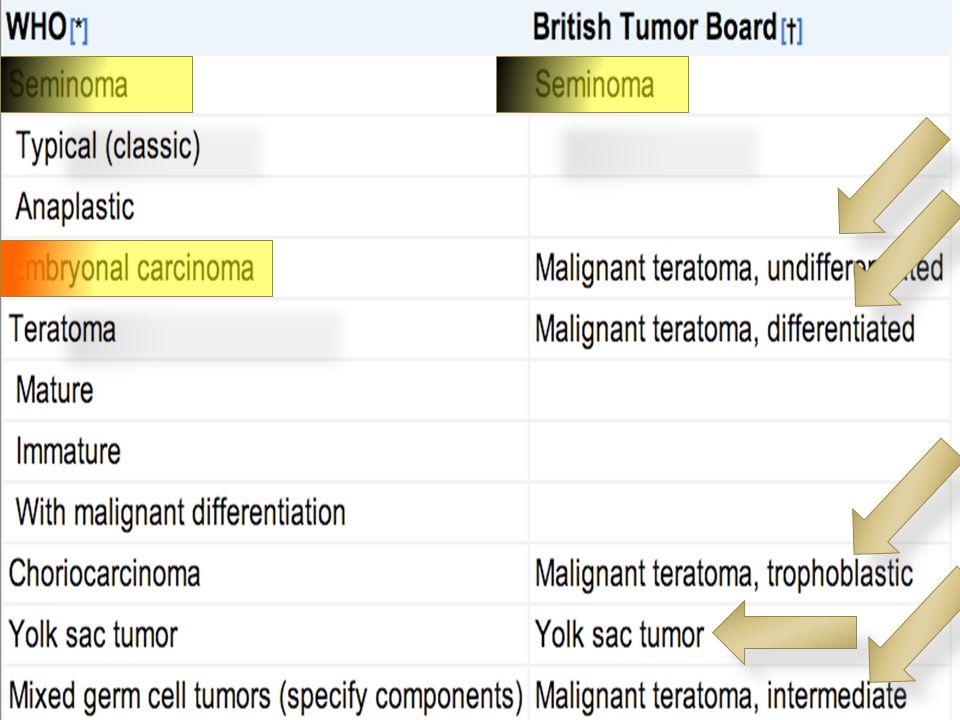
WHO Classification And British Testicular Tumor Panel and Registry

9
Mixed Germ Cell Tumors Are Considered NSGCT

10
Isochromosome 12 What is isochromosome? Value?
Pathognomonic feature of GCT of all histologic types, whether of gonadal or extragonadal origin. Can be an early marker (reported in insitu tumors). The presence of three or more copies of i(12p) has been correlated with poor prognosis GCT.
. The presence of three or more copies of i(12p) has been correlated with poor prognosis GCT.")
11
Natural History Seminoma associated with more ureteric obstruction?
NSGCT is more aggressive go blood.

12
RT LT

13
Other Lymph Nodes External Iliacs Obturator. Inguinal .
can occur in the external iliac and obturator nodes if the primary tumor invades the epididymis or extends up the spermatic cord, or in inguinal lymph nodes if the tumor extends through the tunica vaginalis to involve the scrotum, or if trans-scrotal exploration has been used.[29]

14
Spermatocytic Seminoma
Sixth decade. Bilateral more. Indolent course. Treatment surgery. -ve PLAB Spermatocytic seminoma represents approximately 5% of all seminomas and warrants special consideration. It generally occurs in the sixth decade. Although it is more likely to be bilateral than typical seminoma (6% vs. 2%), it is nonetheless a fairly indolent malignancy in which metastatic events are distinctly uncommon. Spermatocytic seminoma can be histologically distinguished from classic seminoma by the relative lack of compartmentalization of sheets of cells by fibrous septae, by the marked variation in cell size, and by the absence of lymphocytic infiltration.
, it is nonetheless a fairly indolent malignancy in which metastatic events are distinctly uncommon. Spermatocytic seminoma can be histologically distinguished from classic seminoma by the relative lack of compartmentalization of sheets of cells by fibrous septae, by the marked variation in cell size, and by the absence of lymphocytic infiltration.")
15
Anaplastic Seminoma

16
Intratubular Germ cell Neoplasia
Precursor but not for SS: Found in high risk group. Found adjacent to cancer. 50% risk to transform at 5 years. 100% risk at 8 years. Treatment : Radiotherapy 18 to 20Gy.

17
Symptoms and Signs Pain: local, Back. Gynecomastia?
DD: testicular torsion, hydrocele, varicocele, spermatocele, and epididymitis

18
Markers and CT chest Abdomen and Pelvis
Suspicious Mass Testicular US Mass Orchiectomy Markers and CT chest Abdomen and Pelvis No Mass

19
Orchiectomy may occasionally be delayed in metastatic cases to control primary disease .
Orchiectomy should be done? When orchiectomy should not be done?

20
Staging and Risk Assessment

21
HCG HCG: alpha unit and beta unit.
prostate, bladder, ureteral, and renal cancers may show increase in B-HCG elevation. Spurious elevations have been noted in persons using marijuana. Cis-platinum-induced testicular atrophy in the remaining testis, resulting in lower levels of testosterone, with a compensatory hypersecretion of LH to stimulate Leydig cell secretion of testosterone. very high levels of LH may spuriously elevate measured HCG levels. When necessary, measurement of HCG levels 2 weeks after the administration of depotestosterone should rule out this possibility.

22
To Make Life More Complicated
Neuroendocrine tumors and cancers of the bladder, kidney, lung, head and neck, GI tract Specifically gastric, pancreatic, biliary, and colorectal cancers, cervix, uterus, and vulva.

23
In addition, there are case reports of elevations in hCG in lymphoma and leukemia.

25
HCG produced by Scincytiotrophoblast.
Seminoma can produce HCG 5-40% of cases. Not more than 100 IU.

26
AFP 3 H Pregnant women (Hamel). Hepatitis. Hepatocellular carcinoma.
Similarly, elevations of AFP are typical of hepatocellular carcinoma and certain benign liver diseases and may be seen in gastric and, rarely, in lung, colon, and pancreatic cancers.

27
LDH Gene that encodes LDH isoenzyme 1 maps to chromosome 12.
The serum level of LDH isoenzyme 1 has been shown to correlate with the number of copies of i(12p) in the tumor, a fairly specific genetic marker of germ cell malignancies. Furthermore, the presence of three or more copies of i(12p) has been correlated with a worse prognosis.
 in the tumor, a fairly specific genetic marker of germ cell malignancies. Furthermore, the presence of three or more copies of i(12p) has been correlated with a worse prognosis.")
28
Very Important Up to 30% of patients with early-stage non-seminomatous GCT will have normal serum markers, so the absence of marker elevation should not influence the decision to perform an orchiectomy. Eventhough markers should be done before and After Surgery.

29
PET-CT FDG-PET was unable to detect mature teratomas as well as lesions smaller than 5 mm in diameter. Not routinely used or recommended in initial staging. Can be used to differentiate between residual disease and fibrotic bands?

30
Other Investigations Brain imaging in Choriocarcinoma.
In patients with clear clinical examination and Elevated markers don’t forget to investigate the other testis.

31
ASCO Guidelines For the Use of Tumor Markers

35
Treatment

36
Stage I Seminoma 1- Observation When? Or 2- Radiotherapy When?
Orchiectomy PLUS 1- Observation When? Or 2- Radiotherapy When? 3- Chemotherapy What?

37
Chemotherapy in advanced Stage
BEP or EP Cisplatin is better than Carboplatin

38
Spermatic cord involvement necessitates a radiation field that covers the entire inguinal orchiectomy scar, whereas scrotal skin involvement mandates radiation to the hemiscrotum

39
Residual Disease Post Chemo
Less than 3 cm or more than 3cm. Post chemotherapy field of radiation??

40
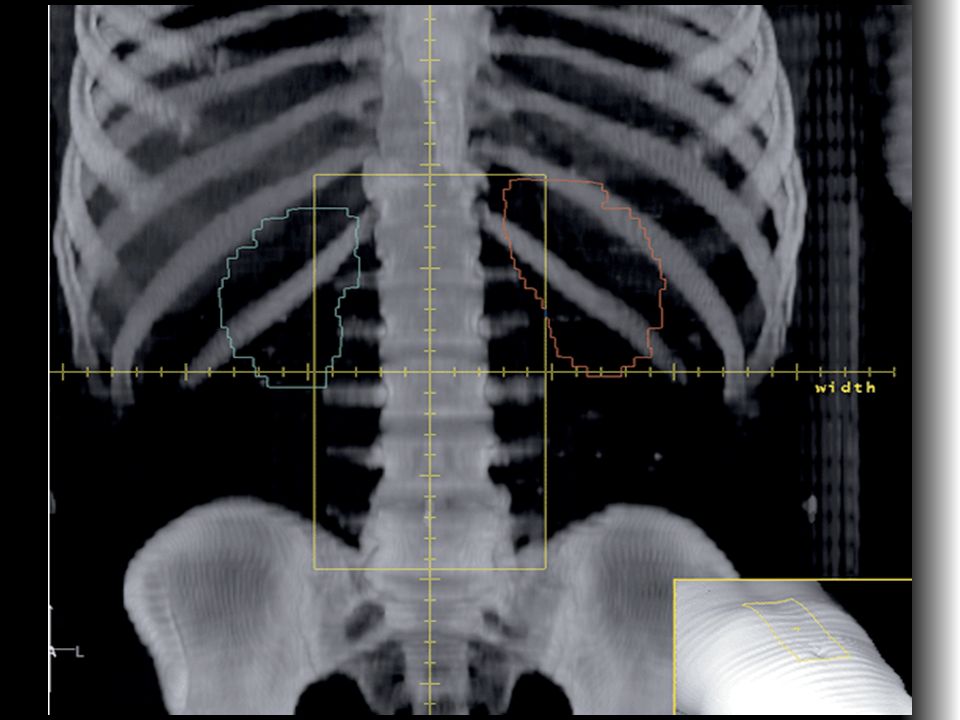
Radiotherapy Technique

41
Consent. Preparation. Positioning. Simulator. 30 degrees rotation of the remaining testis from the patient’s long axises.

44
Testicualt Irrdiation
Intratubular germ cell tumor. Testicular leukemia or lymphoma. Position is the Key. Penis. Beam arrangement. Energy: deep X- Electron, Photon. Bolus Where???

45
Technical consideration
Adjuvant radiotherapy to the hemiscrotum and ipsilateral inguinal lymph nodes is recom- mended. The scrotal field is matched to the tattoo at the inferior border of the dog-leg field.

48
Non Seminoma Vascular/lymphatic invasion
Embryonal carcinoma elements (>30%) Absence of yolk sac elements Absence of AFP preorchiectomy Less than 50% teratoma Local extension into paratesticular structures
 Absence of yolk sac elements. Absence of AFP preorchiectomy. Less than 50% teratoma. Local extension into paratesticular structures.")
Similar presentations



























; FRCS (Ireland); MMed (Wits); FCS (SA) Urology 38 th BMA CONGRESS.>")

