Download presentation
Presentation is loading. Please wait.

1
Anti-depressants vs Placebo Joan R. Shepherd, FNP
TIC TACS or TREATMENT Anti-depressants vs Placebo Joan R. Shepherd, FNP

2
Objectives Estimate the relative benefit of medication vs placebo across a wide range of initial symptom severity in patients diagnosed with depression Recognize current standard of care/medications for selected mood disorders

3
Objectives Consider alternative tools for use in primary or acute care setting ACT--Acceptance and Commitment Therapy Thought Work--Byron Katie Self-Coaching Model--Brooke Castillo Change Cycle-- Martha Beck, PhD.

4
Higher standard of living than ever before
Medical treatment Food Housing Sanitation Money Welfare Access to education Justice Travel Entertainment Career opportunities

5
Harris, R. 2008. The Happiness Trap, Exisle Pub.Ltd
Depression 13.1 to 14.2 million American adults in any given year 1/10th of the adult population/week 32 million (one in five)at some point in their life Harris, R The Happiness Trap, Exisle Pub.Ltd
at some point in their life. Harris, R The Happiness Trap, Exisle Pub.Ltd.")
6
World Health Organization
4th biggest, costliest most debilitating disease in the world By 2020, 2nd biggest Harris, R The Happiness Trap. Exisle Pub. Ltd.

7
only 50% of depressed people seek and receive adequate treatment
Mostly treated by PCP Fitzgerald Health Education Assoc. 2007

8
DSM IV Criteria at least 5 symptoms in the same 2-week period
Sleep: insomnia or hypersomnia, staying asleep problematic Interest: depressed mood, loss of interest or pleasure Guilt; feelings of worthlessness Energy: fatigue Concentration: diminished ability to think or make decisions Appetite: weight change, loss of food enjoyment Psychomotor: agitation or retardation Suicide: recurrent thoughts of death; passive, without plan

10
PCPs will not use a screening tool that’s more than 4 questions long!
Sally Miller, PhD. NCNP Conference 2007

11
PHQ-2 In the last 2 weeks, have you felt down, depressed, or hopeless?
In the last 2 weeks, have you felt little interest or pleasure in doing things? 96% Sensitivity, less Specificity Positive response should lead to PHQ-9:download at accessed

12
Kirsch et al 1998 1998 analysis of 38 manufacturer-sponsored studies of 3000 depressed patients Patients did improve This formed the basis for the claim that anti-depressants work

13
Studies Impact? The number of Americans taking anti-depressants doubled in a decade 13.3 million in 1996 27 million in 2005 National Patterns in Antidepressant Medication Treatment. Marcus and Olfson, Archives of General Psychiatry, 2005.

14
hmmmmmm… Comparing improvement in patients on ADM and placebo…
Placebo improved about 75% as much as those on ADM or 3/4 of benefit from ADM is placebo

15
Clinical trials of antidepressants are difficult to design and conduct.
more than half of all recent clinical trials of commonly used antidepressants failed to show statistical superiority for the drug over placebo. This is not necessarily because of the ineffectiveness of the antidepressant, but rather because of an increased response to placebo. Kahn et al 2005

16
Symptom Severity Estimate the relative benefit of medication vs placebo across a wide range of initial symptom severity in patients diagnosed with depression

17
What affects outcome? Fournier et al 2010
Examined Kirsch and Kahn’s meta-analyses Looked at Baseline symptom severity Hamilton Depression Rating Scale

18
Hamilton Depression Rating Scale (HDRS)
Most widely used clinician-administered depression assessment scale. 17- items pertaining to symptoms experienced over the past week Originally developed for hospital patients Many variations since then

19
HDRS Scoring 0-7 normal or remission 8-13 mild depression
moderate depression severe depression > 23 very severe depression

20
Placebo Washout Most trials testing the effectiveness of psychotropic drugs begin with a placebo washout phase. Pill placebo administered in single blind fashion Improvement > 20% excluded from the trial prior to randomization

21
Kahn et al Hypothetically this technique rids studies of placebo responders before randomization of subjects to drug and placebo groups. In theory, this lowers the level of response to placebo in the study and magnifies the superiority of the response to medication.

22
Kahn et al An analysis of 10 years of research: the washout technique does not do what it was designed to do in antidepressant studies. Within placebo or drug groups neither measures of depression nor dropouts were affected by including a preliminary washout in the design.

23
Size Matters Kirsch: Only 1 of 35 studies comprised samples with mean baseline HDRS scores lower than 23 (very severe depression) Kahn: Minimum entry score 20 (severe or very severe)
")
24
71% of 503 depressed, treatment-seeking out patients had HDRS scores less than 22
Zimmerman, Posternak, Chelminski. 2002

25
Conclusion “The magnitude of benefit of antidepressant medication compared with placebo increases with severity of depression symptoms and may be minimal or non-existent, on average, in patients with mild or moderate symptoms.” Founier et al. Antidepressant Drug Effects and Depression Severity. 2010

26
Numbers, please The minimum baseline HDRS score needed to achieve a clinically meaningful ADM/placebo difference is approximately 28 Differences are negligible for lower baseline HDRS scores

27
Current Guidelines Provide information and support
Build a trusting relationship Explore treatment options Information appropriate to their level of understanding and range of treatments Comprehensive written info available Audio available National Guideline Clearinghouse. Depression: the treatment and management of depression in adults. Accessed 9/17/10

28
Principles for assessment
Comprehensive assessment that does not rely simply on a symptom count Consider degree of functional impairment and/or disability and duration of the episode

29
Anti-depressants: Which Ones?
“Multiple randomized trials of patients in the primary care setting have found similar efficacy for drug therapy and psychotherapy with no clear predictors of which treatment is best for individual patients.” Up To Date. Initial Treatment of depression in adults. 2010

30
ADM: How to Choose? which antidepressant less important than treating patients with medications that they can tolerate sufficient doses to achieve symptom remission

31
ADM: How to Choose: What has worked in the past?
-if it worked before, try it again Positive response in a first degree relative Less danger of overdose

32
ADM: How to choose? Most psychotropic medications used in the treatment of depression work via manipulating serotonin, norepinephrine, and/or dopamine

33
Serotonin “…a chemical of thought, movement and behavior, as well as digestion, ejaculation, and evacuation. The body’s all-purpose neurotransmitter, involved in sleep, mood, appetite…” Hanson, D The Chemical Carousel

34
Norepinephrine The ‘engergizer’, associated with focused attention
Motivation to win a reward Responsible for the “adrenaline surge” It is the brain’s “go” signal Also important in memory

35
Dopamine “Pleasure chemical” Linked to experiences of joy
Attention, movement, problem solving, anticipation of a reward Creates the desire to repeat a pleasant experience Hanson, 2008.

36
Most Bothersome Symptom?
Vegetative? Energized? Anxious?

37
SSRIs Selective serotonin or serotonin Specific reuptake inhibitors
Inhibit reuptake of 5H-T, so more serotonin at synaptic cleft

38
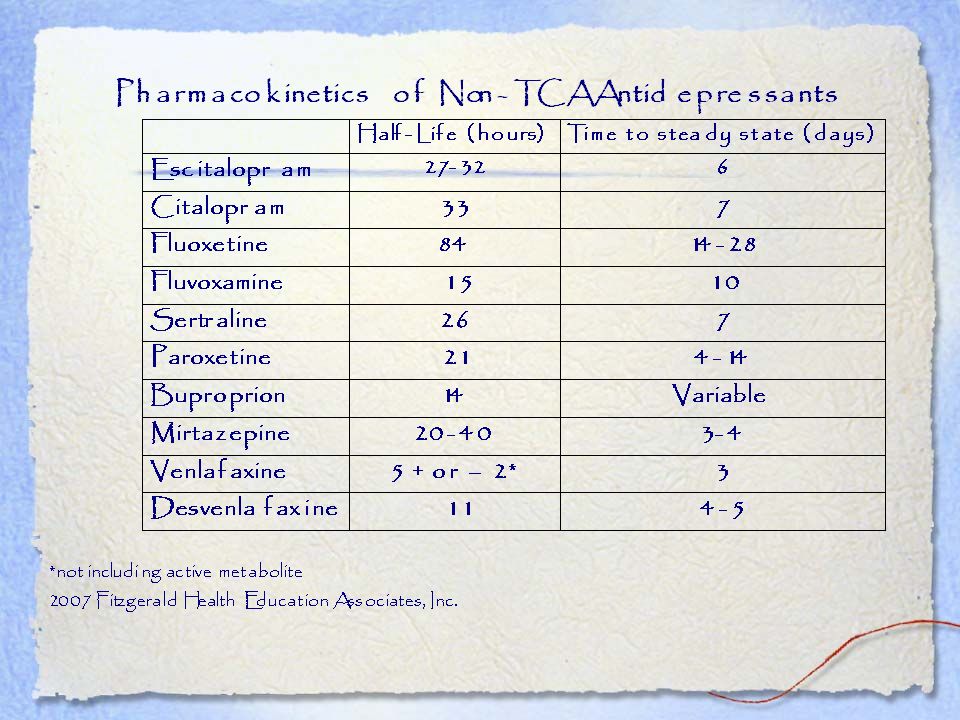
SSRIs Citalopram (Celexa) Escitalopram (Lexapro) Fluoxetine (Prozac)
Fluvoxamine (Luvox) Paroxetine (Paxil) Sertraline (Zoloft)
 Paroxetine (Paxil) Sertraline (Zoloft)")
39
Differences among SSRIs…
Fluoxetine long half-life Less control Takes longer to be eliminated If patient discontinues drug, less likely to have side effects Minimizes withdrawal Poor compliance, misses doses

40
SSRI Differences Paroxetine
Drug holiday for sexual side effects bc relatively short 1/2 life Better control Patient with better compliance

41
Adverse Effects: Maximize!
SE from agitating to sedating Fluoxetine: energizing and long acting Depressed patient without energy Vegetative patient Not for the very anxious patient Paroxetine: sedating and short acting Use in patient with depression w/insomnia High discontinuation from SE

42
Others? Intangible…some patients just do better with one than another for no apparent reason… Sertraline Post MI anhedonia Lower SE profile Pre-menstrual dysphoric disorder

43
Citalopram Escitalopram Substrate cytochrome P450 Mildly sedating
Good SE profile

45
SSRI Common adverse effects
Headache Usually controlled with acetaminophen Keep well hydrated May take 3-4 weeks to resolve

46
SSRI Common side effects
Associated with increased risk of bleeding, esp in older people or people taking other drugs that have potential to damage the GI mucosa or interfere with clotting Consider adding gastroprotective drug if on NSAID or ASA

47
SSRIs-Class Effects GI disturbance-often loose stools Nausea
Take with food Except paroxetine bc of anti-cholingergic effect Sertraline-lose 1/3 dose effect on empty stomach Nausea Take with food and adequate water Use at bedtime Consider adding short course of ranitidine (H2RA…not Tagamet) May take 3-4 weeks to resolve
 May take 3-4 weeks to resolve.")
48
SSRI Side Effects Weight gain after several weeks
Initially mild anorexia May lower seizure threshold Not usually clinically significant at normal doses But consider other meds that may have same effect

49
SSRI side effects Agitation
Reduce the dose by 25% and gradually reintroduce Trazaodone great for helping with sleep Sedating antidepressant Low abuse potential Onset of action = 1/2 - 1 hr Peaks 2-3 hr Full stomach will delay effect

50
SSRIs Fluoxetine, fluvoxamine and paroxetine associated with a higher propensity for drug interactions than other SSRIs Paroxetine is associated with higher incidence of discontinuation symptoms than other SSRIs

51
*LOW SODIUM* At the end of the presentation, a NP-PhD in psych approached me and told me I should share with the group that SSRIs can cause low sodium! I hadn’t heard that before…so please take note. Could be extremely important especially in the depressed population!

52
When effective? Try a medication for 4-6 weeks for beginning to see a response Trial of 3 months necessary for true response Then try another SSRI In 6 months, go to different class (SNRI, TCA…)
")
53
SNRIs Target norepinephrine (NE) and serotonin
2nd line agents, depending upon co-morbidities and symptom presentation Try for SSRI resistant depression

54
Venlafaxine Dose dependent Higher dose, higher BP
Consider for patient who presents with depression and chronic pain Menopausal symptoms-low dose Sallly Miller, PhD. NCNP Conference. 2007

55
Venlafaxine Greatest suicide risk of SNRIs
more likely to cause side effects that will cause patient to stop taking the med Consider increasing the doses gradually Higher doses can exacerbate cardiac arrhythmias

56
Duloxetine NE slightly lower doses Diabetic peripheral neuropathy
Urinary incontinence?

57
Desvenlafaxine Active metabolite of venlafaxine Approved for MDD
May cause more nausea, HTN May give with or w/o food Don’t divide, crush, chew or dissolve Matrix tablet-may see ‘ghost tablet’ in stool Cost for 30 days: $108.71 Prescriber’s Letter. Detail Document # Accessed 9/18/10

58
Bupropion Inhibits re-uptake of NE, dopamine Very activating
Contraindicated in patients with or at an increased risk of seizures Slight risk of arrhythmias

59
Mirtazapine-Remeron Noradrenergic antagonist-blocks presynaptic alpha-adrenergic 5HT2 Mildly anti-cholingergic Lots of sedation Weight gain Great GI profile

60
Trazodone-Desyrel Good for anxious depression Very sedating
‘Anxiety receptor site’ Blocks 5-HT2A, inhibits reuptake of 5-HT

63
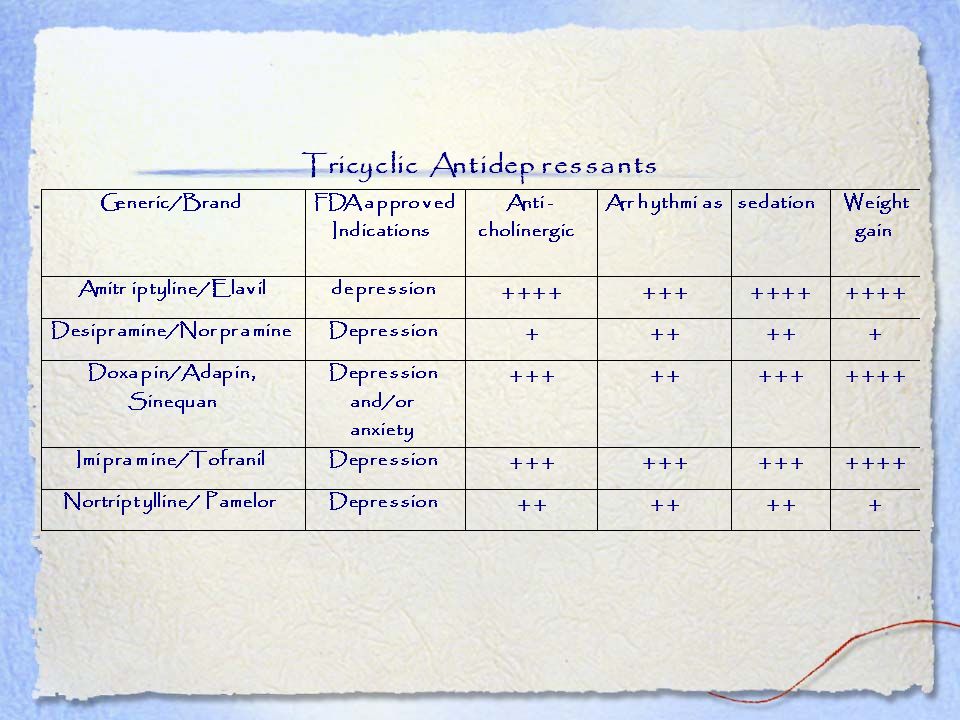
TCAs Dry mouth Blurred vision Constipation Urinary retention
Memory impairment Postural Hypotension Cardiac arrthythmias

64
Suicidality One of the main reasons TCAs are used less frequently now than SSRIs is because of how fatal they are in overdose. Thanks to the NP, PhD in psych who approached me after the talk to remind me of this fact! (Sorry, I don’t remember your name!).
.")
66
Tricyclics-unapproved but common uses
Amitriptyline commonly used for bulimia nervosa and neuralgias Norpramine-bulimia, panic disorder, premenstrual syndrome Contraindicated in acute recovery post MI Prolongation of QRS or QT and high doses

67
Common uses… Doxepin-depression and/or anxiety associated with alcoholism Pamelor-smoking cessation

68
Treatment Resistant Depression
Response: 50% reduction in symptoms Remission: almost complete absence of symptoms 8 week clinical trials only 35-40% achieve remission Goal: Remission Prescriber’s Letter Detail Document , accessed

69
Strategies: Dosage increase Switching antidepressant
Combining antidepressants Augmentation with non-antidepressant

70
Assessing Response Earliest:
Increased interest and pleasure in activities Improvements in psychomotor retardation 3-4 weeks with no response or 6 weeks with partial response despite adherence, consider diagnosis reassessment or change therapy

71
Dose Optimization Increase dose if tolerated
Esp for partial responders Consider after 2 weeks If no response, consider med change

72
Switching ADM 4-8 weeks after dose optimization with no response or partial response Achieves remission about 25% time Can stay in the same class

73
STAR*D Trial Patients who didn’t respond to citalopram were just as likely to respond to sertraline as as to extended release venlafaxine or sr bupropion

74
Taper paroxetine and venlafaxine to prevent withdrawal
Fluoxetine-consider a 4-7 day washout when switching due to long T-1/2 Failing two SSRIs, consider a different class Consider co-morbidities Pain-SNRI or TCA Anxiety, agitation, insomnia-mirtazapine SSRI induced sexual SE-add bupropion, mirtazapine

75
Combining Antidepressants
Avoids risk of withdrawal symptoms and loss of benefit from 1st ADM Drug 2 may counteract Drug 1’s Ses Most common combo is Bupropion plus SSRI SSRI plus TCA Keep TCA low range (25-75mg) bc SSRI can increase TCA levels
 bc SSRI can increase TCA levels.")
76
Combining ADMs Trazodone (Desyrel) mg plus SSRI or venlafaxine for sedating effect Trazadone plus fluoxetine or paroxetine can inhibit the elimination of trazodone’s metabolite, leading to CNS stimulation

77
Combining ADMs Mirtazapine/SSRI, bupropion, or venlafaxine has showed improvement Little data Consider for patients with nervousness, insomnia or sexual side effects

78
MAOI’s Combinations can cause life threatening serotonin syndrome or hypertensive crisis Leave to the specialists!

79
Data does NOT support combining venlafaxine with other SSRIs
Or combining two SSRIs.

80
Augmentation with Non-ADM
Treat concomitant conditions Improve specific symptoms Quick onset of other meds Buspirone (BuSpar) Improves SSRI-induced sexual Ses Good choice for depressed patients with anxiety
 Improves SSRI-induced sexual Ses. Good choice for depressed patients with anxiety.")
81
Aumentation with non-ADM
Atypical Antipsychotics Used with SSRI improve NE and serotonin release through blockade of 5-HT2A receptors Improvements in sexual function and sleep Likely effective at lower doses than schizophrenia, minimizing SEs

82
Augmentation with Atypical Antipsychotics
Aripiprazole (Abilify)-add-on treatment for MDD in adults Starting dose when adding to ADM is 2-5mg Can increase by 2-5mg weekly Maximum 15mg/day SE: akathisia, restlessness, insomnia May help to add mirtazapine for akathisia
-add-on treatment for MDD in adults. Starting dose when adding to ADM is 2-5mg. Can increase by 2-5mg weekly. Maximum 15mg/day. SE: akathisia, restlessness, insomnia. May help to add mirtazapine for akathisia.")
83
Symbyax-combination fluoxetine/olanzapine
treatment of bipolar depression and derpession in patients who have failed 2 ADM of sufficient dose and duration Starting dose 6/25 QHS Caution: hypotension, hepatic impairment Most common adverse effects: Weight gain Increased appetite Dry mouth Sonmolence Fatigue

84
Quetiapine (Seroquel, Seroquel XR)
Treatment resistant depression Dose qhs 50mg day one and two, then 150mg daily Watch lipids, weight gain, diabetes, tardive dyskinesia! Use lowest effective dose for shortest duration When switching, start Seroquel XR while tapering ADM

85
Atypical Antipsychotics
Glucose monitoring Check fasting glucose in patients who develop symptoms of dibetes Baseline fasting glucose Periodically in patients with risk factors Metabolic effects Risk of sudden cardiac death Black box warning re Suicidality

86
Augmentation con’t Risperdal and Geodon also being studied
Lamotrigine (Lamictal) mood stabilizer improves several symptoms of depression: Mood, lack of interest, decreased energy, impaired cognition SE: dizziness, headache, nausea, sleepiness Like lithium, may be good adjunct for patients with bipolar
 mood stabilizer. improves several symptoms of depression: Mood, lack of interest, decreased energy, impaired cognition. SE: dizziness, headache, nausea, sleepiness. Like lithium, may be good adjunct for patients with bipolar.")
87
Lithium Improves depression with poor response to TCIs
Efficacy with SSRIs not so good-both serotonergic Serum concentration monitoring Adverse effects (weight gain, tremor) Serotonin syndrome
 Serotonin syndrome.")
88
71% of 503 depressed, treatment-seeking out patients had HDRS scores less than 22
Zimmerman, Posternak, Chelminski. 2002

89
Depression is never an accident; it is perfectly designed to tell you something important about how your life is going.

90
Therapeutic listening skills….
Tools to take home!

91
Thought Work Acceptance and Commitment Therapy Byron Katie
Brooke Castille Martha Beck, PhD.

92
Thought Work The technique of stepping back, becoming the Compassionate Watcher of my thoughts. Becoming aware of the stories I am Telling Myself. Realizing: I am a Person who has thoughts…I am not my thoughts.

93
Acceptance and Commitment Therapy
Grew out of Cognitive Behavioral Therapy Examines the role of language and thoughts in suffering Based on the assumption that most unwanted internal experiences cannot be eliminated or controlled, so they must be accepted.

94
Valued Actions Heavy emphasis on values-based living
Knowing one’s sense of direction dignifies one’s experiences

95
Lizard Fears Human brain evolved for survival Lack or Attack fears
Lack: Not enough food, water, shelter, sex Attack: saber toothed tigers

96
Top 10 Lizard Tunes Write them down Put them to music Twinkle twinkle
Happy birthday

97
Self-Coaching 101 Circumstance Thoughts Feelings Actions Results
Brooke Castillo

98
Self-Coaching Model Brooke Castillo
Circumstances: things that happen in the world, facts Thoughts: things that happen in your mind Feelings:not physical sensations, but emotional feelings in your body Actions: what we DO in the world Results: what we see in the world, the effect of our action

99
Circumstance: 57 yoAAf hx of HTN. Flat affect and various somatic complaints. Recent change in job responsibilities from working night shift in laundry room to more physical house-keeping. Thought: Evening shift people are slobs, they leave this place a mess, making my job so much harder. My supervisor doesn’t care…

100
SC 101 Feelings: anger, frustration, victimized, powerless
Actions: work with hostility, isolate from other workers, avoid supervisor Results: HTN increased, insomnia, dreads going to work, angry at home.

101
Being in the place of the watcher.
How are you reacting to your thoughts? How can you change your thoughts? Thoughts cause Feelings and you can change your thoughts. Regardless of circumstances, you can always change the thoughts.

102
The result of your actions caused by your feelings will always prove the original thought….brains compelled to gather evidence to support the original thought.

103
Result: HTN increased, insomnia, dreads going to work, angry at home.
Will always prove the original thought: “This job is killing me…The evening shift people are slobs. They leave this place a mess, making my job harder…my supervisor doesn’t care…”

104
Intervene at level of THOUGHT.
Notice your thoughts about the circumstance. Change the thought to something that feels slightly better, or flip it around. This will give you the power to change your feeling about the circumstances.

105
In the moment of asking, “what am I thinking
In the moment of asking, “what am I thinking?” you assume the position of the watcher. This process alone can create new wiring, allows a person to make conscious decisions and a feeling of control.

106
How to change the thought?
a full thought turnaround slightly better thought Write down the painful thought Write down the feeling the thought is causing Try to find a slightly better-feeling-thought you know is true…

107
they’re sloppiness is job security for me
Maybe the shift before them left them a mess I can ask my supervisor to keep me in mind the next time there’s an opening It’s kind of satisfying to make the room look nice I’m getting a little exercise I can imagine that it’s my Mother’s room in her nursing home

108
SC 101 Example 2 24 yocm recently completed detox from methadone
Circumstance: No GF Thought: I deserve one. Look at all the losers with GFs. I can’t get one. Feelings: loneliness, frustration, desperate Actions: Passing cards out to people with his number. Avoiding actually speaking to girls. Watching others with contempt. Result: No GF. Depressed, isolating.

109
Change the Thought New Thought: It’s highly likely I’m going to meet girls now that I’m in recovery. I’ve got a lot more to offer. Feelings: hopeful, peaceful, less desperate Actions: discuss with counselor, observe relationships that seem to be working, read helpful books. Focus on your recovery Result: more confidence, willing to speak to a girls without expectations of liason

110
Thought Work or Inquiry Byron Katie
Suffering Thought Is it true? Can you absolutely know it’s true? How do you react when you think this thought? Who would you be without the thought? Turnaround

111
Inquiry/The Work 36 yoAAm incarcerated 8 years. Productive Citizen class, be out in next couple months. Resentments. Painful Thought: My mother shouldn’t have given me away Is that true? Can you absolutely know it’s true? She couldn’t care for me

112
Who would I be without this thought?
Believe a woman could love and stay with me Not feel so angry toward my mother Build a relationship with her

113
Turnaround: Opposite, Self, Others
1. My mother should have given me away Couldn’t care for me Great act of love Opened doors for me 2. I shouldn’t have given myself away betrayed myself, not honoring myself, ending up in prison

114
3. I shouldn’t have given my mother away:
I’ve given away my relationship with her because I’ve been so hurt and angry

115
38 yo morbidly obese cf chronic lymphedema, depression, anxiety
38 yo morbidly obese cf chronic lymphedema, depression, anxiety. Years earlier had witnessed her mother’s death after long illness.

116
Limiting Belief/Painful Thought: “I wasn’t there for my mother.”
Is that true? well… 2. Can you absolutely know it’s true? 3 reasons why it might NOT be true -sat up together many nights talking, laughing -put off going to college -responsible for her meds

117
3. How do I react when I’m having this thought?
-stuck -undeserving -sad, trapped 4. Who would I be without this thought? -free -light -making plans for school

118
Turnaround statement:
1. Opposite: I was there for my mother. 2. Self: I wasn’t there for me. 3. Other: My mother wasn’t there for me. Provide evidence for each statement, without forcing it. Is there a thought that is more true for you?

119
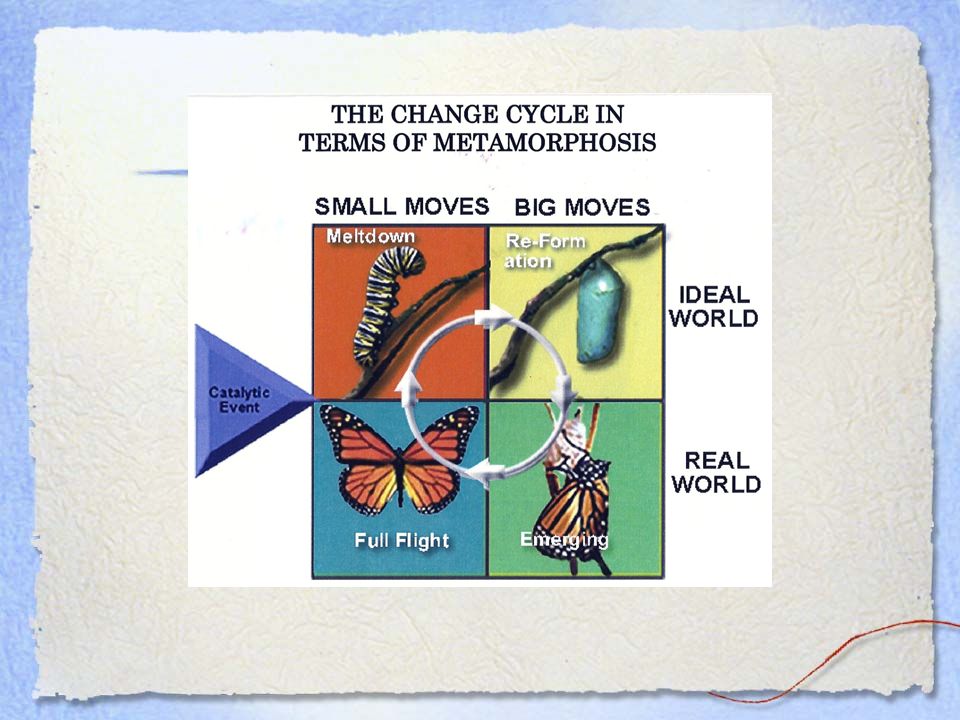
The Change Cycle Dr. Martha Beck, PhD

121
48 yocf in long term relationship presents with somatic complaints
48 yocf in long term relationship presents with somatic complaints. Feeling ‘out of sorts’, distracted, sleeping problems. Little interest and pleasure in doing things. Recently paid off mortgage.

122
Catalytic Event: Joyful event/transition
Paying off the mortgage threw her into Square One. Redefinition of self. Not the “starving artist” anymore. Look at the story, look at the thoughts. May need to go through a grieving process.

123
Yeeha! Hello Square Two--Dream and Scheme!!

124
56 yocm was a body builder by hobby
56 yocm was a body builder by hobby. Seven years earlier severely injured his back while working out. Had surgery and was on daily high dose opiates til he came for AOD. Felt great physically, but at 1 month f/u stated he’d “never been more depressed in his entire life”.

125
Catalytic Event: Back Injury, traumatic event threw him into the Change Cycle.
Had not gone through a grieving process to allow transition into square 2: Dream and Scheme. Follow up visit 1 month-making plans to return to school. Family life much improved.

126
Depression is never an accident; it is perfectly designed to tell you something important about how your life is going.

127
Grazi!!

129
Beck, Martha. Life Coach Training Handbook. 2008.
Castillo, Brooke. Self-Coaching 101, Fournier, DeRubeis et al. Antidepressant Drug Effects and Depression Severity: A Patient-Level Meta- analysis. JAMA 2010; 303 (1):47-53 Hamilton MA. A rating scale for depression. J Neurol Neurosurg Psychiatry. 1960;23:56-62. Hyman, Mark. “Why Antidepressants Don’t Work for Treating Depression”
: Hamilton MA. A rating scale for depression. J Neurol Neurosurg Psychiatry. 1960;23: Hyman, Mark. Why Antidepressants Don’t Work for Treating Depression")
130
Katie, Byron Kathleen. http://www.thework.com/index.php
Lee S, Walker JR, Jakul L, Sexton K. Does elimination of placebo responders in a placebo run-in increase the treament effect in randomized clinical trials? A meta-analytic evaluation. Depress Anxiety. 2004; 19(1):10-19. National Guideline Clearing House, Depression. The treatment and management of depression in adults
: National Guideline Clearing House, Depression. The treatment and management of depression in adults")
131
Strosahl, K. and Robinson, P. The. Mindfulness. and Acceptance
Strosahl, K.and Robinson, P. The Mindfulness and Acceptance Workbook for Depression, 2008.

Similar presentations











 Anticholinergic.>")











