Download presentation
Presentation is loading. Please wait.

1
University of California, San Diego
Overview of Quality Improvement Focus on Designing Reliable Interventions Greg Maynard MD, MS Professor of Clinical Medicine and Chief, Division of Hospital Medicine University of California, San Diego

2
Quality Improvement: Bridging the Implementation Gap
Scientific understanding Progress Time Implementation Gap Patient care So we start out by noticing an area of focus. This focus for quality improvement projects should develops from recognition of a gap between the level of care that is optimal and best supported by the evidence contrasted with the care that is actually being delivered to our patients. We are all here today because we know that management of hyperglycemia in the hospital is one of these areas. What is actually being done, is far from what is supported in the literature. How do we ultimately bridge that gap? It can be accomplished by using qi principles and following steps that have been determined to be essential by those who have gone before you.

3
Working harder isn’t always the answer……

4
The Evolving Culture of Medicine
20th Century Characteristics Autonomy Solo Practice Continuous learning Infallibility Individual Knowledge 21st Century Characteristics Teamwork & systems Group practice Continuous improvement Multidisciplinary problem solving Change Shine, KI. Acad.Med. 2002;77:91-99

5
How Do We Close the Gap? Essential Elements
Institutional support and multidisciplinary teams Standardized order sets Infusion Subcutaneous which promote basal / bolus regimens Algorithms / protocols / policies Address dosing Nutritional intake Special situations: TPN, enteral tube feedings, perioperative insulin, steroids Safety issues Transitions in care and discharge planning Metrics: How will you know you’ve made a difference? Comprehensive educational program

6
Traditional Quality Assurance
Focus on the statistical outliers in the ‘tail’ Faulty assumption: Care not in the ‘tail’ must somehow be acceptable and needs no improvement Focus on intervention for a few individuals Little focus on process improvement No potential for breakthrough improvement even if complete success in getting rid of outliers Event related - reactive outliers

7
Quality Improvement Before After Quality Quality better better worse
Focus on processes of care, not just outliers Improvement in processes reduces variation and shifts entire curve toward better care Potential for radical change through changing the design of care Really bad apples now isolated for picking! Goal related - proactive better Quality worse better Quality worse

8
Quality Improvement is… Focus on processes of care
Reduced variation by shifting entire practice A change in the design of care Quality Improvement is NOT… Forcing people to work harder / faster / safer Traditional QA or peer review Creating order sets or protocols without monitoring use or effect …not just the outliers …shifting entire practice toward better care by process change …potential for radical change through changing the design of care …Yelling at people to work harder / faster / safer

9
Good Teamwork is Essential

10
Features of a Good Team Safe Inclusive Open Consensus seeking
no ad hominem attacks Inclusive open to all potential contributors values diverse views; not a clique Open considers all ideas fairly Consensus seeking finds a solution all members can support

11
Models for Improvement
In use around the globe for decades Success in many fields of endeavor Healthcare late to the game! Alternative to the usual: Predictable breakdowns in reliability leading to common problems Ignoring improvement concepts & trying the first thing that comes to mind Not measuring effectiveness of implementation outcomes or process until bad events happen…..again

12
A Model for Improvement
Setting Aims Improvement requires setting aims. The aim should be time-specific and measurable, with a defined population. Establishing Measures Teams use quantitative measures to determine if a specific change actually leads to an improvement. Selecting Changes All improvement requires making changes, but not all changes result in improvement. Organizations therefore must identify the changes that are most likely to result in improvement. Testing Changes The Plan-Do-Study-Act (PDSA) cycle is shorthand for testing a change in the real work setting — by planning it, trying it, observing the results, and acting on what is learned. This is the scientific method used for action-oriented learning.
 cycle is shorthand for testing a change in the real work setting — by planning it, trying it, observing the results, and acting on what is learned. This is the scientific method used for action-oriented learning.")
13
Features of Good Aim Statements
Specific Measurable Aggressive yet Achievable Relevant Time-bound

14
Sample Aim Statements:
Glycemic Control on the Wards Within 6 months the use of sliding scale only regimens will be reduced by half. Within 12 months the % of patients with POC glucose testing achieving a mean glucose of < 200 mg/dL will improve from 65% to 85%. Within 12 months the % of our patients suffering from hypoglycemic events will be reduced from 11% to 6%.

16
Measurement Principles
Seek usefulness, not perfection Integrate measurement into daily routine Use qualitative and quantitative data Use sampling Plot data over time Use a balanced set of measures for all improvement efforts

17
A Blend of Measures Structure Process Outcomes
Do you have a multidisciplinary steering committee? Do your SQIO sets include a prompt for A1c? Process % of SQIO written using your order form % with basal insulin Outcomes LOS, Mortality: Glycemic control, Hypoglycemia

18
Picabo Street and Communication
Olympic Gold Medal Winner….AND a Critical Care Nurse!

19
“Picabo, ICU”

20
Hierarchy of Reliability
Predicted Success rate Level 1 No protocol* (“State of Nature”) Decision support exists but not linked to order writing, or prompts within orders but no decision support Protocol well-integrated (into orders at point-of-care) Protocol enhanced (by other QI and high reliability strategies) Oversights identified and addressed in real time 40% 50% 2 3 65-85% 4 90% 5 95+%
 Decision support exists but not linked to order writing, or prompts within orders but no decision support. Protocol well-integrated (into orders at point-of-care) Protocol enhanced (by other QI and high reliability strategies) Oversights identified and addressed in real time. 40% 50% % 4. 90% %")
21
Order sets w/ embedded insulin orders: Standardization?

22
High Reliability Design Solutions (as applied to Insulin Protocol)
Standardize insulin choices for common situations MD must “opt out” of default choices (not opt in) Prompts for basal insulin if over glycemic target, prompts for HgA1c, etc. Scheduled assessments of glycemic control / insulin regimen Redundant responsibility to maintain glycemic target STANDARDIZE: Choosing one preferred option for these situations is advantageous because: You can communicate preferred regimens more simply and succinctly to all staff. You eliminate all inappropriate choices for insulin regimens for that situation, as well as some other less preferred, but acceptable choices. You can encourage regimens that are most economical (by promoting the insulin regimens that reflect your hospital formulary choices). Staff members can become very familiar with a few regimens, instead of being confused by a multitude of them. They can identify variations from your preferred choices and target these patients for extra scrutiny and actions should they fail to meet glycemic targets. It lends itself to building protocols more than the inherent variability in usual practice.
 Prompts for basal insulin if over glycemic target, prompts for HgA1c, etc. Scheduled assessments of glycemic control / insulin regimen. Redundant responsibility to maintain glycemic target. STANDARDIZE: Choosing one preferred option for these situations is advantageous because: You can communicate preferred regimens more simply and succinctly to all staff. You eliminate all inappropriate choices for insulin regimens for that situation, as well as some other less preferred, but acceptable choices. You can encourage regimens that are most economical (by promoting the insulin regimens that reflect your hospital formulary choices). Staff members can become very familiar with a few regimens, instead of being confused by a multitude of them. They can identify variations from your preferred choices and target these patients for extra scrutiny and actions should they fail to meet glycemic targets. It lends itself to building protocols more than the inherent variability in usual practice.")
23
CAUTION!!!! Be Sure to Insert a Brain Between Protocol and Patient!
Education for broad range of providers Consider special team of focused providers

24
Engineering Change: Hints for Success
Empower nursing Expedite passage through medical staff committees Better to implement an imperfect, compromise change than no change at all Provide hot line or support for difficult situations Follow metrics continuously as you implement

25
Engineering Change: Hints for Success
Measure, learn, and over time eliminate variation arising from professionals; retain variation arising from patients Keep big picture in mind Negotiate ‘speed bumps’ Time delays in getting data Incomplete buy-in Go around obstacles instead of through them (can always go back to them later) Some who disagree with you may be correct Make changes painless as possible: make it easy to do the right thing
 Some who disagree with you may be correct. Make changes painless as possible: make it easy to do the right thing.")
26
PDSA: Plan-Do-Study-Act
The use of PDSA has been referred to as the “democratization of the scientific method.” (Paul Miles, MD) Do small scale tests of change. Everyone can do it! Act Plan Study Do Plan it Do it Check it Act on the results found - quickly
 Do small scale tests of change. Everyone can do it! Act. Plan. Study. Do. Plan it. Do it. Check it. Act on the results found - quickly.")
27
Benefits of rapid cycle change:
Increases belief that change will result in improvement Allows opportunities for “failures” without impacting performance Provides documentation of improvement Adapts to meet changing environment Evaluates costs and side-effects of the change Minimizes resistance upon implementation

28
Examples: integration of best practice
A1c level within last 30 days. Specify hyperglycemic diagnosis Each patient should have a glycemic target.

29
A1c Level Incorporate prompt for A1c level in insulin order sets and protocols. Ordering can be accomplished with checkbox Monitor performance, feedback to providers Glycemic control team obtains it

30
Proper diagnosis Diagnosis: Uncontrolled –or– Controlled
Diabetes type: 1 2 Gestational –or– Secondary to another cause;Specify –or– Stress/situational hyperglycemia Improves reimbursement: define “uncontrolled DM” and monitor coding accuracy Order set docmentation translates into ICD-9

31
Identify non-critical care glycemic target
Preprandial target 90–130 mg/dL; maximum random glucose < 180 mg/dL (ADA/AACE consensus target) 80–150 mg/dL Preprandial target 90–130 mg/dL for most patients, 90–150 mg/dL if hypoglycemia risk factors
 80–150 mg/dL. Preprandial target 90–130 mg/dL for most patients, 90–150 mg/dL if hypoglycemia risk factors.")
32
“Actionable” Glycemic Target
The “what” is common to all institutions: push for changes in regimens when glycemic target not being met. Variable by institution: Glycemic target definition How to generate report Who acts on report Putting this in place moves you up hierarchy of reliability. Opportunity to Learn from variation! What happens if your institution’s glycemic targets are not being met? Glucose values consistently out of your target range without attempts by physicians to tighten control warrants institutional action. Consider creating parameters for calling the physician if glycemic targets aren’t met as a standing order, or integrate a few limited choices for glycemic targets into your insulin order sets, which trigger calls from nursing should glucose values fall persistently outside this range. Some institutions print out all glucose values for their monitored patients on each ward on a day-to-day basis, along with their glucose control regimen. Pharmacists or nurses get involved in asking for physician action and presenting recommended choices (such as adding scheduled basal insulin). Others refer similar information to a special team (a “glucose control team” or “hyperglycemia hit squad”) who intervenes via consultation or direct ordering strategies. Certain electronic medical records may have the capability of prompting physician action when glucose values are out of the target range. The what to do is common across all institutions: push for order changes when glycemic targets aren’t met. The specifics of the glycemic target and the who and the how the spur to action occurs is institution specific.
. Others refer similar information to a special team (a glucose control team or hyperglycemia hit squad ) who intervenes via consultation or direct ordering strategies. Certain electronic medical records may have the capability of prompting physician action when glucose values are out of the target range. The what to do is common across all institutions: push for order changes when glycemic targets aren’t met. The specifics of the glycemic target and the who and the how the spur to action occurs is institution specific.")
33
Hierarchy of Reliability
Predicted Success rate Level 1 No protocol* (“State of Nature”) Decision support exists but not linked to order writing, or prompts within orders but no decision support Protocol well-integrated (into orders at point-of-care) Protocol enhanced (by other QI and high reliability strategies) Oversights identified and addressed in real time 40% 50% 2 3 65-85% 4 90% 5 95+% eliminate variation arising from professionals; retain variation arising from patients
 Decision support exists but not linked to order writing, or prompts within orders but no decision support. Protocol well-integrated (into orders at point-of-care) Protocol enhanced (by other QI and high reliability strategies) Oversights identified and addressed in real time. 40% 50% % 4. 90% % eliminate variation arising from professionals; retain variation arising from patients.")
34
Setting Academic teaching medical centers with over 400 beds
Adult inpatients on non-critical care wards with POC glucose testing. Nov 2002 – Dec 2005 Excluded: Critical care, OB, Psych, Senior Behavioral Health

35
Questions What is current state? Baseline Nov ’02-Oct ’03.
Insulin Use Patterns Glycemic Control Hypoglycemia Other What is effect of implementing a standardized SQIO set? Main Intervention #1 Nov ’03-May ‘05 What is the incremental effect of an insulin management protocol? Main Intervention #2 May ’05-Dec ‘05

36
Intervention #1 (Nov 2003): A Basic Subcutaneous Insulin Order Set
Basal / Nutritional / Correction dose terminology introduced Multiple correction dose scales available, based on total insulin dose required. Sliding scale only regimens discouraged Check box simplicity Some guidance for dosing and adjustment Hypoglycemia protocol incorporated Paper, then CPOE versions

37
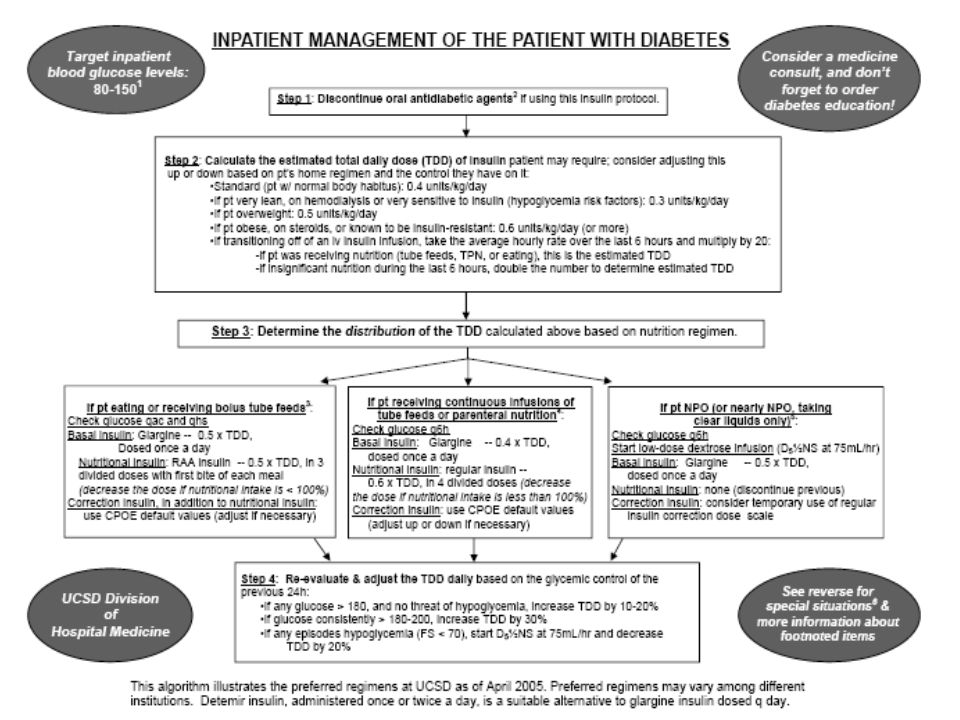
Intervention #2 (May 2005) Insulin Management Protocol
One page algorithm Glycemic Target Prompt for A1C DC Oral Hypoglycemic Agents Guidance on dosing Suggested regimens for eating patient, NPO patient, patient on enteral nutrition Guidance on dosing adjustment Introduced with case based teaching

39
The Use of Basal Insulin Increases (sliding scale only regimens decline)
UCSD clinicians have done a good job of switching to regimens that have some scheduled basal insulin in them, but we still see a lot of variability. The first generation order set was introduced 10/03, and the computerized order entry version was initiated at UCSD Thornton 1/04, then at Hillcrest in the summer of ’04. 30-90 patients sampled per month, no formal analysis done, results sustained

40
Glycemic Control Days 1 – 14 of admission
Exclude patients with < 8 POC tests 5,800 patients 37,516 patient days 111,473 POC tests By patient stay % of patients with mean glucose < 180 mg /dL By patient day % of patient days when all glucose values were between 60 – 180 mg / dL Pearson chi-square statistic to compare: TP 1 (Baseline) Nov ’02 – Oct ‘03 TP2 (Order Set) Nov ‘03 – Apr ’05 TP3 (Algorithm) May ’05 – Dec ’05
 Nov ’02 – Oct ‘03. TP2 (Order Set) Nov ‘03 – Apr ’05. TP3 (Algorithm) May ’05 – Dec ’05.")
41
73% 69% 62 % 5800 patients w/ > 8 POC glucose values, day 1-14 values: p value < .02 (Pearson chi-square statistic)
")
42
Algorithm Baseline Order set 1st order set

43
53% 48% 44% 37,516 Patient Days monitored in 5800 patients with > 8 POC glu tests, day 1-14: (Pearson chi-square statistic p < .001)
")
44
Clinical Inertia Improves with Order Set and Algorithm

45
Oh no! What about…… HYPOGLYCEMIA!

46
Hypoglycemia All non critical care patients with POC values
11,057 patients / 53,466 days / 148,466 POC tests Hypoglycemia: ≤ 60 mg/dL Extreme Hypoglycemia: ≤ 40 mg/dL By patient day % of patient days with one or more hypoglycemic events Pearson chi-square statistic to compare: TP 1 (Baseline) Nov ’02 – Oct ‘03 TP2 (Order Set) Nov ‘03 – Apr ’05 TP3 (Algorithm) May ’05 – Dec ’05
 Nov ’02 – Oct ‘03. TP2 (Order Set) Nov ‘03 – Apr ’05. TP3 (Algorithm) May ’05 – Dec ’05.")
47
Percent of Patient Days with Hypoglycemia / Extreme Hypoglycemia decreased by 30% and 31%, respectively. (Pearson chi square p < .02) > 53,000 patient days > 148,000 POC glu tests

48
Approximately 100 fewer patients with Hypoglycemia per year
Month

49
Summary Large opportunities for improvement A safety and quality issue
Systems approach is needed SHM and others now provide resources to assist implementation teams with all “essential elements” Use “Talking Points”, local anecdote, and small sample data to gain institutional support Reduced hypoglycemia can be compatible with improved glycemic control on the wards Controversy exists, but time for action is now

50
The first time subcutaneous insulin is ordered, the prescriber is asked for an actionable glycemic target. A prompt to order HbA1C is also presented.

51
The weight and markers of insulin sensitivity are elicited, as well as the form of the patient’s nutritional intake. (in this case, the patient is an obese 80 kg woman eating regular meals)
.")
52
The Total Daily Dose (TDD) is calculated for the clinician, based on the information provided on the patient’s obesity and weight. The TDD can be adjusted by the physician. Alternate methods of calculating the TDD are also presented.

Similar presentations