Download presentation
Presentation is loading. Please wait.

1
Otitis Media J. MacCormick, MD, FRCSC Associate Professor U of Ottawa
Division Otolaryngology Children’s Hospital Eastern Ontario Images used in this lecture were obtained from the presenter’s collection, various textbooks and internet websites., particulaly Abraham Jacob MD, The Ohio State University. Their use is for educational purposes only.

2
Objectives Define the middle ear cavity
Compare and contrast acute otitis media and serous otitis media with respect to natural history, etiology, prevalence, symptoms and signs List the complications of acute otitis media Describe the contemporary management of acute otitis media

3
The Eustachian Tube

4
The Eustachian Tube Connection between middle ear (ME) & nasopharynx (NP) Medial 2/3 fibro-cartilage; lateral 1/3 bony Equalizes ME pressure with atmospheric pressure Lined with respiratory epithelium Mucociliary clearance towards the NP – drains fluid from ME Usually closed to prevent reflux of NP contents into ME 13 birth; 36 mm in adulthood More horizontal at birth; elongates and descends over time

5
Eustachian Tube Embryology
ET and middle ear develop from the first pharyngeal pouch (endoderm) The external ear canal develops from the first branchial cleft (ectoderm) The ossicles develop from the 1st and 2nd branchial arches The interface between the first pharyngeal pouch and the first branchial cleft forms the tympanic membrane
 The external ear canal develops from the first branchial cleft (ectoderm) The ossicles develop from the 1st and 2nd branchial arches. The interface between the first pharyngeal pouch and the first branchial cleft forms the tympanic membrane.")
6
Eustachian Tube Dysfunction
Abnormal cranial base anatomy Bony anatomy Abnormal musculature Tensor veli palatini and/or levator veli palatini, e.g. cleft palate Inflammation/edema Physical obstruction (e.g. adenoids) Usually “too closed” but can also be “too open” (patulous Eustachian tube)
 Usually too closed but can also be too open (patulous Eustachian tube)")
7
Eustachian Tube Musculature

9
EUSTACHIAN TUBE (ET) DYSFUNCTION
Active Opening equalizes pressure in middle ear If dysfunctional, air in middle ear space is gradually absorbed Negative middle-ear pressure Retraction With enough vacuum effect, fluid is sucked from the surrounding tissue (effusion) Increasing angulation of tube improves ET function 95% children normal ET function by age 7
 Increasing angulation of tube improves ET function. 95% children normal ET function by age 7.")
10
ACUTE OTITIS MEDIA antecedent event (URI)
congestion mucosa Eustachian tube negative middle ear pressure aspiration of potential pathogens accumulation of effusion microbial pathogens proliferate suppurative & symptomatic O.M.

12
Acute Otitis Media (AOM)
")
13
Acute Otitis Media

14
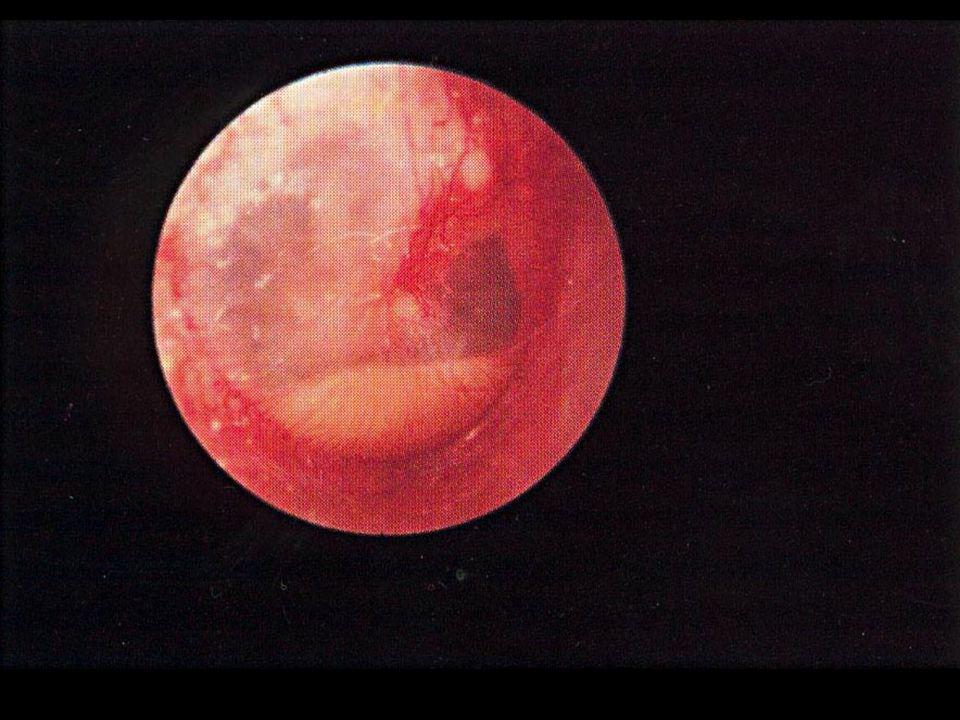
Severe AOME, pre Rupture

15
ACUTE OTITIS MEDIA Treatment Antibiotics +/- anti-inflammatories

16
CASE #1 Lisa HPI: 3 yo healthy girl
4 day hx Upper Respiratory Infection fever last pm, crying, pulling at ears mom using Tylenol

17
Rel Hx: O/E: daycare no previous AOME’s T 38oC cranky
red TM’s, slight bulge

19
Management….

20
TO TREAT OR NOT TO TREAT 80% AOM resolve without antibiotics
no diff in fever, otorrhea, or middle ear effusions at 3 mos, between treatment vs nontreatment groups only benefit: pain by day 2 is less in treated group therefore do not need to treat everyone….but who??

21
NEED TO TREAT DUE TO HIGHER FAILURE RATE:
age <2 ( risk meningitis) perforated ear temp >38.5oC
 perforated ear. temp >38.5oC.")
22
RECOMMENDATIONS if Watch & Wait
carefully choose subjects recheck 48 hrs, or if reliable parent, return if , or persistent symptoms Advil/Motrin treat if toxic, temp >38.5o F/U 4 weeks

23
Lisa’s Management?

24
Lisa’s Management Age>2, not too toxic, reliable parents, not perforated Conservative watch and wait Reassess in office 48 hrs

25
CASE #2 Tom HPI: 18 month boy
Upper Respiratory Tract Infection x2 days fever & crying last pm pulling at ears

26
O/E: 38.5oC red bulging TM’s No previous AOME’s

28
Immediate management to treat or not? with what? how long?

29
Tom’s Management Age<2 High fever Will treat

30
Etiology of AOM: Bacteria
H. influenzae M. catarrhalis 22% 14% GAS 3% S. pneumoniae No 36% growth 25%

31
Antibiotic Choice First Line antibiotics if no previous antibiotics in last 3 months Amoxicillin For Penicillin allergic patient: Clarithromycin Azithromycin (TMP/SMX- but significant resistance)
")
32
DURATION OF THERAPY 5-7 day treatment (3 days for azithromycin)
equal efficacy to 10 days fewer side effects better compliance 10 days needed for: age <2 perforation & otorrhea (drainage)
")
33
Tom’s Follow Up In 4 wks No symptoms Fluid present

36
Case #3 David 2 days after given amoxicillin for AOM
He still has fever intermittently and cries throughout the night. He continues to eat poorly and is fussy during the day His temperature is 38.7o C The otoscopy findings follow:

38
Trends in Resistance to S. pneumoniae in Canada
Amoxicillin % High Dose Amoxil <1% Cefuroxime % Cefprozil 10% Erythromycin* 10% TMP/SMX % 0% 10% 20% 30% *Cross-resistance with other macrolides e.g., azithromycin, clarithromycin Low DE et al. Antimicrob Agent Chemother 2002;46: , Kellner JD et al. 42nd ICAAC, San Diego, September 2002

39
S. PNEUMONIAE RESISTANCE
S. pneumoniae is often cause of persistent otitis is cause of majority of complications increases with antibiotic use in the 3 months prior Best oral agent is high dose amoxicillin ( mg/kg/day)
")
40
Trends in Resistance to H.influenzae in Canada
Amoxicillin % Cefuroxime 1% Cefprozil 10% Azithromycin <1% Clarithromycin 2% TMP/SMX % 0% 10% 20% 30% Zhanel G et al. JAC 2000;45:655-62, Hoban DJ et al. Clin Infect Dis 2001;32(Suppl 2):S81-93
:S")
41
David’s Management Failed Treatment of Amoxil
May be S pneumonia, H influenza Consider 2nd line antibiotic: Clavulin (amoxil + clavulinic acid, neutralizes Beta Lactamase) 2nd generation cephalosporin macrolide for penicillin allergic If quite ill, more likely S pneumonia High dose amoxicillin If very ill or not sure of bug: amoxicillin (40mg/kg/d)+ Clav/amox (40 mg/kg/d) to provide high dose amox for pen resistant pneumococcus, as well as the clavulinic acid for Beta Lactamase positive H influenza
 2nd generation cephalosporin. macrolide for penicillin allergic. If quite ill, more likely S pneumonia. High dose amoxicillin. If very ill or not sure of bug: amoxicillin (40mg/kg/d)+ Clav/amox (40 mg/kg/d) to provide high dose amox for pen resistant pneumococcus, as well as the clavulinic acid for Beta Lactamase positive H influenza.")
42
PROPHYLAXIS works 73% of time BUT OUT OF FAVOR because it causes resistance amoxicillin prophylaxis study* Showed an increase in Beta Lactamase Positive(BLP) organisms in nasopharynx from baseline 20%- 100% Showed an increase in penicillin resistant s. pneumoniae (PRSP) from 0% to 25% Use for patients too ill to go to OR for tubes, or waiting for OR * Brook 1995
 organisms in nasopharynx from baseline 20%- 100% Showed an increase in penicillin resistant s. pneumoniae (PRSP) from 0% to 25% Use for patients too ill to go to OR for tubes, or waiting for OR. * Brook")
43
Indications for Ventilation Tubes for Recurrent AOM
4 episodes AOM in 6 months, 6 in 12 months Most ENT’s require also evidence of significant quality of life interference e.g. miserable, febrile, screaming with each AOM; needing 2 courses of antibiotics to clear; developing allergies to Ab Reduced number needed if febrile seizures occurring, language delay with recurrent transient hearing loss

44
CASE #4- Ahmed 4 year old boy with speech delay
seems to understand well but does not speak clearly only 2 known ear infections, but has a lot of colds Doc notes fluid always present parents are concerned that he is not joining in at kindergarten and other children do not understand what he says kindergarten teacher suggests he is not ready to start school next year, even though he will be 5 in October

47
Otitis Media with Effusion (Chronic non-suppurative Otitis Media)
Middle ear filled with serous or mucoid fluid, no purulence Often present after acute otitis media is treated appropriately with antibiotics Most will clear within 3 months Chronic after 3 months (COME)
")
48
Etiology of OME 50% sterile to culture Eustachian tube dysfunction 48

49
Mucoid OM (Glue)
")
51
Mucoid OM

52
Serous OM

53
Serous OM

54
MIDDLE EAR EFFUSION CLEARANCE RATE AFTER AOM
2 weeks - 30% 4 weeks - 60% 8 weeks - 80% 12 weeks- 90%

55
Management COME After 3 Months
rarely consider trial antibiotics boost short-term resolution by only 15% (benefit to one in seven treated) fix modifiable factors consider nasal steroid if congested control allergies do hearing test If fluid and hearing loss persist, esp if speech/language delay consider tubes
 fix modifiable factors. consider nasal steroid if congested. control allergies. do hearing test. If fluid and hearing loss persist, esp if speech/language delay consider tubes.")
56
Modifiable Risks for COME
Going to sleep with a bottle or drinking from a bottle while lying on his/her back Smoking in the house A wood burning stove, Cat Day care with > 6 kids Pacifier

57
VENTILATION TUBES FOR COME
Insert if: Fluid present bilaterally for more than 3 months Hearing level worse than 30dB threshold hearing level Be more aggressive if language delay is present Unilateral- if present, worse than 30dB for > 6 months

58
Tympanostomy Tubes Not just there to “drain fluid”
Bypass Eustachian tube to ventilate middle ear 58

60
Complications of otitis media
Intratemporal Mastoiditis Petrositis Labyrinthitis Facial paralysis Perforation Intracranial Extradural abscess Subdural abscess Brain abscess Meninigitis Sinus thrombophlibitis Extracranial Retropharyngeal abscess Parapharyngeal abscess Lymphadentitis

61
Intra-Temporal complications

62
PERFORATIONS Can reduce hearing Risk of water entry
Risk of cholesteatoma invasion

65
Acute Mastoiditis AOM: 88% fever: 83%
History/Px AOM: 88% fever: 83% narrowed external auditory canal: 80% Sagging of posterosuperior meatal wall postauricular edema: 76% Microbiology: S. pneumoniae > P. aeruginosa > other species

66
Treatment Hospitalization for IV antibiotics +/- Myringotomy and tube
+/- I&D subperiosteal abscess if present +/- CT +/- Cortical Mastoidectomy

67
Surgery Conditions for surgical treatment:
failure to respond to antibiotics significant abscess intracranial complications coalescence (Bony trabeculae broken down)= surgery non-coalescence medical management +\- myringotomy
= surgery. non-coalescence medical management +\- myringotomy.")
68
Facial nerve paralysis
-Acute otitis media Treatment : -ventilation tube -rarely need mastoidectomy -consider steroids -most get complete recovery

69
Intracranial complications

70
Intra-cranial Complications
Meningitis the most common intracranial complication of otitis media. Tube, +/- mastoidectomy, IV Ab

71
Intra-cranial complications
Extradural abscess: Diagnosis – CT scans reveal the abscess as well as the middle ear pathology. Treatment: – Mastoidectomy and drainage of the abscess

72
Intra-cranial complications
It is most lethal complication of suppurative otitis media

73
Intra-cranial complications
Venous Sinus Thrombosis Clinical picture: – Signs of blood invasion: • (spiking) fever with rigors and chills • persistent fever (septicemia). – Signs of increased intracranial pressure: headache, vomiting, and papilledema.
 fever with rigors and chills • persistent fever (septicemia). – Signs of increased intracranial pressure: headache, vomiting, and papilledema.")
74
Otitic Hydrocephalus increased intracranial pressure without effect or signs of hydrocephalus no evidence of ventricular dilatation and focal neurologic signs are absent Headache, drowsiness, vomiting, blurring of vision, and diplopia are typical symptoms. Papilledema and sixth cranial nerve palsy are usually evident.

75
Otitis Hydrocephalus Optic atrophy can eventually develop
A normal CSF cytology and biochemistry along with an opening pressure greater than 24 mm H2O very commonly associated with sigmoid sinus thrombophlebitis not all patients with sigmoid sinus thrombophlebitis develop otitic hydrocephalus

76
Complications of Otitis Media
Due to antibiotics, the incidence of complications has greatly declined. Complications are usually associated with some degree of bone destruction, granulation tissue formation, or the presence of a cholesteatoma. Complications arise most commonly by infection spreading by direct extension from the middle ear or mastoid cavity to adjacent structures.

77
Complications of Otitis Media
Patients appear more ill than expected fever, new onset vertigo, sensorineural hearing loss, fetid drainage, facial nerve weakness, proptotic ear lethargy and mental status changes CT +/- MRI are indicated

78
Cholesteatoma

79
Cholesteatoma Cholesteatomas are epidermal inclusion cysts of the middle ear and/or mastoid with a squamous epithelial lining Contain keratin and desquamated epithelium Misnomer because the cysts don’t contain cholesterol Natural history is progressive growth with erosion of surrounding bone due to pressure effects and osteoclast activation

80
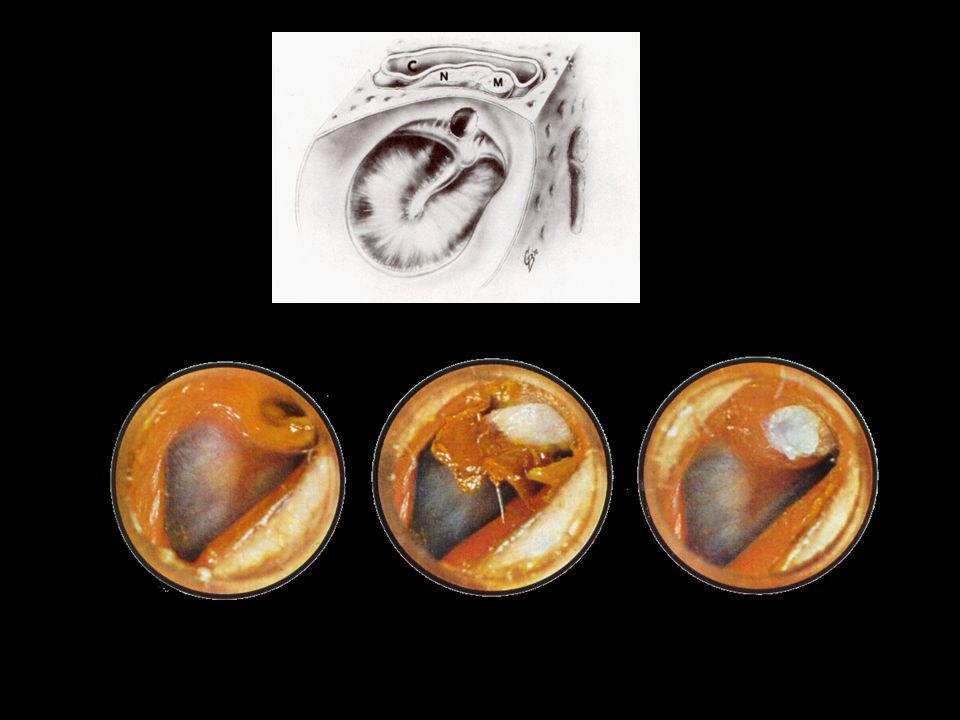
Acquired Cholesteatoma From Perforation
As the edges of the Tympanic Membrane try to heal, the squamous epithelium migrates into the middle ear

81
Eustachian Tube Dysfunction: Progression of Cholesteatoma
Pars Flacida

83
Mastoidectomy 30% recurrence/persistence in pediatrics

84
Conclusion Not all cases of acute otitis media need to be treated with antibiotics Amoxicillin/TMP-SMX remains first line for non recurrent AOM Recurrent AOM within 3 months, or recent antibiotic use, choose second line antibiotics High dose amoxicillin for resistant cases

85
Refer to ENT and Audiology if fluid is present for 3 months
In meantime, assess environmental issues, nasal congestion, immunization If you see something white coming through the tympanic mambrane, or behind it, refer to ENT in case it is a cholesteatoma

86
Questions?

Similar presentations












>")













. >")
 is inflammation.>")



