Download presentation
Presentation is loading. Please wait.

2
Pulmonary Function Tests

3
Spirometer A device that measures the volume of gas entering or leaving the mouth A spirometer measures changes in lung volume A spirometer measures subdivisions of vital capacity A spirometer does NOT measure RV

4
ERV/IRV Expiratory/Inspiratory reserve volume
Vt Tidal volume VC Vital Capacity ERV/IRV Expiratory/Inspiratory reserve volume These are all measured easily with spirometers FRC Functional residual capacity RV residual volume TLC Total lung capacity (RV + VC) Measuring these requires more specialized equipment
 Measuring these requires more specialized equipment.")
5
RESPIRATORY MANOEUVRE
Maximal breath in Maximal breath out

6
Tidal Volume Vt Total Lung Capacity

7
Vital Capacity VC Vt TLC

8
Residual Volume VC Vt TLC Residual Volume RV

9
Functional Residual Capacity
IC Vt TLC FRC RV

10
TLC=VC + RV VC Vt TLC Residual Volume RV

11
Subdivisions of Lung Volume
IRV IC VC Vt TLC TLC ERV FRC RV

12
LUNG VOLUMES Dead space ? Residual Tidal volume Volume ? Total lung
capacity Expiratory reserve volume Tidal volume Vital capacity Inspiratory reserve volume

13
Capacities Total Lung Capacity Vital Capacity
TLC = IC + FRC TLC = RV + ERV + VT + IRV Vital Capacity VC = ERV + VT + IRV VC= ERV + IC Functional Residual Capacity FRC = RV + IRV

14
FEV1 & FVC Forced expiratory volume in 1 second Forced vital capacity
young trained athletes: 4.0 L Forced vital capacity young trained athletes: 5.0 L FEV1/FVC = 80% FEV1 FVC

15
By calculation: RV = TLC - VC FRC = TLC - IC by spirometry
by body plethysmography or helium dilution TLC FRC = TLC - IC By calculation: RV = TLC - VC

16
TLC RV ERV IC TLC VC Vt VC FRC RV RV Normal

17
Vital capacity is reduced in both obstructive and restrictive diseases
VC VC VC RV RV RV Obstructive Normal Restrictive

18
Restrictive lung disease
By definition means a reduced total lung capacity Reduced vital capacity can suggest restriction TLC V t VC FRC RV

19
Why measure residual volume
Why measure residual volume? Look at two people with identical vital capacity TLC TLC Vt Vt VC FRC VC RV FRC RV

20
RV RV TLC TLC Vt Vt VC FRC VC FRC
Be careful before citing “restrictive deficits” in people with obstructive lung disease TLC TLC Vt Vt VC FRC VC RV FRC RV Emphysema Normal

21
FLOW-VOLUME CURVE in respiratory patients Obstructive disease
FEV1 + FVC cst FEV1/FVC Obstructive disease resistance to airflow e.g., COPD, asthma FVC + FEV1 FEV1/FVC= cst Restrictive disease expansion of the lung e.g., interstitial fibrosis FVC + FEV1 FEV1/FVC

22
Indication for lung volume test :
Low FVC : -? Restrictive -? Obstructive with hyperinflation and air trapping -? Mixed pattern -? Equivocal spirometry findings (FEV1&FVC at lower limit of normal)
")
23
Plethysmography (body box)
Measuring TLC To measure TLC or FRC, which include RV, spirometry is insufficient Techniques: Gas dilution Plethysmography (body box)
")
24
Gas dilution tests: Lung volume can be measured when a person breathes nitrogen or helium gas through a tube for a specified period of time. The final dilution of the gas used to calculate the volume of air in the thorax. It is sensitive to errors Leakage of gas Failure to measure the volume of gas in lung bullae.because helium may not mix with all parts of the lung . Helium doesn’t readily diffuse across the alveolar capillary membrane .

25
C1=N/Vbox C2=N/(Vbox+FRC)
")
26
Gas Dilution C1V1 = C2V2 C1V1 C2 V2=V1 + FRC

27
Lung Volumes / Gas Distribution
Body Plethysmography (BP) Measurement of FRC by body plethysmograph is based on an application of Boyle’s law P1V1 = P2V2 or V1 = P2V2 P1
 Measurement of FRC by body plethysmograph is based on an application of Boyle’s law. P1V1 = P2V2. or. V1 = P2V2. P1.")
28
Boyle’s Law: for fixed mass of gas at constant temperature: P1V1 = P2V2
Brief occlusion at airway opening to seal a fixed mass of gas in the lungs (V1) - i.e the FRC to be measured Pressure within lungs at end expiration (P1) ~ atmospheric pressure. P2 and V2 represent the pressure and volume in the lungs after a respiratory effort against the occlusion.
 - i.e the FRC to be measured. Pressure within lungs at end expiration (P1) ~ atmospheric pressure. P2 and V2 represent the pressure and volume in the lungs after a respiratory effort against the occlusion.")
29
Plethysmography (Body Box)
Boyle’s Law : P1V1= k Closed container whose volume can be adjusted so that the pressure in the container increases in proportion to the fractional decrease in container volume.

30
Plethysmograph No flow at the mouth so that DPm = Dpalv Pbox
Vbox is the volume of the box (known) Vth is the volume of the thorax (unknown) Vbox Pm Vth Pbox
 Vth is the volume of the thorax (unknown) Vbox. Pm. Vth. Pbox.")
31
Plungx Vlung=P’lungx V’lung
Plethysmography- measures total thoracic gas volume, but is more cumbersome. Uses Boyle’s law to calculate RV. Pbox x Vbox= P’box x V’box V’box =Vbox+∆V P’box =Pbox+∆P Plung Vlung Plungx Vlung=P’lungx V’lung V’lung = Vlung +∆V P’lung =Plung+∆P Pbox x Vbox

33
Plethysmography: Situation at end expiration, prior to any respiratory efforts against an occlusion valve

34
During inspiratory efforts against the occlusion
As lung volume increases, box volume decreases and box pressure increases As lung volume increases,alveolar pressure decreases and hence pressure at mouth decreases Changes in box pressure calibrated in terms of volume using a calibrated syringe P1 -ΔP

35
Lung Volumes / Gas Distribution
Body Plethysmography (BP) Unlike gas dilution tests, BP includes both air in communication with open airways as well as air trapped within noncommunicating thoracic compartments In patients with air trapping, plethysmography lung volumes are usually larger those measured with gas dilution methods Volume measured is referred to as thoracic gas volume (TGV or VTG) ATS is recommending term be dropped and changed to “plethysmographic lung volume” (VL, pleth), and “FRC by body plethysmography” or TGV at FRC (FRCpleth)
 Unlike gas dilution tests, BP includes both air in communication with open airways as well as air trapped within noncommunicating thoracic compartments. In patients with air trapping, plethysmography lung volumes are usually larger those measured with gas dilution methods. Volume measured is referred to as thoracic gas volume (TGV or VTG) ATS is recommending term be dropped and changed to plethysmographic lung volume (VL, pleth), and FRC by body plethysmography or TGV at FRC (FRCpleth)")
36
Body plethysmography The patient sits inside a fully enclosed rigid box and breath through mouthpiece connected through a shutter to the internal volume of the box The subject makes respiratory efforts against the closed shutter (like panting), causing their chest volume to expand and decompressing the air in their lungs. while breathing in and out again into a mouthpiece. The volume of all gas within the thorax can be measured by Changes in pressure inside the box and allow determination of the lung volume. transparent box that resembles a telephone booth
, causing their chest volume to expand and decompressing the air in their lungs. while breathing in and out again into a mouthpiece. The volume of all gas within the thorax can be measured by Changes in pressure inside the box and allow determination of the lung volume. transparent box that resembles a telephone booth.")
37
Lung Volumes / Gas Distribution
Body Plethysmography (BP) Procedure Patient is required to support cheeks with both hands and pant with an open glottis at a rate of Hz (30 – 60 breaths/min) BP shutter is suddenly closed at end-expiration prior to inspiration Panting is continued for several breaths against closed shutter (no air flow)
 Procedure. Patient is required to support cheeks with both hands and pant with an open glottis at a rate of Hz (30 – 60 breaths/min) BP shutter is suddenly closed at end-expiration prior to inspiration. Panting is continued for several breaths against closed shutter (no air flow)")
38
Lung Volumes / Gas Distribution
Body Plethysmography (BP) Procedure The thoracic-pulmonary volume changes during panting , produce air volume changes within the BP cabinet Decreases in cabinet volume are an equal inverse response to thoracic volume increase (As thoracic volumes increase with panting inspiration, BP cabinet volume decreases and visa versa)
 Procedure. The thoracic-pulmonary volume changes during panting , produce air volume changes within the BP cabinet. Decreases in cabinet volume are an equal inverse response to thoracic volume increase (As thoracic volumes increase with panting inspiration, BP cabinet volume decreases and visa versa)")
39
Lung Volumes / Gas Distribution
Body Plethysmography (BP) Criteria of Acceptability Panting maneuver shows a closed loop without drift Tracing does not go off the screen Panting is 0.5 – 1 Hz Tangents should be within 10% At least 3 FRCpleth values should agree within 5% and the mean reported
 Criteria of Acceptability. Panting maneuver shows a closed loop without drift. Tracing does not go off the screen. Panting is 0.5 – 1 Hz. Tangents should be within 10% At least 3 FRCpleth values should agree within 5% and the mean reported.")
41
The history of clinical whole body plethysmography
1790 Menzies „Dissertation on Respiration“ 1881/2 Gad und Pflüger, „Residualvolumen“ Verzar, Du Bois, Mead etc 1972, Matthys „Historische Entwicklung der klinischen Ganzkörperplethysmographie“ Atemw.u.Lungenkrkh. 31/4,

44
Lung Volumes / Gas Distribution
Body Plethysmograph Two types Constant-volume, variable-pressure “Pressure Plethysmograph” Flow or variable-volume “Flow Plethysmograph” Both measure thoracic gas volumes and airway resistance and it derivatives Both use a pneumotachometer to measure flow and a mouth transducer with a shutter to measure alveolar pressure

45
Lung Volumes / Gas Distribution
Body Box Calibration Mouth pressure is verified with a mercury or water barometer Flows are verified with a rotometer (flow-metering device) or a 3-liter syringe Box pressure is calibrated by using a sine-wave rotary pump simulates inspiratory/expiratory volumes
 or a 3-liter syringe. Box pressure is calibrated by using a sine-wave rotary pump. simulates inspiratory/expiratory volumes.")
46
INTERPRETATION of RESULTS
In patients with obstructive diseases airway closure occurs at an abnormally high lung volume FRC (functional residual capacity) RV (residual volume) Patients with reduced lung compliance (e.g., diffuse interstitial fibrosis) stiffness of the lungs + recoil of the lungs to a smaller resting volume FRC RV
 RV (residual volume) Patients with reduced lung compliance (e.g., diffuse interstitial fibrosis) stiffness of the lungs + recoil of the lungs to a smaller resting volume. FRC. RV.")
47
Clinical Applications and Interpretations
FRC gas trapping due to intrathoracic airway obstruction cystic lung disease FRC abnormal alveolar development reduced recoil of chest- wall decreased lung compliance atelectasis

48
What do the results mean: Algorhithim for PFT's Assessing severity of restrictive defects
Without TLC measurement, base severity on the FVC ≥80% is considered “normal” 70-80% is considered mild 60-70%% is considered moderate 60% is considered severe When TLC is measured Gold standard to define restrictive ventilatory defect Only order “Full PFTs” if you suspect restrictive or interstitial lung disease (expensive!)
")
49
What do the results mean: Algorhithim for PFT's
Is the FEM adequate? y e s n o Is the FEV1/FVC lower than predicted? Interpretation may be limited by falsely low FVC y e s n o This is the definition of obstruction Mild FEV1 >70% Moderate FEV % Mod severe FEV % Severe FEV1 <50% Very severe FEV1 <40% Is FVC reduced? y e s n o Restriction may be present; Need TLC to definitively diagnose restriction Normal pulmonary mechanics Restriction Spirometry: Lung volumes: Severity is determined Severity determined by by the reduction in VC the reduction in TLC Mild 70-80% Mild 65-80% Moderate 60-70% Moderate 50-65% Severe <60% Severe <50%

50
What can PFTs tell you about the patient
Normal or abnormal What diseases can you diagnose? Only asthma is defined by its PFTs Estimation of impairment, or severity of disease Response to therapy Occupational surveillance

51
What PFTs cannot tell you
Does the degree of abnormality explain the patients symptoms? “Normality” does not exclude the presence of disease Abnormal test may not reflect loss of lung function

52
By this technique we will be able to know
Residual volume (RV) Tidal volume (TV) Total Lung Capacity (TLC) Expiratory reserve volume (ERV) Inspiratory Reserve Volume (IRV) Inspiratory capacity (IC) Functional residual capacity (FRC) Vital Capacity (VC)
 Tidal volume (TV) Total Lung Capacity (TLC) Expiratory reserve volume (ERV) Inspiratory Reserve Volume (IRV) Inspiratory capacity (IC) Functional residual capacity (FRC) Vital Capacity (VC)")
53
Residual volume (RV) It is the volume of air remaining in the lungs at the end of maximal expiration. Normally it accounts for about 25% of TLC. - RV increased in airway narrowing with air trapping (Asthma) or in loss of elastic recoil (emphysema). - RV decreased in Increased elastic recoil (pulmonary fibrosis)
 or in loss of elastic recoil (emphysema). - RV decreased in Increased elastic recoil (pulmonary fibrosis).")
54
Tidal volume (TV) It is the volume of air inspired or expired with each breath during normal breathing ( 7ml/kg) ml TV decreased in severe RLD
 It is the volume of air inspired or expired with each breath during normal breathing ( 7ml/kg) ml TV decreased in severe RLD")
55
Total Lung Capacity (TLC) It is the total volume of air within the lung after maximum inspiration. (the maximum volume of air that the lung can contain). TLC = FVC + RV OR TLC = RV + ERV + TV + IRV TLC Increased in airway narrowing with air trapping (Asthma) or in loss of elastic recoil (emphysema). TLC Decreased in RLD , increased recoil (Pulmonary fibrosis), muscle weakness, Obesity…
. TLC = FVC + RV OR TLC = RV + ERV + TV + IRV TLC Increased in airway narrowing with air trapping (Asthma) or in loss of elastic recoil (emphysema). TLC Decreased in RLD , increased recoil (Pulmonary fibrosis), muscle weakness, Obesity….")
57
Expiratory reserve volume (ERV): It is the maximal volume of air exhaled from the resting end-expiratory level. ( volume expired by active expiration after passive expiration. ERV: From TV to RV ERV decreased in RLD

58
Inspiratory Reserve Volume (IRV): It is the maximal volume of air inspired with effort in excess of tidal volume IRV: From TV to TLC
: It is the maximal volume of air inspired with effort in excess of tidal volume IRV: From TV to TLC")
59
Inspiratory capacity (IC): It is the maximal volume of air inspired from resting expiratory level IC= IRV+TV.
: It is the maximal volume of air inspired from resting expiratory level IC= IRV+TV.")
60
Functional Residual Capacity (FRC) It is the volume of air remaining in the lungs at the end of resting (normal) expiration. FRC = RV + ERV. -FRC Increased (>120% of predicted) in Emphysema (decreased elastic recoil), Asthma, bronchiolar obstruction (air trapping) -FRC decreased in intrinsic ILD or by upward movement of diaphragm (obesity,painful thoracic or abdominal wound)
 in Emphysema (decreased elastic recoil), Asthma, bronchiolar obstruction (air trapping) -FRC decreased in intrinsic ILD or by upward movement of diaphragm (obesity,painful thoracic or abdominal wound).")
61
Vital Capacity: volume of gas measured on complete expiration after complete inspiration without effort VC= TLC – RV or VC= IRV+TV+ERV decreased in OLD and RLD ( VC < 15 ml/kg (and VT < 5ml/kg) indicates likely need for mechanical ventilation
 indicates likely need for mechanical ventilation")
62
Lung volumes & capacities

63
Obstructive Lung Disease
Lung Volume in Obstructive Lung Disease

64
Obstructive Lung Disease
Narrowing and closure of airways during expiration tends to lead to gas trapping within the lungs and hyperinflation of the chest. Air trapping → increase in RV Hyperinflation → increases TLC RV tends to have a greater percentage increase than TLC RV/TLC ratio is therefore increased (nl 20-35%) Gas trapping may occur without hyperinflation (increase in RV & normal TLC)
 Gas trapping may occur without hyperinflation (increase in RV & normal TLC)")
65
Gas trapping and airway closure at low lung volume cause the patient to breath at high lung volume so FRC (RV+ERV) increased This will prevent airway closure and improve ventilation-perfusion relationship It will reduce mechanical advantage of respiratory muscles and increases the work of breathing

66
Obstructive Lung Disease cont.
RV increased TLC Nl/increased RV/TLC increases FRC increased VC decreased *Air trapping :Normal TLC with increase RV/TLC *Hyperinflation: Increase in both TLC and RV/TLCl/

67
Restrictive Lung Disease
Lung Volume in Restrictive Lung Disease

68
Reduction in TLC is a cardinal feature
1. In Intrinsic RLD (Interstitial Lung Disease) TLC will decrease RV will decrease because of increased elastic recoil (stiffness) of the lung and loss of the alveoli. Breathing take place at low FRC because of the increased effort needed to expand the lung . RV/TLC normal
 TLC will decrease. RV will decrease because of increased elastic recoil (stiffness) of the lung and loss of the alveoli. Breathing take place at low FRC because of the increased effort needed to expand the lung . RV/TLC normal.")
69
2. In extrinsic RLD (chest wall disease :kyphoscoliosis or neuromuscular disease:ALS,MG)
TLC is reduced either because of mechanical limitation to chest wall expantion or because of respiratory muscle weakness RV is Normal because Lung tissue and elastic recoil is normal So RV/TLC ratio will be high Breathing take place at low FRC because of the increased effort needed to expand the lung .

70
Restrictive Lung Disease:
RLD Intrinsic & severe chest wall dis (pleural and skeletal) TLC decreased RV decreased RV/TLC normal FRC decreased VC decreased Extrinsic RLD TLC decreased RV normal RV/TLC High
 TLC decreased. RV decreased. RV/TLC normal. FRC decreased. VC decreased. Extrinsic RLD. TLC decreased. RV normal. RV/TLC High.")
71
3. In combined obstructive and restrictive disease (e,g
3. In combined obstructive and restrictive disease (e,g.sarcoidosis ,COPD+IPF) Obstructive pattern on spirometry and Reduced lung volume 4. In equivocal spirometry result : e,g.when FEV1,FVC at lower limit of normal If TLC or RV raised the diagnosis is obstructive lung disease
 Obstructive pattern on spirometry and. Reduced lung volume. 4. In equivocal spirometry result : e,g.when FEV1,FVC at lower limit of normal. If TLC or RV raised the diagnosis is obstructive. lung disease.")
72
FEV1 FVC FEV1/FVC RV TLC RV/TLC VC FRC RLD Extrinsic RLD Interinsic
Obstructive Lung dis. FEV1 FVC FEV1/FVC RV TLC RV/TLC VC FRC

73
Interpretation: no significant differences of the measured data from the normal reference values

74
Interpretation: Cough with light obstructive ventilatory defect and relative overinflation

75
Interpretation: severe effort dependant intrathoracic airway obstruction with overinflation and trapped air

76
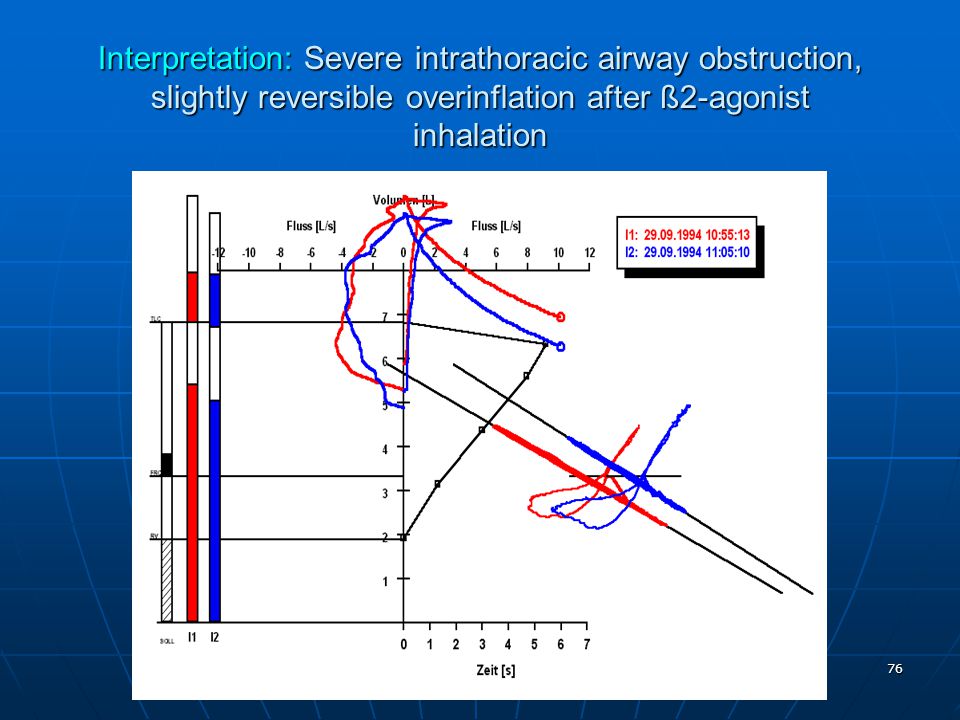
Interpretation: Severe intrathoracic airway obstruction, slightly reversible overinflation after ß2-agonist inhalation 20 5
77
Interpretation: Mixed restrictive and obstrucive ventilatory defect with relative overinflation

78
Interpretation: Carbacholtest positive, overinflation with good reversibility after ß2-agonist inhalation

79
The infant plethysmograph

80
Infant plethysmography

81
Plethysmography: Closed system: changes in thoracic volume
are inversely proportional to changes in ‘box’ volume.

Similar presentations










>")









 Role of surfactant Lung volumes and capacities Anatomical and physiological VD Alveolar space and.>")


 volume moved during either an inspiratory or expiratory phase of each breath (L)>")


