Download presentation
Presentation is loading. Please wait.

1
Continuous renal replacement therapy
Dr. M.A. Al-Odat Jordanian Board of Medicine Saudi ICU board fellow.

2
Continuous Renal Replacement Therapy CRRT
WHAT Is CRRT WHAT Is CRRT HOW To use CRRT

3
Continuous Renal Replacement Therapy (CRRT)
Is an extracorporeal blood purification therapy intended to substitute for impaired renal function over an extended period of time and applied for or aimed at being applied for 24 hours a day. * Bellomo R., Ronco C., Mehta R, Nomenclature for Continuous Renal Replacement Therapies, AJKD, Vol 28, No. 5, Suppl 3, November 1996 CRRT is the blanket term which encompasses all continuous therapies. It has been defined as…. Read the slide. Make sure to note the proof source.

4
CRRT Goals Mimic the functions and physiology of the native organ
Qualitative and quantitative blood purification Restore and maintain of homeostasis Avoid complications and good clinical tolerance Provide conditions favoring recovery of renal function Before I describe each unique therapy, it’s important to understand the goals of CRRT. The main goals are to: Mimic the functions and physiology of the native kidney Restore and maintain hemodynamic stability Avoid complications while achieving good clinical tolerance Provide conditions that favor renal recovery

5
Requirements for CRRT A central double-lumen veno-venous hemodialysis catheter An extracorporeal circuit and a hemofilter A blood pump and a effluent pump. With specific CRRT therapies dialysate and/or replacement pumps are required. In order, to initiate CRRT there are some essential items you will need. CRRT requires a functioning vascular access, which is usually a central double-lumen catheter, and extracorporeal circuit, a hemofilter, a blood pump, and a effluent pump. In some CRRT therapies dialysate and/or replacement pumps are required.

6
Indications CRRT is indicated in any patient who meets criteria for hemodialysis therapy but cannot tolerate intermittent dialysis due to hemodynamic instability. CRRT is better tolerated by hemodynamically unstable patients because fluid volume, electrolytes and pH are adjusted slowly and steadily over a 24 hour period rather than a 3 – 4 hour period.

7
Hemodynamically unstable patients with the following diagnoses may be candidates for CRRT:
fluid overload acute renal failure chronic renal failure life-threatening electrolyte imbalance major burns with compromised renal function drug overdose

8
Principals of CRRT Vascular access. Semi-permeable membrane.
Transport mechanism. Dialysate and replacement fluid.

9
I- Vascular access Internal jugular. Subclavian. Femoral.

10
Access Location Internal Jugular Vein Femoral Vein Subclavin Vein
Primary site of choice due to lower associated risk of complication and simplicity of catheter insertion. Femoral Vein Patient immobilized, the femoral vein is optimal and constitutes the easiest site for insertion. Subclavin Vein The least preferred site given its higher risk of pneumo/hemothorax and its association with central venous stenosis. There are three access locations that are used some may be preferred over others. Internal jugular vein is the primary choice due to the simplicity of catheter insertion. Femoral vein is a great access when a patient is immobilized, and is also considered an easy site for insertion. Subclavin is the least preferred and often used if no other sites are available. A Subclavin has a high risk of pnemo/hemothorax and is associated with central stenosis.

11
Choosing the right catheter
The length of the catheter chosen will depend upon the site used Size of the catheter is important in the pediatric population. The following are suggested guidelines for the different sites: RIJ= 15 cm French LIJ= 20 cm French Femoral= 25 cm French Choosing the right catheter is another important aspect to be considered.. The catheter length will depend on the site used. Pediatric of course will need to be assessed for an appropriate size catheter.

12
II- Semi-permeable membrane
The basis of all blood purification therapies. Water and some solutes pass through the membrane, while cellular components and other solutes remain behind. 2 types: cellulose and synthetic. Synthetic membranes allow clearance of larger molecules and are the primary type used in CRRT. Filters are changed when they become contaminated, clogged or clotted.

13
Molecular size: Both molecule size and pore size determine the solute flow through the semi-permeable membrane. As you can see from this picture we have a membrane with small pores. The pink molecule represent Urea molecules, which are considered small size molecules. The green molecules represents cytokine molecules, which are considered a middle size molecules. The (pink molecule) Urea easily passes through the small pores, but the (green molecule) Cytokines are to large to move across the membrane therefore they remain in the blood.
 Urea easily passes through the small pores, but the (green molecule) Cytokines are to large to move across the membrane therefore they remain in the blood..")
14
This picture depicts a membrane that has large pore size
This picture depicts a membrane that has large pore size. As you can see from this picture we have a membrane with large pores. Again, we will say the pink molecule represent Urea molecules, and the green molecules represent a cytokine molecules. The Urea easily passes through the large pores, and the Cytokines also move across the membrane therefore they are removed from the blood.

15
Molecular Weights (Dalton) 100000 50000 10000 5000 1000 500 100 50 10
Albumin (55000 – 60000) Beta 2 Microglobulin (11800) Inulin (5200) Vit B12 (1355) Aluminium/Desforoxamine complex (700) Glucose (180) Uric Acid (168) Creatinine (113) Phosphate (80) Urea (60) Potassium (35) Phosphorus (31) Sodium (23)
 Beta 2 Microglobulin (11800) Inulin (5200) Vit B12 (1355) Aluminium/Desforoxamine complex (700) Glucose (180) Uric Acid (168) Creatinine (113) Phosphate (80) Urea (60) Potassium (35) Phosphorus (31) Sodium (23)")
16
III- Transport mechanisms a) Ultrafiltration
The passage of water through a membrane under a pressure gradient. Driving pressure can be +ve (push fluid through the filter), or –ve (pull fluid to other side of filter). Pressure gradient is created by effluent pump.
, or –ve (pull fluid to other side of filter). Pressure gradient is created by effluent pump.")
17
Here is a visual example of how ultrafiltration works
Here is a visual example of how ultrafiltration works. On the blood side of the hemofilter you have a positive pressure gradient. on the fluid side of the hemofilter you have a negative pressure gradient. The effluent pump applies pressure on the membrane causing the fluid to move from the positive pressure gradient to the lower pressure gradient.

18
b) Convection Movement of solutes through a membrane by the force of water “solvent drag”. The water pulls the molecules along with it as it flows through the membrane. can remove middle and large molecules, as well as large fluid volumes. maximized by using replacement fluids.

19
To better understand this phenomenon, think of a quiet stream as compared to a raging river. The stream could never shift a boulder, but the powerful raging river could easily drag a boulder downstream. So it is with convection; the faster the flow through the membrane, the larger the molecules that can be transported

20
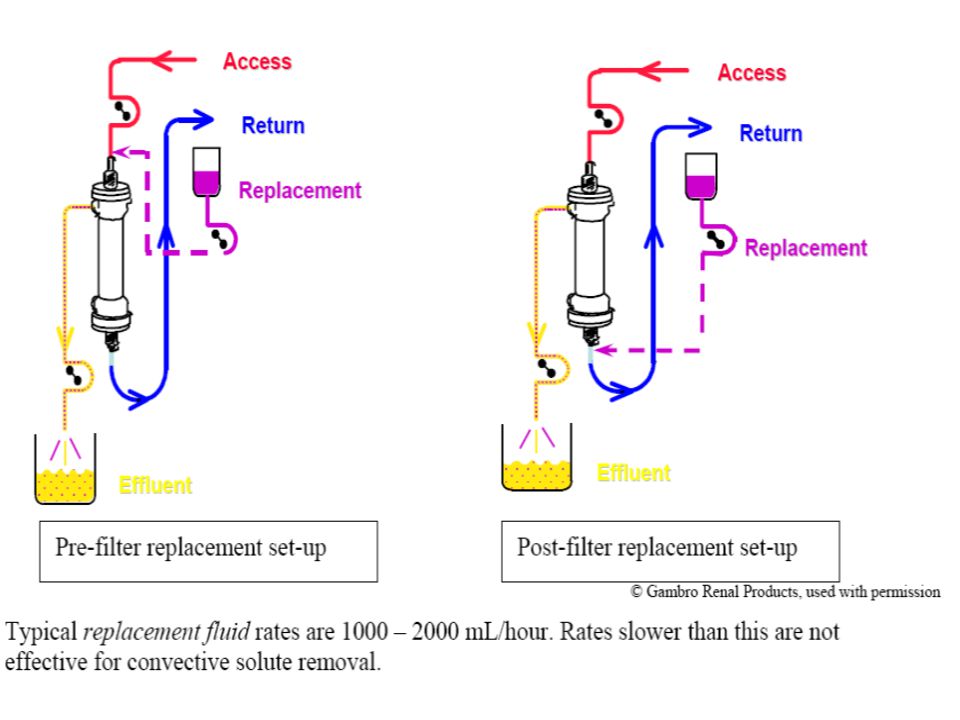
This visual will provide you with a better understanding of how convection works. From the picture you can see a faucet which represents replacement solution. The top faucet is an example of pre-filter dilution, which means that the replacement solution mixes with the blood as it enters the filter. The bottom faucet is an example of post-filter dilution and is delivered as the blood is returning to the patient. Now the effluent pump is removing ultrafiltration (just like SCUF), or patient plasma water and replacement solution.
, or patient plasma water and replacement solution.")
21
c) Adsorption Adsorption is the removal of solutes from the blood because they cling to the membrane. Think of an air filter. As the air passes through it, impurities cling to the filter itself. Eventually the impurities will clog the filter and it will need to be changed. The same is true in blood purification. High levels of adsorption can cause filters to clog and become ineffective

22
This picture gives you a great visual picture of how adsorption occurs during CRRT. some molecules will attach to the membrane surface. While other molecules may permeate the membrane, but become stuck within the fibers. It is believed that inflammatory mediators are effectively removed via adsorption.

23
d) Diffusion Diffusion is the movement of a solute across a membrane via a concentration gradient. For diffusion to occur, another fluid must flow on the opposite side of the membrane. In blood purification this fluid is called dialysate. When solutes diffuse across a membrane they always shift from an area of higher concentration to an area of lower concentration until the solute concentration on both sides of the membrane is equal.

24
The patients blood contains a high concentration of unwanted solutes that can be effectively removed by diffusion. Diffusions key mechanism is to move a solute from a higher concentration gradient to a lower concentration gradient. For example, let us assume the blood in the filter has a high concentration of potassium molecules and on the fluid/dialysate compartment has a low concentration of potassium. The potassium gradually diffuses through the membrane from the area of a higher potassium concentration to the area of a lower potassium concentration until it is evenly distributed.

25
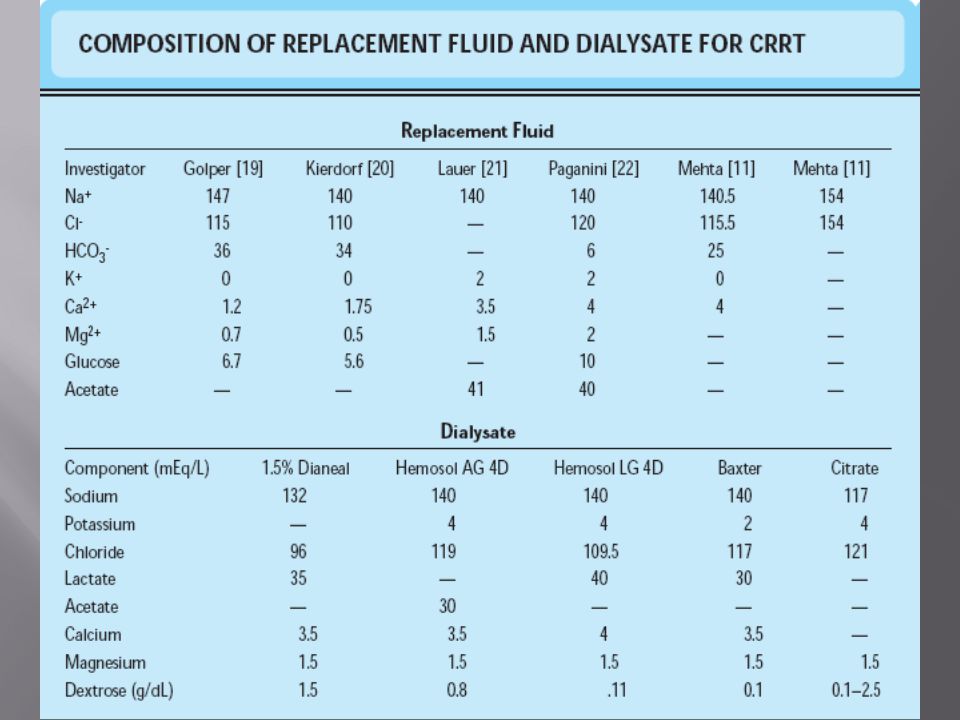
IV- Dialysate and replacement fluid
Dialysate is any fluid used on the opposite side of the filter from the blood during blood purification. As with traditional hemodialysis therapy, the dialysate is run on the opposite side of the filter, countercurrent to the flow of the patient’s blood. The countercurrent flow allows a greater diffusion gradient across the entire membrane, increasing the effectiveness of solute removal. Typical dialysate flow rates are between 600 – 1800 mL/hour.

26
Replacement fluid Used to increase the amount of convective solute removal in CRRT. Replacement fluids do not replace anything. Fluid removal rates are calculated independently of replacement fluid rates. The most common replacement fluid is 0.9% Normal Saline. Can be pre or post filter.

27
The decision to infuse replacement fluids before or after the filter is made by the physician. Replacement fluids administered pre-filter reduce filter clotting and can be administered at faster rates (driving higher convection) than fluids administered post-filter. The downside of pre-filter replacement fluids is that they invalidate post-filter lab draws; the lab results will show the composition of the replacement fluid rather than that of the effluent.

30
Modalities of CRRT

31
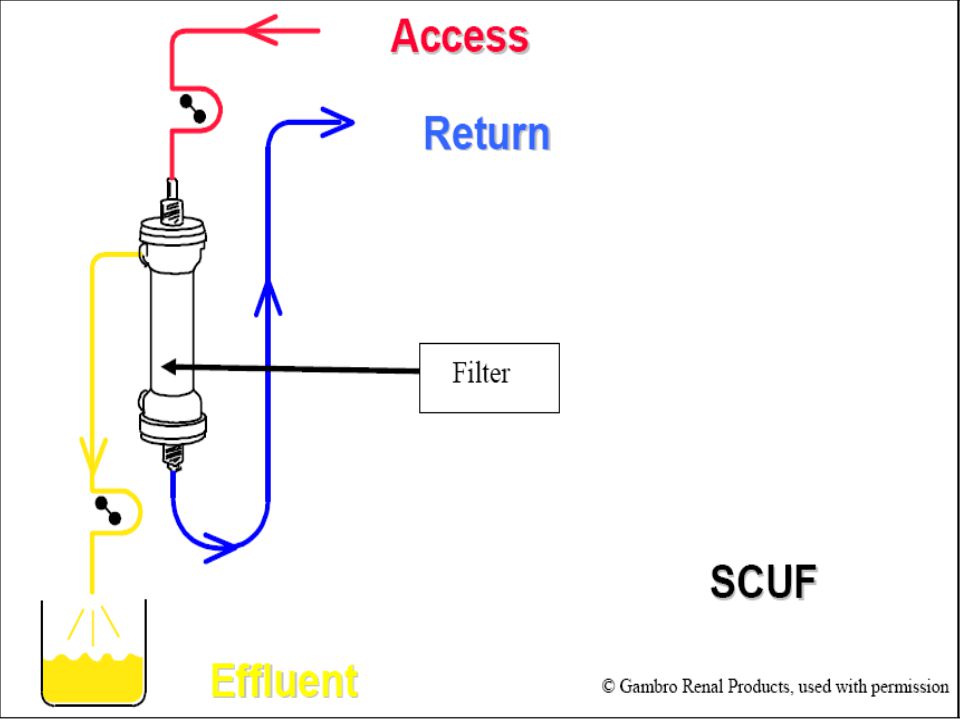
Slow Continuous Ultrafiltration (SCUF)
The primary indication for SCUF is fluid overload without uremia or significant electrolyte imbalance. The main mechanism of water transport is ultrafiltration. Other solutes are carried off in small amounts, but usually not enough to be clinically significant. the amount of fluid in the effluent bag is the same as the amount removed from the patient. Fluid removal rates are typically closer to 100 mL/hour. No dialysate or replacement fluid is used.

33
SCUF Blood flow: 80 – 200 ml/min Duration
Ultrafiltration: ml/hr (or total volume) Anticoagulation NO dialysate, NO replacement fluid
 Anticoagulation. NO dialysate, NO replacement fluid.")
34
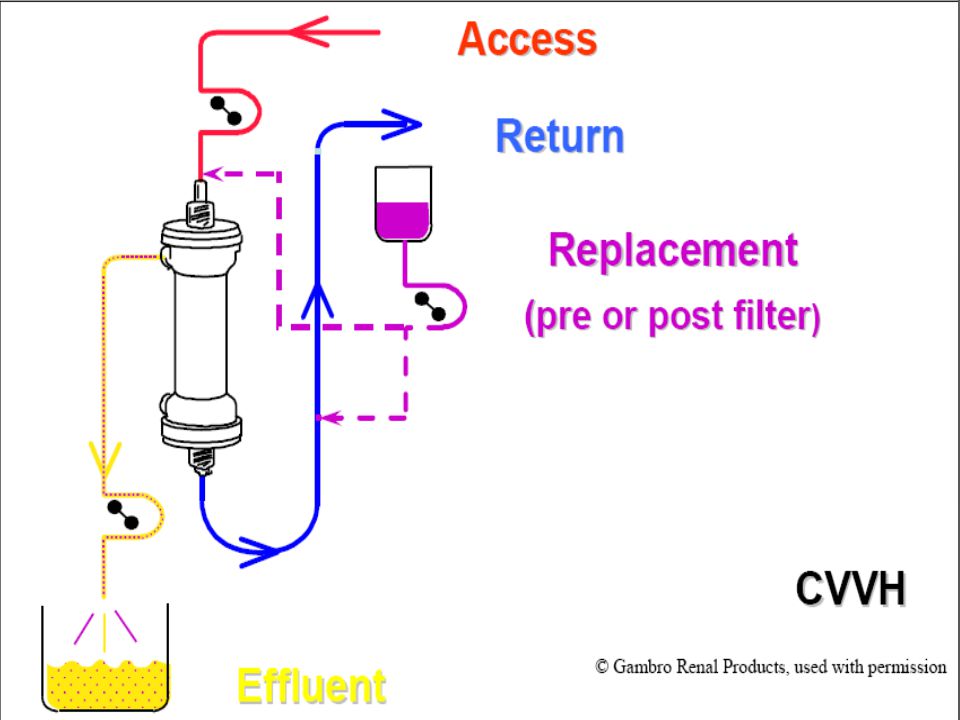
Continuous Veno-venous Hemofiltration (CVVH)
An extremely effective method of solute removal and is indicated for uremia or severe pH or electrolyte imbalance with or without fluid overload. Particularly good at removal of large molecules, because CVVH removes solutes via convection, Many theories exist regarding the removal of pro-inflammatory mediators by CVVH. solutes can be removed in large quantities while easily maintaining a net zero or even a positive fluid balance in the patient. the amount of fluid in the effluent bag is equal to the amount of fluid removed from the patient plus the volume of replacement fluids administered. No dialysate is used.

36
CVVH Blood flow:80 – 200 ml/min Duration
Ultrafiltration: ml/hr (or total volume) RF: 1000 – 2000 ml/hr , pre or post filter (up to 3 lit/hr). Anticoagulation NO dialysate
 RF: 1000 – 2000 ml/hr , pre or post filter (up to 3 lit/hr). Anticoagulation. NO dialysate.")
37
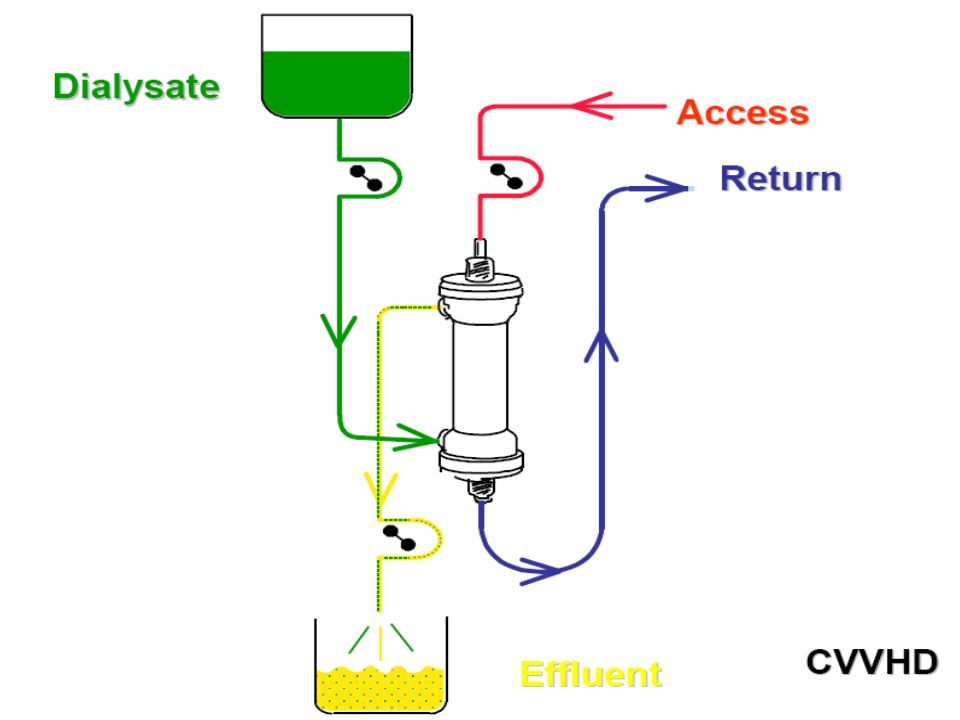
Continuous Veno-venous Hemodialysis (CVVHD)
Effective for removal of small to medium sized molecules. Solute removal occurs primarily due to diffusion. No replacement fluid is used. Dialysate is run on the opposite side of the filter. Fluid in the effluent bag is equal to the amount of fluid removed from the patient plus the dialysate.

39
CVVHD Blood flow:80 – 200 ml/min Duration
Ultrafiltration: ml/hr (or total volume) Anticoagulation Dialysate: 600 – 1800 ml/hr (up to 3 lit/hr). NO replacement fluid
 Anticoagulation. Dialysate: 600 – 1800 ml/hr (up to 3 lit/hr). NO replacement fluid.")
40
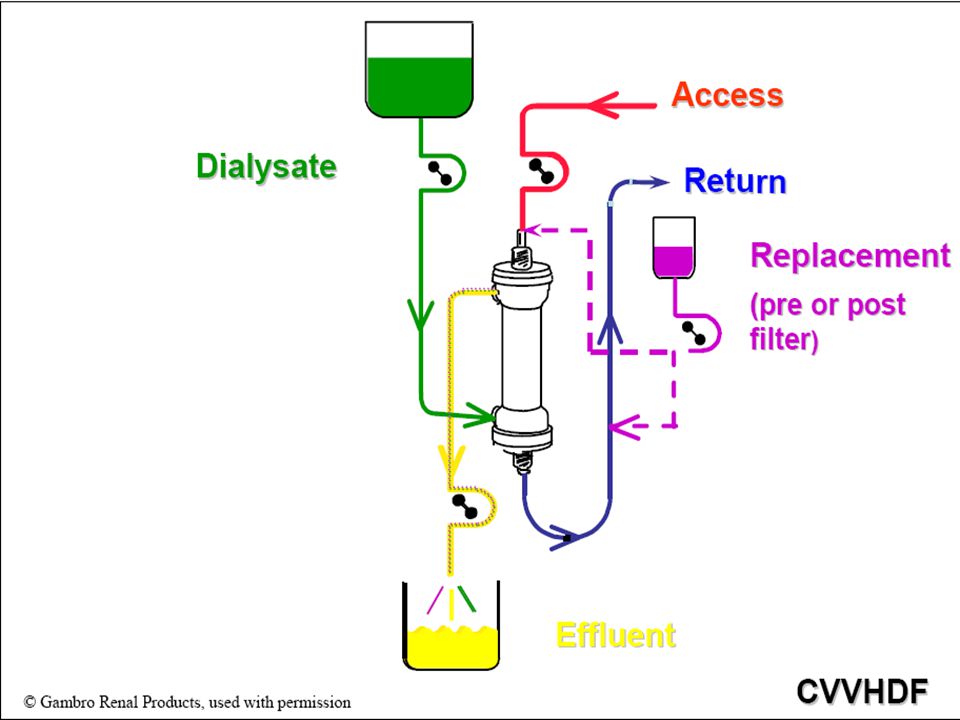
Continuous Veno-venous Hemodiafiltration (CVVHDF)
The most flexible of all the therapies, and combines the benefits of diffusion and convection for solute removal. The use of replacement fluid allows adequate solute removal even with zero or positive net fluid balance for the patient. Amount of fluid in the effluent bag equals the fluid removed from the patient plus the dialysate and the replacement fluid. Dialysate on the opposite side of the filter and replacement fluid either before or after the filter.

42
CVVHDF Blood flow: 80 – 200 ml/min Duration
Ultrafiltration: ml/hr (or total volume) Anticoagulation Dialysate: 600 – 1800 ml/hr (up to 3 lit/hr). Replacement fluid: ml/hr, pre or post filter (up to 3 lit/hr).
 Anticoagulation. Dialysate: 600 – 1800 ml/hr (up to 3 lit/hr). Replacement fluid: ml/hr, pre or post filter (up to 3 lit/hr).")
43
Anticoagulation & CRRT
Low-dose pre-filter unfractionated Heparin: any dose less than 5 units/kg/hour. Medium-dose pre-filter unfractionated Heparin: a dose between 8-10 units/kg/hour. Systemic unfractionated Heparin is administered intravenously and titrated to achieve an activated partial thromboplastin time (aPTT) ordered by the physician, for patients who have another indication for heparinization, such as. DVT Regional unfractionated Heparin: a pre-filter dose of 1500 units/hour of Heparin, with administration of Protamine post-filter at a dose of mg/hour. Low-molecular-weight Heparins Prostacyclin: rarely used (expensive, hypotension) Citrate: infused pre-filter, Ca must be replaced.
 ordered by the physician, for patients who have another indication for heparinization, such as. DVT. Regional unfractionated Heparin: a pre-filter dose of 1500 units/hour of Heparin, with administration of Protamine post-filter at a dose of mg/hour. Low-molecular-weight Heparins. Prostacyclin: rarely used (expensive, hypotension) Citrate: infused pre-filter, Ca must be replaced.")
44
No Anticoagulation Platelet count < 50,000/mm3 INR > 2.0
aPTT > 60 seconds Actively bleeding or with an active bleeding episode in the last 24 hours Severe hepatic dysfunction or recent liver transplantation Within 24 hours post cardiopulmonary bypass or extra-corporeal membrane oxygenation (ECMO)
")
45
Complications of CRRT Bleeding Hypothermia Electrolyte imbalance
Acid-base imbalance Infection Dosing of medications

46
Continuous Renal Replacement Therapy CRRT
WHAT Is CRRT HOW To use CRRT HOW To use CRRT

47
When to start CRRT. IHD Vs CRRT. Dose of CRRT. Anticoagulation and CRRT. Nutrition and CRRT. Drug doses in CRRT. Ethical issues of CRRT.

48
When to start CRRT

50
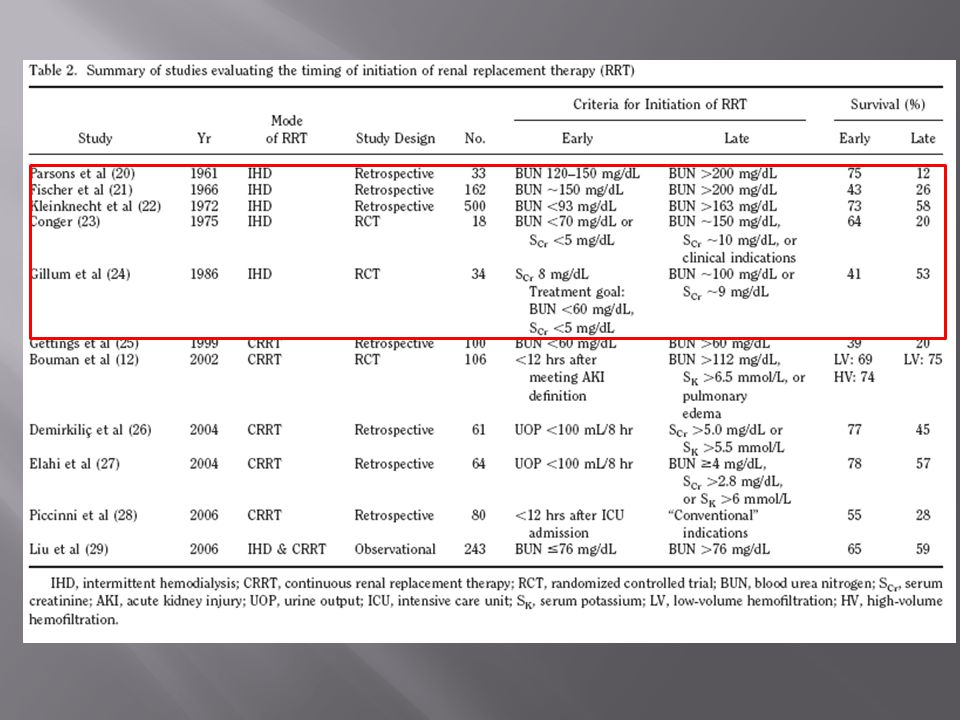
Moving On Further studies focused mostly on the timing of initiation of CRRT Gettings et al published a retrospective analysis of 100 consecutive patients with post traumatic AKI in 1999 Early vs late initiation based on BUN < or > 60 mg/dL at initiation of therapy

51
Cont. Early group Late group
CRRT initiated on hospital day 10+15 Mean BUN of 43+13 Late group CRRT initiated on HD mg/dl BUN of mg/dl Survival – 39% in early Vs 20% in late group

52
Critical points: Non-randomized, retrospective
More pts with multi-system organ failure or sepsis in late group More pts oliguric on first day of CRRT in early than late group, leading to suggestion that there was a confounding effect (?physician bias)
")
53
How about a prospective study of CRRT timing?
Bouman et al (2002)randomized 106 critically ill patients with AKI to three groups: Early high-volume CVVHDF (35 pts) Early low-volume CVVHDF (35 pts) Late low-volume CVVHDF (36 pts) Two early groups – txt started within 12 hrs of meeting inclusion criteria: Oliguria x 6 hrs despite hemodynamic optimization Measured cr clearance <20 ml/min on a 3-hr timed collection Late groups: BUN>112 K>6.5 Pulmonary edema present
randomized 106 critically ill patients with AKI to three groups: Early high-volume CVVHDF (35 pts) Early low-volume CVVHDF (35 pts) Late low-volume CVVHDF (36 pts) Two early groups – txt started within 12 hrs of meeting inclusion criteria: Oliguria x 6 hrs despite hemodynamic optimization. Measured cr clearance <20 ml/min on a 3-hr timed collection. Late groups: BUN>112. K>6.5. Pulmonary edema present.")
54
Outcome No significant differences in survival were observed
Critical point is that 28-day mortality was only 27%, much lower than in previously reported studies of critically ill patients with AKI Small sample size lead to low statistical power Interestingly, 6/36 pts in late group never got RRT (2 pts died and 4 pts recovered renal function)
")
56
Early Renal Replacement Therapy in Patients with Postoperative Acute Liver Failure Associated with Acute Renal Failure: Effect on Postoperative Outcomes Patients were divided into early or late dialysis groups based on an arbitrary blood urea nitrogen cut-off level of 80 mg/dL before renal replacement therapy. Earlier initiation of renal replacement therapy, based on the predialysis blood urea nitrogen level, with continuous venous-venous hemofiltration might provide a better ICU survival rate. Journal of the American College of Surgeons Volume 205, Issue 2, August 2007, Pages

57
The Randomized Evaluation of Normal versus Augmented Level of renal replacement (RENAL) Study NEJM 2009 multi-center, randomized controlled trial with 1,508 critically ill AKI patients in Australia and New Zealand. 2 groups: higher-intensity group (CRRT dose of 40 mL/kg/hr) or a lower-intensity group (CRRT dose of 25 mL/kg/hr). Early initiation may have contributed to excellent outcomes (mean, 50 hours).
 or a lower-intensity group (CRRT dose of 25 mL/kg/hr). Early initiation may have contributed to excellent outcomes (mean, 50 hours).")
58
So When Do We Initiate RRT?
Inadequate data available to answer this question Observational data suggests better outcomes are associated with early RRT initiation ? If “less sick” patients are included in these early groups Also, many patients with AKI are not treated with RRT

59
IHD Vs CRRT

61
Objective: The impact of CRRT and IHD on renal recovery.
Design: retrospective cohort study between the years 1995 and Follow-up ranged between 3 months and 10 years. Patients: 2202 90 days survival: 85.7% with CRRT, 14.3% with IHD

63
Conclusions: Although further study is needed, this study suggests that renal recovery may be better after CRRT than IHD for ARF. Mortality was not affected significantly by RRT mode.

65
Objectives: To estimate the impact of hemodialysis modality on patient outcome.
Design: Prospective multicenter observational study conducted from March 1996 to May 1997. 28 ICUs, 587 patients, France. Conclusions: Renal replacement therapy mode was not found to have any prognostic value. Randomized controlled trials should be undertaken to assess this important question.

66
DOSE of RRT

67
The concept of RRT dose is part of the required knowledge for a safe and effective delivery of therapy. As is the case for antibiotics, vasopressors, anti-inflammatory drugs, mechanical ventilation, etc. In chronic kidney disease, urea often has been used as a marker molecule. The amount (dose) of delivered RRT can be described by various terms: efficiency, intensity, frequency, and clinical efficacy.
 of delivered RRT can be described by various terms: efficiency, intensity, frequency, and clinical efficacy.")
68
Efficiency (K) The volume of blood cleared of a given solute over a given time. (mL/min, mL/hr, L/hr, L/24 hrs, etc.) During RRT, K depends on solute molecular size and diffusivity, transport modality (convection or diffusion), and circuit operational characteristics such as blood flow rate, ultrafiltration rate, dialysate flow rate, and membrane and hemodialyzer type and size.
, and circuit operational characteristics such as blood flow rate, ultrafiltration rate, dialysate flow rate, and membrane and hemodialyzer type and size.")
69
Intensity (Kt) Defined as: The product of K X time.
(Kt: mL/min X 24 hrs, L/hr X 4 hrs, etc.) Kt is more useful than K in comparing various RRTs. Nevertheless, equal Kt products may lead to different results if K is large and t is small or if K is small and t is large.
 Kt is more useful than K in comparing various RRTs. Nevertheless, equal Kt products may lead to different results if K is large and t is small or if K is small and t is large.")
70
Efficacy (Kt/V) The effective outcome resulting from the administration of a given treatment dose to a given patient. V: is the volume of distribution of the marker molecule in the body. Kt/V is a dimensionless number(e.g., 3 L/hr X 24 hrs/45 L = 72 L/45 L = 1.6)
")
71
Limitations The marker solute cannot and does not represent all of the solutes that accumulate in renal failure. Its kinetics and volume of distribution are also different from other solutes. Finally, its removal during RRT is not representative of the removal of other solutes. This is true for both end-stage renal failure and acute renal failure.

72
Brause et al. (2008), using CVVH, found that higher Kt/V values (0
Brause et al. (2008), using CVVH, found that higher Kt/V values (0.8 versus 0.53) were correlated with improved uremic control and acid-base balance. Paganini EP (2001):A mean Kt/V >1.0 was associated with increased survival. Ronco C (2000): A randomized, controlled trial of CRRT dose, CVVH at 35 or 45ml/kg per h was associated with improved survival when compared with 20 ml/kg per h in 425 critically ill patients with ARF .
, using CVVH, found that higher Kt/V values (0.8 versus 0.53) were correlated with improved uremic control and acid-base balance. Paganini EP (2001):A mean Kt/V >1.0 was associated with increased survival. Ronco C (2000): A randomized, controlled trial of CRRT dose, CVVH at 35 or 45ml/kg per h was associated with improved survival when compared with 20 ml/kg per h in 425 critically ill patients with ARF .")
73
Effects of different doses in CVVH on outcome of ARF - Ronco & Bellomo study. Lancet . july 00
100 90 80 70 60 50 40 30 20 10 Group 1(n=146) ( Uf = 20 ml/kg/hr) Group 2 (n=139) = 35 ml/kg/hr) Group 3 (n=140) = 45 ml/kg/hr) 41 % 57 % 58 % p < 0.001 p n.s. Survival (%) This is a another way to visually see the outcome from Dr. Ronco’s study. Group 1 is what we consider conventional delivery with poor patient outcome. Group 2 and 3 prove that a higher dose improves patient survival. Group 2 and 3 showed very little difference in survival therefore, the new dosing standard was announced that a dose of 35 mL/hr/kg improved patient outcome.
 ( Uf. = 20 ml/kg/hr) Group 2 (n=139) = 35 ml/kg/hr) Group 3 (n=140) = 45 ml/kg/hr) 41 % 57 % 58 % p < p n.s. Survival (%) This is a another way to visually see the outcome from Dr. Ronco’s study. Group 1 is what we consider conventional delivery with poor patient outcome. Group 2 and 3 prove that a higher dose improves patient survival. Group 2 and 3 showed very little difference in survival therefore, the new dosing standard was announced that a dose of 35 mL/hr/kg improved patient outcome")
74
Bouman C et al (2002):3 groups
Early high-volume hemofiltration (72 to 96 L/24 h). Early low-volume hemofiltration (24 to 36 L/24 h). Late low-volumehemofiltration (24 to 36 L/24 h). No difference in terms of renal recovery or 28-d mortality regarding the dose.
. Early low-volume hemofiltration (24 to 36 L/24 h). Late low-volumehemofiltration (24 to 36 L/24 h). No difference in terms of renal recovery or 28-d mortality regarding the dose.")
76
Anticoagulation and CRRT

77
Why ? Prevent clotting of the circuit. Preserve filter performance.
Optimize circuit servival. Prevent loss of blood due to circuit clotting.

78
Ideal anticoagulant Should prevent filter clotting without inducing hemorrhage. Should have a short half-life, and action limited to extracorporeal circuit. Should be easily monitored. Should have No systemic side effects. Should have an antidote.

79
Anticoagulation & CRRT
Low-dose pre-filter unfractionated Heparin: any dose less than 5 units/kg/hour. Medium-dose pre-filter unfractionated Heparin: a dose between 8-10 units/kg/hour. Systemic unfractionated Heparin is administered intravenously and titrated to achieve an activated partial thromboplastin time (aPTT) ordered by the physician, for patients who have another indication for heparinization, such as. DVT Regional unfractionated Heparin: a pre-filter dose of 1500 units/hour of Heparin, with administration of Protamine post-filter at a dose of mg/hour. Low-molecular-weight Heparins Prostacyclin: rarely used (expensive, hypotension) Citrate: infused pre-filter, Ca must be replaced.
 ordered by the physician, for patients who have another indication for heparinization, such as. DVT. Regional unfractionated Heparin: a pre-filter dose of 1500 units/hour of Heparin, with administration of Protamine post-filter at a dose of mg/hour. Low-molecular-weight Heparins. Prostacyclin: rarely used (expensive, hypotension) Citrate: infused pre-filter, Ca must be replaced.")
80
Minimal systemic anticoagulation
Kozek-Langenecker et al (2002). Fiaccadori E et al (2002). Nakae H et al (2003). Attractive strategy that has its drawbacks (HIT, bleeding)
. Fiaccadori E et al (2002). Nakae H et al (2003). Attractive strategy that has its drawbacks. (HIT, bleeding)")
81
Current Opinion in Anaesthesiology 2001, 14:143-149
5000 – U of UFH added to the priming solution. Continuous infusion of 3-5 u/kg/hr. 50 – 100 % prolongation of aPTT. Incidence of bleeding varied between 0 – 50 %

82
Regional anticoagulation using Citrate
Pre-filter citrate inhibits coagulation by chelating Ca+ As a result iCa decreases. An iCa concentration below 0.35 mmol/L is required to inhibit coagulation.

83
H.M. Oudemans-Van 2009 RCT, 144 patients.
Safety and efficacy of regional anticoagulation with citrate in critically ill patients with AKF, without an increased risk of bleeding. Nadroparin group Vs Citrate group. Hb concentration lower in N group (p=0.002) ICU mortality lower in C group than N group (25% Vs 30% , p< 0.01) Hospital mortality lower in C group than N group (40% Vs 48%, p = 0.065)
 ICU mortality lower in C group than N group (25% Vs 30% , p< 0.01) Hospital mortality lower in C group than N group (40% Vs 48%, p = 0.065)")
84
Metabolic effects of citrate

85
Prospective dose finding study.
30 patients with acute or history of HIT. ARF in need of CRRT. Safety determined by: - steady state of BUN ±18.02 mg/dl - mean filter patency at 24 hrs: 98% - Bleeding episodes.

86
Argatroban loading dose of 100 µ/kg
Followed by maintenance infusion rate ( µ/kg/min) Maintenance infusion calculated by: 2.15 – 0.06 X APACHE II score Conclusion: In critically ill patients with HIT and necessity for CRRT , APACHE II can help to predict the required argatroban maintenance dose for anticoagulation. This predictor identifies decreased argatroban dosing requirements. Resulting in effective and safe CRRT.
 Maintenance infusion calculated by: 2.15 – 0.06 X APACHE II score. Conclusion: In critically ill patients with HIT and necessity for CRRT , APACHE II can help to predict the required argatroban maintenance dose for anticoagulation. This predictor identifies decreased argatroban dosing requirements. Resulting in effective and safe CRRT.")
87
What’s the point ? Anticoagulation during CRRT should be individualized. The first goal should be the safety of the patient. Attention should be paid to non-pharmacological means of prolonging filter life (blood flow, wide pore cath, pre-filter replacement fluid).
.")
88
Nutrition and CRRT

89
Nutrition Implications of ARF
ARF causes anorexia, nausea, vomiting, bleeding ARF causes rapid nitrogen loss and lean body mass loss (hypercatabolism) ARF causes ↑ gluconeogenesis with insulin resistance Dialysis causes loss of amino acids and protein Uremia toxins cause impaired glucose utilization and protein synthesis
 ARF causes ↑ gluconeogenesis with insulin resistance. Dialysis causes loss of amino acids and protein. Uremia toxins cause impaired glucose utilization and protein synthesis.")
90
Nutrient Requirements in ARF
Calories: kcals/kg dry weight or REE Protein: about g amino acids lost per day with CRRT ARF w/o HD (expected to resolve within a few days): .6-1 g pro/kg Acute HD: g/kg; acute PD: g/kg; CRRT: g/kg CHO: ~60% total calories; limit to 5 mg/kg/min; peripheral insulin resistance may limit CHO In CWHD(F) watch for CHO in dialysate or replacement fluids Fat: 20-35% of total calories; lipid clearance may be impaired
: .6-1 g pro/kg. Acute HD: g/kg; acute PD: g/kg; CRRT: g/kg. CHO: ~60% total calories; limit to 5 mg/kg/min; peripheral insulin resistance may limit CHO. In CWHD(F) watch for CHO in dialysate or replacement fluids. Fat: 20-35% of total calories; lipid clearance may be impaired.")
91
Vitamins in ARF Vitamin A: elevated vitamin A levels are known to occur with RF Vitamin B – prevent B6 deficiency by giving 10 mg pyridoxine hydrochloride/day Folate and B6: supplement when homocysteine levels are high Vitamin C: <200 mg/day to prevent ↑ oxalate Activated vitamin D Vitamin K: give Vitamin K especially to pts on antibiotics that suppress gut production of K

92
Minerals in ARF ↑ potassium, magnesium, and phos occur often due to ↓ renal clearance and ↑ protein catabolism ↓ potassium, mg and phos can occur with refeeding CRRT pts can have ↓ K+, phos Mg deficiency can cause K+ deficiency resistant to supplementation Vitamin C, copper, chromium lost with CVVH

93
Fluid in ARF Depends on residual renal function, fluid and sodium status, other losses Usually 500 mL/day + urine output Fluid replacement needs can be ↑ with CRRT

94
Drug dosing in CRRT

95
Extracorporeal removal
only the drug in the central compartment(plasma)is available for extracorporeal removal drugs with a large Vd have less access to the hemofilter or dialyzer Extracorporeal treatmentdeeper compartments the rate of extracorporeal removal the rate of transfer between the peripheral and central compartment.
is available for extracorporeal removal. drugs with a large Vd have less access to the hemofilter or dialyzer. Extracorporeal treatmentdeeper compartments. the rate of extracorporeal removal. the rate of transfer between the peripheral and central compartment.")
96
Factors determining extracorporeal drug removal a) Pharmacological
Molecular weight. Volume of distribution. Plasma protein binding. Drug charge (Gibbs-Donnan effect). Gibbs-Donan effect(the behavior of charged particles near a semi-permeable membrane to sometimes fail to distribute evenly across the two sides of the membrane)
. Gibbs-Donan effect(the behavior of charged particles near a semi-permeable membrane to sometimes fail to distribute evenly across the two sides of the membrane)")
97
Factors determining extracorporeal drug removal b) Technical
Membrane. Diffusion. Convection. Adsorption to membrane. Gibbs-Donan effect(the behavior of charged particles near a semi-permeable membrane to sometimes fail to distribute evenly across the two sides of the membrane)
")
99
Ethical Issues

101
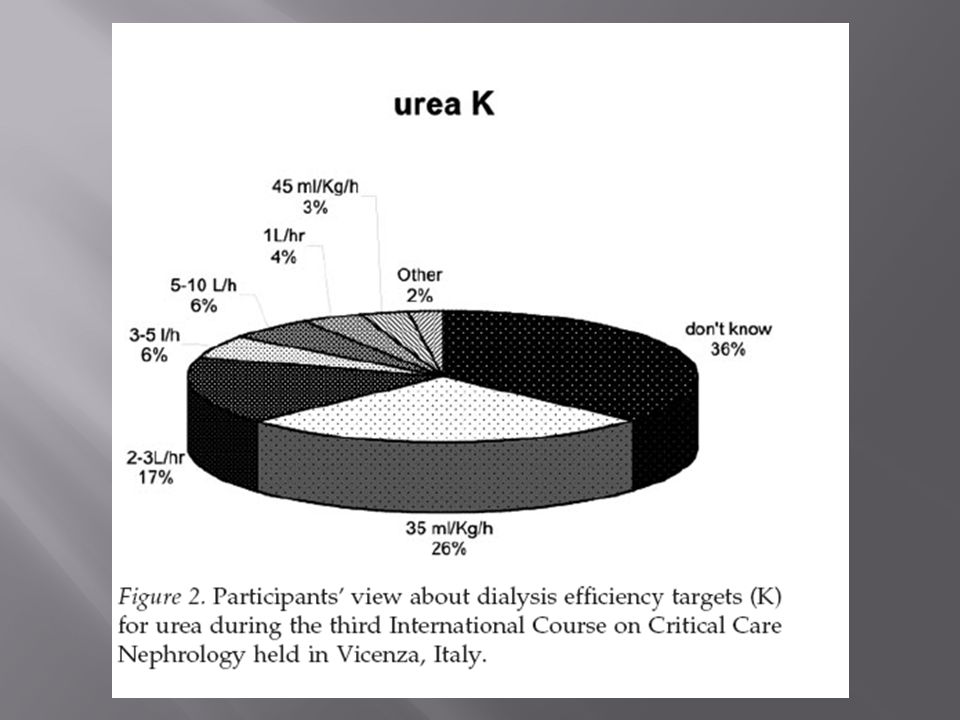
Design: A questionnaire.
Setting: The First International Course on Critical Care Nephrology. Participants: The participants in the course (around 500).
.")
102
Results Most participants think that establishing ethical criteria for managing CRRT is a medical task. Many responders would start futile CRRT or maintain it if requested by the family. Only 55% believe that informed consent is necessary for initiating CRRT. One out of four would start or maintain unwanted life-saving CRRT. Most think that every vital support should be withdrawn when futile

103
Wake Up, It’s Dinner Time
Thank You Wake Up, It’s Dinner Time

Similar presentations






















>")

