Download presentation
Presentation is loading. Please wait.

1
Jennifer Ku & Jennette Kidnie

2
Previous Theories/Beliefs
Vampires “consumption” Draining of blood making victim pale and weak Masturbation Leaving patient drained of energy Sin Creativity Patients got burst of energy- made women more beautiful and men more creative

3
History of TB Origin of Word - Tuberculosis – TB: Tubercle bacillus
Has often been referred to as ‘white plague’ and ‘consumption’ 18,000 year old bison found with Mycobacterium tuberculosis Skeletal remains of prehistoric human from 7000BC 1882 Robert Koch identifies M. tuberculosis as bacteria causing disease 1980’s multi drug resistant TB strains appear

4
First evidence/case TB
Eastern Mediterranean – 9250 to 8160 years ago TB lesions from a woman and infant buried together PCR to examine bone samples

6
What causes TB? Mycobacterium tuberculosis Less common causes:
Slow growing Acid fast bacillus Has waxy layer which prevents drying Less common causes: Mycobacterium bovis Mycobacterium africanum Mycobacterium canetti Mycobacterium microti

7
What happens when the bacteria enter the body?
In healthy individuals or when only small amounts of bacteria are ingested, active macrophages will kill bacteria The immune system will form a wall around the bacteria called a granuloma or tubercule, which can stay dormant for many years before reappearing (latent TB) In some individuals a full blown infection will occur which often leads to death (miliary TB)
 In some individuals a full blown infection will occur which often leads to death (miliary TB)")
8
Pathogenesis Taken from figure 19-1 in Salyers and Whitt, 2002

9
Pathogenesis cont’d Miliary TB- TB infection in the lung that results in the bacteria getting into the pulmonary vein and going systemic If untreated it is 100% fatal In 25% of the cases, it will cross blood-brain barrier and cause tuberculous meningitis

10
How does it escape the macrophages?
M. tuberculosis is able to survive and grow within unactivated macrophages Prevent fusion with lysosome (oxidative burst) due to waxy coated capsule Inhibits IL-12 production which will prevent TH1 response
 due to waxy coated capsule. Inhibits IL-12 production which will prevent TH1 response.")
11
Host Protection Important defenses:
the T helper cells (CD4+) producing IFN-γ which will stimulate macrophage activation the cytotoxic (CD8+) T cells killing infected phagosomes that have been unable to destroy the bacteria
 producing IFN-γ which will stimulate macrophage activation. the cytotoxic (CD8+) T cells killing infected phagosomes that have been unable to destroy the bacteria.")
12
Transmission Respiratory droplets from coughing, sneezing, talking, or spitting Aerosol droplets 0.5 to 5µm in diameter A single sneeze can release up to 40, 000 droplets

13
Transmission Infectious dose of tuberculosis is very low
Inhalation of just a single bacterium can cause a new infection. Dormant, which can later cause disease if weakened Mechanism of transmission: People who inject drugs using unsanitary needles Residents and employees of high-risk congregate settings Medically under-served and low-income populations Children exposed to adults in high-risk categories Patients immunocompromised (i.e. HIV/AIDS) Immunosuppressant drugs Health care workers serving high-risk patients
 Immunosuppressant drugs. Health care workers serving high-risk patients.")
14
Transmission Transmission can only occur from people with active — not latent — TB Factors influencing effective transmission: Number of infectious droplets expelled by a carrier The effectiveness of ventilation The duration of exposure The virulence of the M. tuberculosis strain

15
Common Symptoms Chronic cough Blood in sputum Fever Night sweats
Weight loss If it travels to other organs than the lungs, then a wider range of symptoms may occur

16
Diagnosis Tuberculin Skin Test Chest Radiograph
Bacteriological Smears & Cultures Clinical Observations

17
Diagnosis- TB Test Tuberculin injected intradermally
Sensitivity of this extract that the bacteria produces will appear as red circle Those immunized or have previously had the infection will show the same result as those that now have the disease Patient Status Positive Result HIV + >5mm Healthy individuals with exposure history or risk factors >10mm Healthy individuals with no exposure history >15mm

18
X-ray of Far-advanced Tuberculosis
The white arrows show bilateral pulmonary infiltrate, black arrows show caving formation

19
Bacteriological Smears & Cultures
Sputum smear is tested for the presence of Acid-Fast-Bacilli Negative result will rule out TB infection. Most definitive diagnosis will come from culture of lung secretions Positive Acid-Fast stain of TB M. Tuberculosis culture

20
Clinical Observations
Clinical signs of active infection: Fatigue, fever, unexplained weight loss, night sweats. Symptoms of pulmonary TB include: Productive cough >3 weeks, coughing up blood, and chest pain. Extra-pulmonary TB will have a range of signs and symptoms depending on the site of primary infection.

21
Treatment in a time before antibiotics
Sanatoriums for both the rich and poor citizens First sanatorium in Canada was at Muskoka lake in 1897 Patients received rest, fresh air, good nutrition to support healing and isolation to prevent spread Closed down mid 1900s after antibiotics were found to be better at treating patients

22
What treatment is used today?
First-line drugs taken for 6-8 months Isoniazid- inhibit mycolic acid synthesis Rifampin- inhibits bacterial RNA polymerase Ethambutol- inhibit mycolic acid synthesis Pyrazidamide- nicotinamide analog Second-line drugs Streptomycin, capreomycin, clofazamine, amikacin, ethionamide, ofloxacin, ribabutin, kanamycin, fluoroquinolones

23
First-Line Treatment Taken from

24
DOT Directly Observed Treatment (DOT)
Used to deal with the high number of noncompliant patients who do not take the drugs every day for the full length of time Important since not taking the drugs as prescribed is a main cause of drug resistance Proof of its effectiveness: 1986- prior to DOT 26% of patients acquired drug resistance After thanks to DOT, drug resistance is 7%

25
Drug Resistant TB MDR-TB -> multi-drug resistant (1980s)
-resistance to 2 of the first line drugs (often isoniazid and rifampicin) XDR-TB -> extremely drug resistant -first reported outbreak was in 2006 -resistance to 2 of the first line drugs, atleast 1 quinolone and atleast 1 of the second line anti-TB injection drugs -can take 6-16 weeks to diagnose CDR-TB -> completely drug resistant -resistance to all known drugs
 XDR-TB -> extremely drug resistant. -first reported outbreak was in resistance to 2 of the first line drugs, atleast 1 quinolone and atleast 1 of the second line anti-TB injection drugs. -can take 6-16 weeks to diagnose. CDR-TB -> completely drug resistant. -resistance to all known drugs.")
26
Prevention Screening Programs Vaccine:
Testing those in high risk groups Vaccine: BCG (Bacillus Calmette-Guerin) Developed in the 1920’s Live, attenuated M. Bovis strains Only lasts ~15 years Given to children to prevent TB meningitis or miliary TB Effectiveness ranging from 0%-80% Use was previously widespread in Canada
 Developed in the 1920’s. Live, attenuated M. Bovis strains. Only lasts ~15 years. Given to children to prevent TB meningitis or miliary TB. Effectiveness ranging from 0%-80% Use was previously widespread in Canada.")
27
Recent Use of BCG Vaccine
Who qualifies for a BCG vaccine? Children of families with a strong history of TB Groups of people that display an uncommonly high rate of infection. Health care workers who are working with the bacteria or patients Newborn infants whose mother has infectious TB at the time of delivery Individuals travelling to TB-laden areas for an extended period of time (i.e. six months or more).
.")
28
The Problem with BCG Variable efficiency. Reasons may include:
Interference with non-tuberculous mycobacteria Genetic variation in BCG strains Genetic variation in the population Severe local inflammation and scarring occurring in patients Tuberculin skin test must be performed first and if positive then they can’t vaccinate Immunocompromised individuals often will get a miliary TB infection

29
Epidemiology

30
Epidemiology Annually, 8 million people become ill with tuberculosis
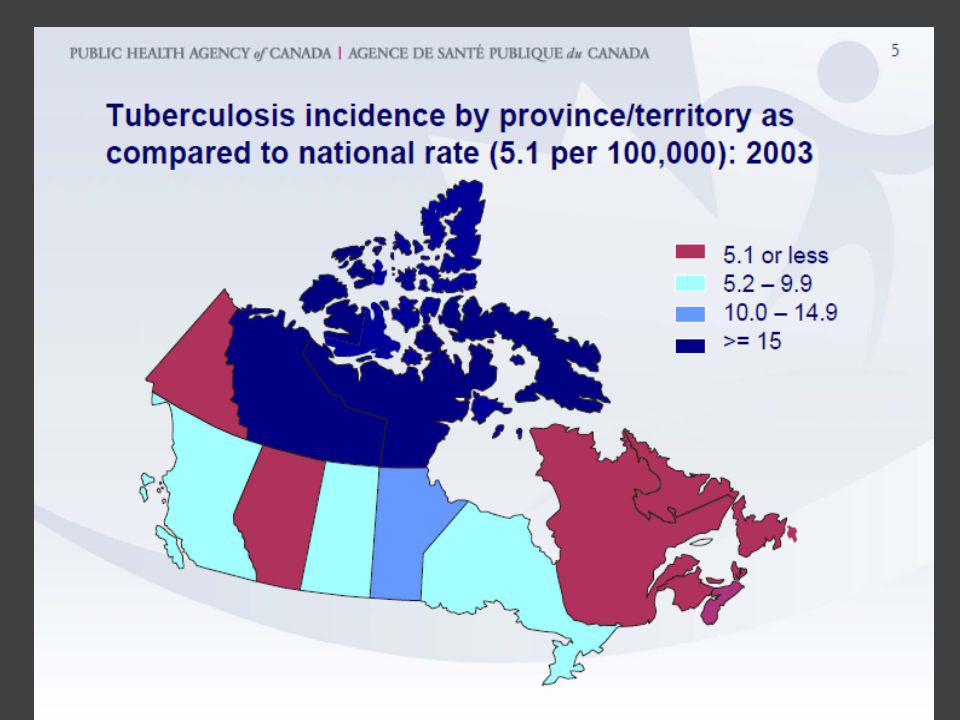
2 million people will die from the disease, worldwide Growing problem In 2004: 14.6 million people active TB disease 9 million new cases In Canada, still an endemic Northwest Territories

31
Annual Incidence by Country
# (per 100, 000) Africa 356 North & South America 41 Switzerland (2005) 1262 London 40 Portugal 31.3 China 113 Brazil 64 United States 4.9
 Africa North & South America. 41. Switzerland (2005) London. 40. Portugal China Brazil. 64. United States")
32
Global Impact

33
Reasons for re-emergence
↑ HIV infections Neglect of TB control programs Drug-resistant strains ↑ migration, international travel, and tourism ↑ incidence of AIDS

38
What will make you more susceptible to TB?
Co-infection with HIV Smoking (>20 cigarettes/day) ↑ risk by 2x-4x Diabetes mellitus Hodgkin lymphoma, End-stage renal disease Chronic lung disease Malnutrition Alcoholism
 ↑ risk by 2x-4x. Diabetes mellitus. Hodgkin lymphoma, End-stage renal disease. Chronic lung disease. Malnutrition. Alcoholism.")
39
QUESTIONS?

Similar presentations


















 is an infectious disease caused by bacteria whose scientific name is Mycobacterium tuberculosis. It was first isolated.>")

 Facts>")


