Download presentation
Presentation is loading. Please wait.

1
Frozen shoulder Shoulder injections
Mr Lee Van Rensburg November 2011

3
www.cambridgeorthopaedics.com office@cambridgemedicalpractice.co.uk
Rheumatology 2006;45:215–221

5
Overview Introduction Anatomy Clinical Injections

6
Prevalence Prevalence of shoulder pain - adults
7% overall 26% in elderly Only 20-50% present to primary care 1% of primary care consultations 20% referred to secondary care Over 50% only 1 consultation Rheumatology 2006;45:215–221

7
Rheumatology 2006;45:215–221

8
Shoulder pain Common Most get better on own
Time Analgesia - NSAID If not better by 3 months refer?

9
Referral GP 1 Diffuse pain in upper arm, spontaneous onset
Hawkins impingement +ve Painful arc Subacromial impingement Physio

10
Physiotherapy Sees physio - 2 weeks later
Physio examines patient - “tendonitis” Starts treatment, pain gets worse Refers back to GP some biceps signs Biceps tendonitis ? Slap tear

11
Referral GP 2 Unable to sleep
Difficult to examine, slightly reduced ROM Weakness of shoulder ? Rotator cuff tear Refer specialist ? Needs MRI

12
Patient Impingement Tendonitis Problem biceps tendon – SLAP tear
Rotator cuff tear Special scan Getting worse Can’t sleep Chew arm off

13
? Specialist Thank you for the referral
Pain in shoulder last months Limited ROM No External rotation Normal x rays No need for scan FROZEN SHOULDER

14
Frozen shoulder

15
VOL. 85-B, No. 6, AUGUST 2003

16
123 Tests

17
Supraspinatus - Apley's Scratch Test - Jobes Supraspinatus test - Dawburn's sign - Sherry Party sign - Codman's Sign (Drop Arm Sign) - Rent Test - Zero Degree Abduction Test - Burkhead's Thumbs down & Burkhead's Thumbs up
 - Rent Test - Zero Degree Abduction Test - Burkhead s Thumbs down & Burkhead s Thumbs up.")
18
175 J Shoulder Elbow Surg Jul-Aug;18(4):529-34
:529-34")
19
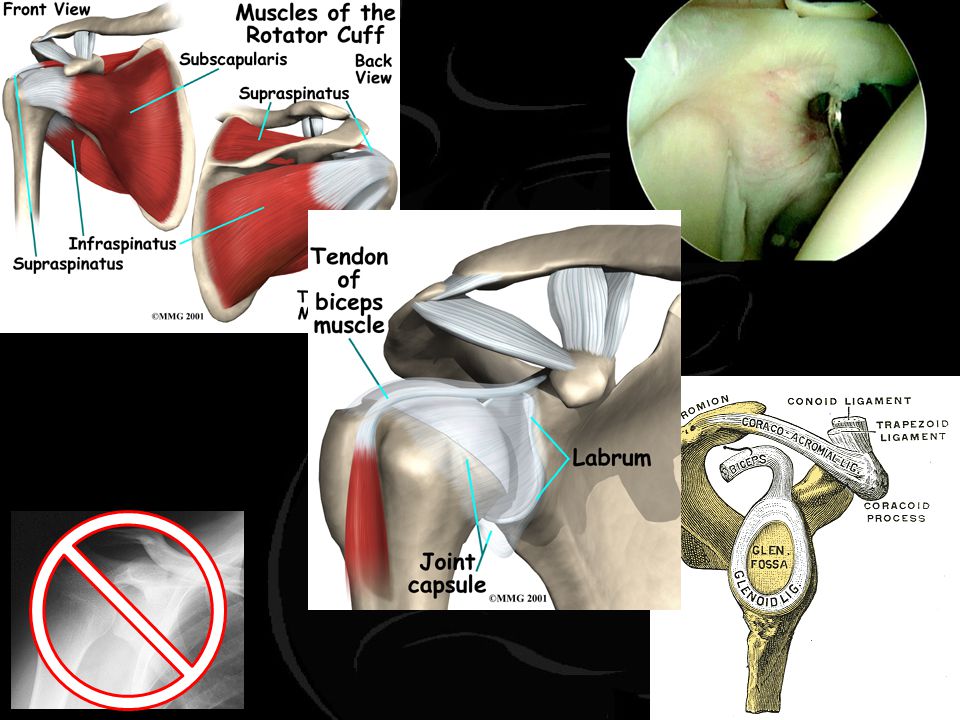
Anatomy Rotator Cuff Muscles

20
Anatomy Glenoid Labrum

21
Anatomy Capsule/Glenohumeral Ligaments

22
Overview Differential Shoulder Assessment Primary care shoulder pain
Acromioclavicular disorders Rotator cuff disorders Glenohumeral disorders Frozen shoulder Arthritis Instability Injections

23
Differential by age < 20 years 20 – 40 years > 40 years
Instability Trauma Labral pathology Biceps pathology Tendonitis Frozen shoulder Rotator cuff dz Osteoarthritis Tumor

24
Shoulder history General Specific Instability Rotator cuff and ACJ
Age, dominance, occupation, hobbies General health Specific Pain – sleep, night pain Weakness Stiffness Rx so far Instability Rotator cuff and ACJ Arthritis

25
Examination Look Feel Move Special Tests COMPARE SIDES

26
Neck Examination Referred pain Cervical Spine Thoracic Spine
Cardiac Disease

27
Look Muscles Deformity Scapulohumeral rhythm Wasting Winging Malunion
Scars ACJ Scapulohumeral rhythm

28
Scapulo-humeral rhythm
Arm Elevation (Abduction) Glenohumeral & Scapulothoracic Jts Variable Contribution Compare sides EXPOSE AND EXAMINE FROM BEHIND
 Glenohumeral & Scapulothoracic Jts. Variable Contribution. Compare sides. EXPOSE AND EXAMINE FROM BEHIND.")
29
Feel Sternoclavicular joint Clavicle ACJ Trapezius/ parascapula Neck

30
Move Compare sides (great variation) Passive v Active Loss of Motion
- Mechanical - Muscular - Pain Inhibition - Neurological

31
External rotation

32
Forward flexion

33
Abduction

34
Internal rotation

35
Special tests Rotator Cuff Disease Instability

36
Rotator cuff disease Muscle Strength Impingement ACjt Pathology
Biceps Pathology

37
Supraspinatus Jobe’s

38
Posterior cuff ER against resistance

39
Subscapularis Gerber’s

40
Subscapularis Napolean

41
Subscapularis Napolean

42
Impingement Neer’s Painful arc

43
Impingement Hawkin’s

44
AC Joint Scarfe’s

45
Biceps Speed’s

46
Biceps Yergason’s

47
Labrum O’Brien’s

48
Normal X rays

49
Arthritis

50
Calcific tendonitis

51
Normal x rays

53
…….. Perhaps this patient needs an MRI scan
60-69 =30% FTRCT 70-79 = 50% FTRCT 80-89 = 80% FTRCT Age-related prevalence of rotator cuff tears in asymptomatic shoulders; Tempelhof et al; JSES July 1999 (Vol. 8, Issue 4, Pg

54
104 shoulders chronic, atraumatic shoulder pain
History, physical examination, radiographs 41% had pre evaluation MRI scans Majority of pre-evaluation MRI scans had no impact on the outcome 90% no value Routine pre-evaluation with MRI does not appear to have a significant effect on the treatment or outcome JSES 2005;14:

55
MRI Atypical Mechanical integrity Rarities Previously prior to surgery
Although it hurts your coming to no harm Rarities Previously prior to surgery ALL rotator cuffs arthroscopically

56
59 YO male Coronal PDFS (T2)
")
57
29 YO Lymphoma Steroids Avascular necrosis

58
Right

59
36 YO male severe pain

60
72 YO Male Bilateral shoulder pain
4 Years post hemi Persistent pain Made no better

61
SHOULDER PAIN Coming from shoulder Instability Rotator cuff, ACJ
Referred, neck Instability Rotator cuff, ACJ Impingement Tear (degenerate) Tendonitis (calcific) Glenohumeral Arthritis Frozen shoulder BMJ 2005;331:1124–8
 Tendonitis (calcific) Glenohumeral. Arthritis. Frozen shoulder. BMJ 2005;331:1124–8.")
62
ACJ Pain top of shoulder Pain worst arm abducted 90°
Unable to lie on it Point tender ACJ Scarfe’s crossed adduction Reassurance Analgesia Steroid injection Arthroscopic excision

63
Rotator cuff - Impingement
Pain deltoid tuberosity Reaching back, coat, bra Painful arc Impingement No real weakness of cuff Orthotherapy Relative rest NSAID Physiotherapy Steroid injection Arthroscopic Subacromial decompression

64
Rotator cuff - tear Acute tear Degenerate tear Previously normal
Fall or similar Now unable to elevate Passive good elevation ? Earlier surgery Degenerate tear Impingement weakness Orthotherapy Arthroscopic rotator cuff repair

65
Rotator cuff - calcific
Acute pain Chew arm off in night Exclude infection Radiograph Orthotherapy Needle barbotage Arthroscopic decompression and needle barbotage

66
Glenohumeral Stiff painful shoulder Reduced ROM
Similar active and passive No ER Scapulothoracic movement Radiograph Frozen shoulder Arthritis

67
Frozen shoulder Three phases Symptoms and signs depend on phase
Inflammatory phase Frozen phase Thawing phase Symptoms and signs depend on phase Diabetic 2 years

68
VOL. 85-B, No. 6, AUGUST 2003

69
Frozen shoulder Treatment Physiotherapy Steroid injection
Hydrodilatation Manipulation under anaesthetic Arthroscopic capsular release

70
Arthroscopic shoulder surgery
ASD & ACJ Day case overnight stay 60-80% better ASD sling 2-3 weeks Drive 4-6 weeks Desk top 4-6 weeks Manual work 3 months RCR Tendon healing times Stabilisation Arthroscopic less stiffness

71
Injections about the shoulder
See separate presentation top of the list updated

Similar presentations