Download presentation
Presentation is loading. Please wait.

1
Hospital Incident Command System Train-The-Trainer Course
National Disaster Medical System (NDMS) Conference March 16-18, 2007 Center for HICS Education and Training
 Conference. March 16-18, Center for HICS Education and Training.")
2
Course Expectations Why are you here today?

3
Course Objectives Outline the historical development of HEICS and HICS
Discuss NIMS Implementation Activities for hospitals Learn the principal concepts and features of HICS Understand the roles and relationships of the Incident Management Team

4
Course Objectives (2) Understand the application and use of the HICS elements Conduct a facilitated, scenario-based exercise Discuss train-the-trainer strategies for implementing and teaching HICS

5
Education and Training
This course is presented by: The Center for HICS Education and Training The Center is a collaborative effort between the ER 1 Institute at Washington Hospital Center and Kaiser Permanente Our mission is to provide information, education and training on HICS The Center’s Advisory Board consists of National Workgroup and Ex-officio members from the HEICS 4 project The Center sponsors a webpage for additional info and updates on HICS utilization at

6
Course Faculty Craig DeAtley, PA-C Ann Potter, RN, CEM Peter Brewster
Director – Institute for Public Health Emergency Readiness, Washington Hospital Center Ann Potter, RN, CEM Chief, Disaster Preparedness Division Office of Emergency Services and Homeland Security Peter Brewster Education/Training Manager Department of Veteran’s Affairs Emergency Management Strategic Healthcare Group Craig Thorne, MD, MPH Medical Director, Employee Health & Safety University of Maryland Medical Center

7
Housekeeping Notes All technology to “silent” or “vibrate” please
If you must take or make a call Wait for a break Leave the room for calls We will have regular breaks during the course Please stay within the announced break times Restroom location(s) Emergency exits There will be time for Q&A- save your questions to the announced periods Please consult with the instructors during breaks if needed Your evaluations are important to us! Complete the evaluation form by the end of the day!
 Emergency exits. There will be time for Q&A- save your questions to the announced periods. Please consult with the instructors during breaks if needed. Your evaluations are important to us! Complete the evaluation form by the end of the day!")
8
Day 1 Agenda NIMS Implementation Activities for Hospital and Healthcare Organizations Origins of HICS Overview of HICS Components The Hospital Incident Command System Job Actions Sheets Incident Planning & Response Guides Forms Discuss relationship of the hospital to its community partners Learn about adapting HICS to rural and small facilities Course Evaluation and Wrap Up

9
Course Copyright The HICS course materials are proprietary and cannot be duplicated, reproduced or utilized without written permission of The Center No cameras or video taping or recording of this program are permitted

10
Emergency Response Is Not Business as Usual !

11
What is the Hospital Goal?
Preparedness Develop effective Emergency Management and Operations Plans Response Ensure safety of patients, personnel and facility Triage, treat, transfer and disposition victims Ensure business continuity Recovery Operational/Business Recovery Financial recovery Restoration of “normal” operations

12
Implementation Activities for Hospitals and Healthcare Systems
NIMS Implementation Activities for Hospitals and Healthcare Systems

13
NIMS Implementation Activities for Hospitals and Healthcare Systems
Document September 12, 2006 Developed by NIC and DHHS Outlines the 17 Implementation Activities for hospitals National Bioterrorism Hospital Preparedness Program (HBHPP), administered through HRSA, outlines compliance for FY 2006 funding cycle Training: ICS 100 and 200 and IS 700
, administered through HRSA, outlines compliance for FY 2006 funding cycle. Training: ICS 100 and 200 and IS 700.")
14
NIMS Implementation Activities for Hospitals and Healthcare Systems
Implementation document outlines: The element Element’s association to NIMS Implementation Guidance Implementation Example References

15
NIMS Implementation Activities for Hospitals and Healthcare Systems
NIMS Implementation Activities have seven categories: Organizational Adoption of NIMS Command and Management Preparedness Planning Preparedness Training Preparedness Exercises Resource Management Communication and Information Management

16
NIMS Implementation Elements Organizational Adoption
Element 1– Adoption of NIMS Adopt NIMS throughout the organization Implementation Guidance: Plan for full implementation A “Phased In Approach” Hospitals should develop a plan, strategy and timeline to implement the elements It can be implemented over time!!! Not immediate or all at once! NBHPP outlines implementation elements Example: All 17 elements are included in the hospital’s Emergency Management Program (EMP) The implementation of NIMS into the organization can be done over a period of time, could be 1, 2, or five years. The NIMS guidance states that hospitals should have a plan for implementation. This is good news, hospitals can implement the mandated elements (mandated by HRSA) first, and then develop a strategy and timeline to phase in the rest of the elements!
 The implementation of NIMS into the organization can be done over a period of time, could be 1, 2, or five years. The NIMS guidance states that hospitals should have a plan for implementation. This is good news, hospitals can implement the mandated elements (mandated by HRSA) first, and then develop a strategy and timeline to phase in the rest of the elements!")
17
NIMS Implementation Elements Command and Management
Element 2 – Incident Command System Manage all emergency incidents, exercises and preplanned events in accordance with ICS Must include Incident Action Planning (IAP) Common communication plans Adopting HICS will ensure element compliance Example: Emergency Operations Plan (EOP) explains the use of ICS, IAP and common communication planning
 Common communication plans. Adopting HICS will ensure element compliance. Example: Emergency Operations Plan (EOP) explains the use of ICS, IAP and common communication planning.")
18
NIMS Implementation Elements Command and Management
Element 3 – Multiagency Coordination System Develop and coordinate connectivity capability with the HCC and the local ICP, 911 centers, EOCs and the State EOC and others, if applicable Implementation Guidance: Once local/regional MAC is established, hospitals should participate in collaborative planning Exercises and training should be conducted Example: The EOP demonstrates the management and coordination between the HCC and multiagency coordination system entities

19
NIMS Implementation Elements Command and Management
Element 4 – Public Information System Implements plans to communicate through a JIS or JIC Implementation Guidance: Hospital should identify at least one PIO, representative or spokesperson responsible for media and public info Establish pre-event working relationships with local media, emergency management, law enforcement, public health, EMS etc. Example: The EOP explains the management of public info with partners

20
NIMS Implementation Elements Preparedness Planning
Element 5 – NIMS Implementation Tracking Hospitals and healthcare systems will track NIMS implementation annually as part of the EMP Implementation Guidance: Hospital must self certify compliance Designate a NIMS implementation designee Example: The hospital will track implementation activities annually with a goal of improving emergency management capability

21
NIMS Implementation Elements Preparedness Planning
Element 6 – Preparedness Funding Develop and implement a system to coordinate hospital preparedness funding to employ NIMS across the organization Implementation Guidance: Collaborate with state and local government and hospital associations to identify and obtain preparedness funding State Department of Health State Office of Homeland Security State Office of Emergency Management Local public health Local emergency management

22
NIMS Implementation Elements Preparedness Planning
Element 6 – Preparedness Funding (continued) Example: The EMP includes information on local, state and federal preparedness grants received and deliverables to be achieved
 Example: The EMP includes information on local, state and federal preparedness grants received and deliverables to be achieved.")
23
NIMS Implementation Elements Preparedness Planning
Element 7 – Revise and Update Plans Revise EOP and Standard Operating Procedures (SOPs) to incorporate NIMS Planning Training Response Exercises Equipment Evaluation and corrective actions Implementation Guidance and Example: The EMP work plan reflects status of revisions to EOPs
 to incorporate NIMS. Planning. Training. Response. Exercises. Equipment. Evaluation and corrective actions. Implementation Guidance and Example: The EMP work plan reflects status of revisions to EOPs.")
24
NIMS Implementation Elements Preparedness Planning
Element 8 – Mutual Aid Agreements/MOUs Participate in and promote interagency mutual aid agreements (public and private sector and NGOs) Implementation Guidance: Establish mutual aid agreements/MOUs with: Neighboring hospitals/healthcare systems Public health departments HazMat Response Teams Local Fire and Law Enforcement Area pharmacies Medical supply vendor Share agreements with local emergency management prior to an incident occurring
 Implementation Guidance: Establish mutual aid agreements/MOUs with: Neighboring hospitals/healthcare systems. Public health departments. HazMat Response Teams. Local Fire and Law Enforcement. Area pharmacies. Medical supply vendor. Share agreements with local emergency management prior to an incident occurring.")
25
NIMS Implementation Elements Preparedness Planning
Element 8 – Mutual Aid Agreements (Continued) Example: EMP documentation includes information supporting any mutual aid agreements and/or MOUs that the facility has
 Example: EMP documentation includes information supporting any mutual aid agreements and/or MOUs that the facility has.")
26
NIMS Implementation Elements Preparedness Training
Element 9 – IS-700: NIMS: An Introduction Complete IS-700 Implementation Guidance: IS-700 should be completed by hospital personnel in a leadership role in emergency preparedness, incident management, filling ICS/HICS roles and/or emergency response Phased in training Train others as indicated (MDs, RNs, others) Example: The EMP training records track completion of IS-700.
 Example: The EMP training records track completion of IS-700.")
27
NIMS Implementation Elements Preparedness Training
Element 10 – IS-800.A: NRP Complete IS-800 Implementation Guidance: IS 800 should be completed by personnel whose primary responsibility is emergency management Hospital must track training Example: Emergency preparedness program training records track completion of IS 800 or equivalent Training by individual(s) responsible for the hospital’s emergency management program
 responsible for the hospital’s emergency management program.")
28
NIMS Implementation Elements Preparedness Training
Element 11 – ICS 100 HC and 200 HC Complete ICS 100 and 200 training or equivalent courses Implementation: IS 100: Completed by hospital personnel that would have a direct role in emergency preparedness, incident management and/or designated to fulfill ICS roles IS 200: Completed by personnel whose primary responsibility is emergency management Including middle management and administration Personnel designated to fulfill ICS roles

29
X Emergency Management Training Requirements for Hospital Personnel
Training to be completed by August 31, 2007 Recommended Levels of Training for Hospital Personnel* IS or equivalent IS or equivalent IS or equivalent IS or equivalent IS 700 or equivalent IS or equivalent Hospital personnel who are likely to assume an ICS position in the Hospital Command Center or have a primary responsibility for emergency management X Emergency Program Manager Hospital Emergency Preparedness Committee Members/persons responsible for the Emergency Management Plan * References: 1) NIMS Integration Center, NIMS Alert: NIMS Implementation Activities for Hospitals and Healthcare Systems, September 12, ) Health Resources and Services Administration, National Hospital Bioterrorism Preparedness Program, Fiscal Year 2005 Continuation Guidance, HRSA Announcement Number 5-U3R
 NIMS Integration Center, NIMS Alert: NIMS Implementation Activities for Hospitals and Healthcare Systems, September 12, ) Health Resources and Services Administration, National Hospital Bioterrorism Preparedness Program, Fiscal Year 2005 Continuation Guidance, HRSA Announcement Number 5-U3R")
30
NIMS Integration Center
Required training resources Emergency Management Institute Self-developed/State certified courses (equivalent courses) Center for HICS Education and Training For questions or correspondence on NIMS NIMS Integration Center
 Center for HICS Education and Training. For questions or correspondence on NIMS. NIMS Integration Center.")
31
NIMS Implementation Elements Preparedness Exercises
Element 12 – Training and Exercises Incorporate NIMS/ICS into internal and external local, regional and state emergency management training and exercises Implementation Guidance: Include NIMS and ICS into trainings and exercises Review plans with staff to ensure competency Example: The EMP documentation reflects the use of NIMS/ICS

32
NIMS Implementation Elements Preparedness Exercises
Element 13 – All-Hazards Exercise Program Participate in all-hazards exercises with response partners Implementation Guidance: Participate in local, regional and/or state multidiscipline/agency exercises 2/year to every 2 years. Exercise (drills, tabletops, functional or full-scale) Internal and external communications Receiving, triage, treatment and transfer of mass casualties Progress of casualties through the system Resource management Security Specialty lab testing Site/facility safety Example: EMP documents reflects participation
 Internal and external communications. Receiving, triage, treatment and transfer of mass casualties. Progress of casualties through the system. Resource management. Security. Specialty lab testing. Site/facility safety. Example: EMP documents reflects participation.")
33
NIMS Implementation Elements Preparedness Exercises
Element 14 – Corrective Actions Hospitals will incorporate corrective actions into response plans and procedures Implementation Guidance: After exercises, develop a corrective action report Actions to correct the issue/deficiency Responsible person/group to implement the action Due date for completion Incorporate correction into P&P Example: EMP documents a corrective action process

34
NIMS Implementation Elements Resource Management
Element 15 – Response Inventory Maintain an inventory of organizational response assets Implementation Guidance: Determine emergency par levels for supplies and equipment Consider stockpiling Develop MOUs for supply and resupply Example: EMP documentation includes a resource inventory Medical/surgical supplies Pharmaceuticals PPE Equipment Staffing Etc.

35
NIMS Implementation Elements Resource Management
Element 16 – Resource Allocation As permissible, incorporate national standards and guidance into acquisition programs Implementation Guidance: As possible, establish common equipment, communications and data interoperability resources with other local response partners Example: EMP emphasizes interoperability

36
NIMS Implementation Elements Communications and Information Management
Element 17 – Standard and Consistent Terminology Apply standard and consistent terminology, in plain English standards Implementation Guidance: Establish common language consistent with local emergency management, public safety and public health Use plain language (internal Emergency Codes OK) Example: EMP emphasizes the use of plain English by staff during emergencies
 Example: EMP emphasizes the use of plain English by staff during emergencies.")
37
Section Summary NIMS Activities for Hospitals and Healthcare System
Include 17 elements of activities Adopting these elements will improve a hospital’s Preparedness Response Recovery Mandated elements by August 31, 2007: Training of selected key personnel in ICS 100 HC and 200 HC IS 700: NIMS IS 800: NRP

38
Questions?

39
The Hospital Incident Command System

40
How did HICS evolve and why is it important to your hospital?
Origins of HICS How did HICS evolve and why is it important to your hospital?

41
From HEICS to HICS Inception of HEICS in 1980’s with 2 revisions in 1990’s Over 6000 hospitals across the country utilize HEICS as their response model Obvious needs surfaced pre- and post 9/11 All hazards approach Coordinated, community planning

42
HEICS IV Project Key concept: Revision of previous models
Incident Management System for: Daily operations Preplanned events Non-emergent situations A systems approach to managing an incident HEICS became HICS Not just for emergencies anymore

43
HEICS IV Project Intent and Objectives
Maintain the fundamental concepts Predictable chain of command Modular and scalable to the incident Position accountability Common language Use the Incident Command System (ICS) principles and practices ICS adapted to the unique hospital setting
 principles and practices. ICS adapted to the unique hospital setting.")
44
HEICS IV Project Intent and Objectives Intended Outcomes
Incorporate current emergency management practices Address NIMS compliance issues Integrate CBRNE events Maintain system scalability for all Develop core materials Address instructor qualifications Scaleable: hospitals both rural and urban; teaching, specialty; Use in planning, response and recovery Promote alignment with community partners through incorporation of NIMS guidelines

45
HEICS IV Project Team National Working Group Ex-Officio Members
Hospital subject matter experts Ex-Officio Members AHA, JCAHO, DHS, DHHS, ASHE, NIC, EMI, HRSA Secondary Review Group Subject matter experts from the healthcare community Executive Group California EMS Authority and Contract Support Group Contract Support Group ER One Institute at the Washington Hospital Center Kaiser National Healthcare Continuity Management

46
What’s New in HICS? All-hazards and ‘systems’ approach
A management tool Emphasizes preparedness efforts with community partners Scalable and adaptable for all hospitals Assists with NIMS compliance for hospitals and healthcare systems

47
What’s New in HICS? Uses the Incident Command System (ICS) principles and practices ICS adapted to the unique hospital setting Approved by the NIMS Integration Center (NIC), HRSA and Joint Commission FIRESCOPE ‘s inception in the 197os was a direct response to the 1907 fires season in Southern California. In 1971, Congress directed the US Forest Services to design a system to respond to these events. US Forest Service joined with CA OES, CDF and the fire depts. of Santa Barbara, LA City, LA County and , Ventura to develop FIRESCOPE.
, HRSA and Joint Commission. FIRESCOPE ‘s inception in the 197os was a direct response to the 1907 fires season in Southern California. In 1971, Congress directed the US Forest Services to design a system to respond to these events. US Forest Service joined with CA OES, CDF and the fire depts. of Santa Barbara, LA City, LA County and , Ventura to develop FIRESCOPE.")
48
New HICS Products HICS Guidebook Incident Management Team Chart
Replaces the HEICS Organizational Chart Revised for consistency with NIMS Updated Job Action Sheets Incident Planning and Response Guides Updated HICS Forms Consistent with NIMS / Standard ICS HICS Educational Materials NIMS Implementation Activities

49
Why Is HICS Important to Your Hospital?
Comply with regulatory standards and nongovernmental guidelines The Joint Commission Environment of Care 4.10 Health Resources and Services Administration Cooperative Agreements NIMS compliance and Training requirements Emergency Medical Treatment and Active Labor Act Health Insurance Portability and Accountability Act The Joint Commission has stated that while there is no mandate to implement the 17 NIMS activity elements for JCAHO accreditation, however, if a hospital does choose to implement the activities and elements, then the hospital will be in line with the emergency management requirements of the Joint Commission for accreditation (per John Fishbeck at JCAHO)
")
50
Why Is HICS Important to Your Hospital?
Comply with regulatory standards and nongovernmental guidelines OSHA 29 CFR Part Hazardous Materials Regulations Centers for Medicare and Medicaid Services National Fire Protection Association (NFPA 1600) Standard Healthcare facilities Standard 1600 – Disaster/Emergency Management American Society for Testing and Materials (ATSM) F-1288 – Guide for Planning and Response to an MCI Superfund Amendments and Reauthorization Act
 Standard 99 - Healthcare facilities. Standard 1600 – Disaster/Emergency Management. American Society for Testing and Materials (ATSM) F-1288 – Guide for Planning and Response to an MCI. Superfund Amendments and Reauthorization Act.")
51
Why Is HICS Important to Your Hospital?
Assists in coordinating the hospital’s planning and response efforts and actions Sets direction and goals in initial efforts Assists with Incident Action Planning Mission focused Manages the incident using the Incident Command System Defines roles and responsibilities Facilitates community responder communication and mutual aid

52
Why Is HICS Important to Your Hospital?
Facilitates coordination with partners Local and community (sister or “buddy”) hospitals and healthcare systems Regional Hospital Coordination Centers Public safety agencies Local Emergency Management Nongovernmental organizations (NGO)
 hospitals and healthcare systems. Regional Hospital Coordination Centers. Public safety agencies. Local Emergency Management. Nongovernmental organizations (NGO)")
53
Why Is HICS Important to Your Hospital?
Serves as the foundation for your Emergency Operations Plan HICS is NOT the EOP HICS is a system management tool

54
HICS Resources HICS Guidebook and materials
California Emergency Medical Services Authority website at: The Center for HICS Education and Training

55
Section Summary HICS is useful for daily operations, preplanned events and non-emergent situations HICS uses the Incident Command System (ICS) principles and practices ICS adapted to the unique hospital setting HICS complies with regulatory mandates Assists in coordinating the hospital’s internal and external planning, response and recovery
 principles and practices. ICS adapted to the unique hospital setting. HICS complies with regulatory mandates. Assists in coordinating the hospital’s internal and external planning, response and recovery.")
56
Questions?

57
Incident Command System
The Hospital Incident Command System

58
The HICS Guidebook

59
The HICS Guidebook Explains the critical components of HICS
Describes the use of HICS products and materials Assists with emergency management planning Guide for: Hospital planners and responders Community responders to understand and integrate hospitals into larger response

60
The HICS Guidebook The Guidebook is NOT
The definitive text on emergency preparedness Designed to comprehensively teach the principles of incident command Not the Emergency Management or Operations Plan

61
The HICS Guidebook Chapter 2 - Principles of Incident Command
Chapter 1 - Introduction to HICS History of the HEICS IV Project and transition to HICS Scope and applicability HEICS IV Project Team Chapter 2 - Principles of Incident Command History of ICS Incident management functions Incident action planning process

62
The HICS Guidebook Chapter 3 - NIMS Compliance for Hospitals
NIMS organizational system overview NIMS compliance activities for hospitals Chapter 4 - Hospital Emergency Management Program Program development All-hazards Emergency Operations Plan Hazard Vulnerability Analysis Planning Partners

63
The HICS Guidebook Chapter 5 - Hospital Incident Command System
Incident Management Team Command Operations Planning Logistics Finance / Administration Incident Command Principles and Practice

64
The HICS Guidebook Chapter 6 - Life Cycle of an Incident
Alert and Notification Situation Assessment and Monitoring Emergency Operations Plan Implementations Establishing the Hospital Command Center Building the ICS Structure Incident Action Planning Communications and Coordination Staff Health and Safety Operational Considerations Legal and Ethical Considerations Demobilization System Restoration Response Evaluation and Organizational Learning

65
The HICS Guidebook Appendices A: Incident Planning Considerations
B: HICS Incident Management Team Chart C: Using the Job Action Sheets D: Using the HICS Forms E: HEICS to HICS: Implementation Steps F: Potential Candidates for HICS Command Positions

66
The HICS Guidebook Appendices G: HEICS III to HICS Position Crosswalk
H: Working with the Scenarios, Incident Planning and Response Guides I: NIMS Implementation Activities for Hospitals and Healthcare Systems J: Recommended Resources K: HEICS IV revision project organization

67
The HICS Guidebook Educational materials
Module based Power Points presentations highlighting key HICS concepts Print materials to accompany the power points 27 scenarios to use to assist with exercise planning 14 External scenarios 13 Internal scenarios

68
The Future of HICS HICS is a living document and system
Grows and evolves as practices and hospital needs change Modifications made as lessons are learned Adapted for your hospital’s unique needs Continue to advance hospital preparedness and emergency management standardization

69
Section Summary The HICS Guidebook provides
The critical components of HICS An overview of Emergency Management principles Guidance on how to use the HICS products and materials

70
Questions?

71
Incident Management Team
Building the Incident Management Team

72
HICS IMT The IMT Depicts hospital management functions and how authority and responsibility is distributed Each of the 5 management functions is color coded Command (white or grey) Operations (red) Planning (blue) Logistics (yellow) Finance/Administration (green)
 Operations (red) Planning (blue) Logistics (yellow) Finance/Administration (green)")
73
HICS IMT Hierarchy Divisions not in HICS, but is used by ICS, mainly Fire Agencies. Strike Teams and Task Forces are more commonly used in hospitals, while single resources are not commonly used. Note: Divisions and Groups are used in ICS but not reflected in the HICS IMT

74
IMT Titles The IMT titles are distinct and standardized. This serves three important purposes: ** Allows for filling IMT positions with the most qualified persons and not by rank Assists with requesting outside resources to staff these positions Assists with clarifying the activities undertaken by specific personnel

75
IMT Hierarchy The Incident Commander Command Staff
Is the only position always activated for every incident** Has overall responsibility to manage the incident Command Staff Title: Officer Positions: Public Information Officer Safety Officer Liaison Officer Medical/Technical Specialists

76
IMT Hierarchy General Staff**: Organizational Component: Section
Title: Section Chief Role: Responsible for major functional areas of the incident IMT Positions: Operations Planning Logistics Finance/Administration

77
IMT Hierarchy Deputy Chief Role: Assistant Role:
The individual assuming the Deputy role will assist the Command Staff, Section Chiefs or Branch Directors** by performing delegated job activities or tasks as outlined by that JAS Assistant Role: A subordinate to a Command Staff or Section Chiefs who performs technical capabilities and responsibilities They may also be assigned to a Unit Leader as situational needs dictate and resources allow

78
IMT Hierarchy Branches: Title: Branch Director Role: IMT Positions:
Branches can be established Geographically or functionally** When the number of Divisions or Groups exceed the span of control for the Section Chief* Branches may also be established* In multi-disciplinary incident In multi-jurisdictional incidents Very large incidents IMT Positions: Specific to the Section’s duties Example: Medical Care Branch Director in Operations Service Branch Director in Logistics

79
IMT Hierarchy Divisions/Groups: Title: Division Supervisor Role:
Division: Divide the incident geographically Example: first floor and second floor Group: Divide the structure into functional areas of operation by the resources to perform the function IMT Positions: Divisions and Groups are not commonly used in the hospital setting Divisions and Groups are NOT REFLECTED in the HICS IMT

80
IMT Hierarchy Units: Title: Unit Leader
Role: Functional responsibility for a specific incident activity under a Section and Branch IMT Positions: Specific to the Branch’s duties Example: Inpatient Unit Leaders in the Medical Care Branch in the Operations Section Situation Unit Leader in the Planning Section Labor Pool and Credentialing Unit in the Support Branch in the Logistics Section

81
IMT Hierarchy Single Resources, Strike Teams, Task Forces
Title: Leader Role: Single Resources: An individual or piece of equipment with its personnel complement (i.e., perfusionist) A crew or team of individuals with a identified supervisor Strike Teams: A set number of similar resources (i.e., burn RNs) Task Forces: A combination of mixed resources (i.e., RNs, MDs, Techs, Secretaries) IMT Positions: These are NOT REFLECTED on the HICS IMT Can be employed by the hospital as dictated by the incident These teams report to the Unit Leader
 A crew or team of individuals with a identified supervisor. Strike Teams: A set number of similar resources (i.e., burn RNs) Task Forces: A combination of mixed resources (i.e., RNs, MDs, Techs, Secretaries) IMT Positions: These are NOT REFLECTED on the HICS IMT. Can be employed by the hospital as dictated by the incident. These teams report to the Unit Leader.")
82
Building the IMT The Incident Commander is responsible for building the Incident Command Team The IMT is built according to the incident: Scope and magnitude of the event Potential/real impact to the hospital Hospital size Available resources Special response needs (i.e., HazMat, biological, legal, IT)
")
83
Building the IMT Every incident requires certain management functions be performed The incident/problem must be evaluated A plan must be developed to address the problems The necessary resources must be assigned Outcomes and effectiveness must be evaluated Management by objectives is essential for successful Incident Action Planning**, response and recovery

84
Building the IMT The IC should appoint properly trained persons to critical Command and General Staff positions

85
Building the IMT Once appointed: IMT position titles are standardized
Section Chiefs and Branch Directors staff their own sections IMT position titles are standardized Describe the position’s role and mission rather than the person Allows the position to be filled by the most qualified rather than by seniority Facilitates requests for outside qualified personnel

86
Building the IMT The IMT reflects a reasonable “Span of Control”
Definition: The number of individuals or resources one supervisor can effectively manage** Ratio of 3-7 reporting elements per 1 supervisor The IMT structure does not exactly mirror the daily administrative structure This is purposeful Reduces role and title confusion during the response** HICS IMT Crosswalk suggests position assignments

87
IMT Crosswalk Incident Commander Planning Section Chief Logistics
Operations Section Chief Finance/Administration Public Information Officer Liaison Medical/Technical Specialist Safety Ÿ Hospital Administrator/Administrator On-Call Nursing Supervisor Chief Executive Officer Chief Operating Officer Chief Medical Officer Chief Nursing Officer Emergency Management Coordinator Safety Director Security Chief Building Engineer Emergency Management Coordinator Radiation Safety Officer Employee Health Infection Control Risk Management Industrial Hygienist Infectious Disease Epidemiology Chief of Staff Chief of Pediatrics Nuclear Medicine Health Physicist Structural Engineer Outpatient Services Administrator Chief of Trauma Primary Care Director Behavior Health Director Legal Risk Manager Poison Control Director IT/IS Director Hospital Public Information Officer Marketing Director Patient Relations Chief Information Officer Community Relations Emergency Management Coordinator Strategic Planning VP of Administration Human Resources Director Nursing Director VP of Facilities Chief Procurement Officer Support Services Director Supply Director Facilities Director Warehouse Director Chief Finance Officer VP of Finance VP of Business Services Controller/Comptroller Hospital Administrator/ Admintrator on Call Chief Engineer

88
Building the IMT Positions appointed to meet the incident needs do not have to be sequential from the top down* Appoint those positions to meet the immediate needs of the incident Example……..

89
Building the IMT - Example
Situation: It is 4:00 am and a large fire erupts in the laboratory, located very close to two patient care areas with a high census. IC activates IMT positions needed immediately! I ensure safety of the patients, staff and facility I will oversee the medical care Example: In the case of a I ensure HVAC, Med Gases and assess damage I am needed to call in additional staff to assist with evacuation

90
IMT Communications Communication and information-sharing in the IMT should occur: Up and down the chain of command Across Sections to the appropriate Section/Branch/Unit** Information should be displayed on status boards and easily accessed Communications should be documented for accountability and archiving Communication can be formal and informal, people can talk among the branches sharing information.

91
Section Summary Incidents may be different but the IMT fundamentals remain the same: Positions activated and structure of IMT meet the needs of the incident Positions are filled by qualified and trained personnel Based on qualifications rather than by seniority The HICS IMT has a defined hierarchy and chain of command and reporting

92
Questions?

93
Command

94
Command Command functions Incident Commander in charge
Maintain overall management of the incident Set the incident objectives and priorities Devise and approve strategies Ensure mission completion Incident Commander in charge Command consists of: Command staff General staff

95
Command

96
Incident Commander Mission:
Organize and direct the Hospital Command Center (HCC). Give overall strategic direction for hospital incident management and support activities, response and recovery. Authorize total facility evacuation if warranted The first Incident Commander is responsible until the authority is delegated to another person**
. Give overall strategic direction for hospital incident management and support activities, response and recovery. Authorize total facility evacuation if warranted. The first Incident Commander is responsible until the authority is delegated to another person**")
97
Incident Commander Duties: Ensure incident safety *
Initiate HICS and activation of the HCC Determine scope and magnitude of event and potential impacts on the facility Determine and activate appropriate IMT positions Initiate and approve the IAP Providing information services to internal and external stakeholders* Liaison with Governing Board and other organizations*

98
Public Information Officer
Mission: Serve as the conduit for information to internal and external stakeholders**, including staff, visitors and families, and the news media, as approved by the Incident Commander Duties: Determine parameters of information release from the IC Determine any restrictions in content (sensitive materials) Collaborate with local community officials (JIC) on risk communication messages for consistent content Maintain contact with Situation Unit Leader for current information and facility status Schedule regular media briefings and press releases Report to: Incident Commander
 Collaborate with local community officials (JIC) on risk communication messages for consistent content. Maintain contact with Situation Unit Leader for current information and facility status. Schedule regular media briefings and press releases. Report to: Incident Commander.")
99
Safety Officer Mission: Duties: Report to: Incident Commander
Ensure safety of staff, patients, and visitors, monitor and correct hazardous conditions. Have authority to halt any operation that poses immediate threat to life and health Duties: Determine safety risks of the incident to personnel, the hospital facility, and the environment Initiate corrective/protective actions for safety issues Report to: Incident Commander

100
Liaison Officer Mission: Duties: Reports to: Incident Commander
Function as the incident contact person in the Hospital Command Center for representatives from other agencies Duties: Is the primary contact for supporting agencies and organizations assisting at an incident but not participating in the HCC/ICS structure** Establish contacts with liaison counterparts in each assisting and cooperating agency (including other hospitals, RHCCs, EOCs and others) Update governmental liaisons on the hospital status and response Make facility needs and requests for assistance and resources Reports to: Incident Commander
 Update governmental liaisons on the hospital status and response. Make facility needs and requests for assistance and resources. Reports to: Incident Commander.")
101
Medical/Technical Specialists
The Specialist Position is new and unique to HICS A category of personnel w/specialized expertise Activated based on situational need Primarily are consultants but can have delegated authority Can have more than one in activated at a time May report to any position in the IMT Hospitals can create other categories as needed

102
Medical/Technical Specialists
Specialist Roles Biological/Infectious disease Chemical Radiological Clinic Administration Hospital Administration Legal affairs Risk management Medical Staff Pediatric Care Medical Ethicist ** Others can be developed as needed by the hospital

103
Medical/Technical Specialists
Mission: Advise the Incident Commander and/or assigned Section on issues related to emergency response in their area of expertise Duties: May be assigned as technical advisor in the HCC May be assigned to advise and oversee specific hospital operations Example: Decontamination operations during a chemical exposure situation

104
Section Summary The Incident Commander is the only position that will ALWAYS be activated The Incident Commander has overall responsibility for: Management of the Incident Activities within the HCC Continuing as IC until authority is delegated to another The Command Staff consists of: PIO Liaison Safety Officer Medical/Technical Specialists

105
Questions?

106
Let’s talk about Sections

107
Sections Sections are: Sections are led by a Chief
Operations Planning Logistics Finance/Administration Sections are led by a Chief Section Chiefs are known as General Staff **

108
The Operations Section

109
Operations Section Section Mission: Lead by a Section Chief
Manage tactical operations** Direct all tactical resources Carry out the mission and Incident Action Plan Lead by a Section Chief Largest section of resources to marshal and coordinate Tactical resources are classified**: Assigned Available Out-of-Service

110
Operations Section The Section includes: Staging Area
Medical Care Branch Infrastructure Branch HazMat Branch Security Branch Business Continuity Branch

111
Operations Section Chief
Mission: Develop and implement strategy and tactics to carry out the objectives established by the Incident Commander. Organize, assign, and supervise Staging, Medical Care, Infrastructure, Security, Hazardous Materials, and Business Continuity Branch resources Duties: Appoint Section personnel as indicated by event Conduct Section briefings, update Unit Leaders Maintain current status of all areas in the Section Communicate with and advise the IC on Section issues/needs

112
Operations Section Chief
Supervises: Staging Manager Medical Care Branch Director Infrastructure Branch Director HazMat Branch Director Security Branch Director Business Continuity Branch Director

113
Staging Manager Mission: Supervises:
Organize and manage the deployment of supplementary resources, including personnel, vehicles, equipment, supplies, and medications Supervises: Personnel Staging Team Vehicle Staging Team Equipment/Supply Staging Team Medication Staging Team

114
Staging Manager Duties:
Coordinate delivery of needed resources to requesting area Once resources are acquired by Logistics, they are then staged with the Staging Manager Establish a staging area in a central location Area must be large enough to “stage” resources Works closely with the Logistics Section If staging area resources become too great, appoint appropriate Team Leaders

115
Medical Care Branch Director
Mission: Organize and manage the delivery of emergency, inpatient, outpatient, and casualty care, and clinical support services Duties: Addresses provision of acute AND continuous care Works closely with Logistics Section to ensure resource acquisition Works closely with Staging Manager for delivery of resources to areas

116
Medical Care Branch Director
Supervises: Inpatient Unit Leader (all inpatient units) Outpatient Unit Leader (all outpatient services) Casualty Care Unit Leader (Emergency Dept.) Mental Health Unit Leader Clinical Support Unit Leader (Lab, Diagnostic Imaging, Pharmacy, Morgue, Blood Donor) Patient Registration Unit Leader Reports to the Operations Section Chief
 Outpatient Unit Leader (all outpatient services) Casualty Care Unit Leader (Emergency Dept.) Mental Health Unit Leader. Clinical Support Unit Leader (Lab, Diagnostic Imaging, Pharmacy, Morgue, Blood Donor) Patient Registration Unit Leader. Reports to the Operations Section Chief.")
117
Infrastructure Branch Director
Mission: Organize and manage the services required to sustain and repair the hospital’s infrastructure operations Duties: Maintains overall facility operations and normal operating capacity Identify and fix utility service-delivery failures Coordinate the acquisition of parts or contractors with the Logistics Section Assign a strike team to address damage to the facility as needed

118
Infrastructure Branch Director
Supervises: Power/Lighting Unit Leader Water/Sewer Unit Leader HVAC Unit Leader Building/Grounds Unit Leader Medical Gases Unit Leader Medical Devices Unit Leader Environmental Services Unit Leader Food Services Unit Leader (for inpatients) Reports to Operations Section Chief
 Reports to Operations Section Chief.")
119
HazMat Branch Director
Mission: Organize and direct hazardous material incident response activities: detection and monitoring; spill response; victim, technical, and emergency decontamination; and facility and equipment decontamination Duties: Oversee the operations involving a hazmat event Decontamination of victims, staff, facility Safe and appropriate use of PPE Clean up operations Collaborates closely with Medical Care Branch Director

120
HazMat Branch Director
Supervises: Detection and Monitoring Unit Leader Spill Response Team Unit Leader Victim Decontamination Unit Leader Facility/Equipment Decontamination Unit Leader Reports to Operations Section Chief

121
Security Branch Director
Mission: Coordinate all of the activities related to internal and external personnel and facility security Duties: Implement facility security measures Ensure security and access control of the HCC Liaison with responding law enforcement personnel Oversee search and rescue operations for the facility

122
Security Branch Director
Supervises Access Control Unit Leader Crowd Control Unit Leader Traffic Control Unit Leader Search Unit Leader Law Enforcement Interface Unit Leader Reports to the Operations Section Chief

123
Business Continuity Branch Director
Mission: Ensure business functions are maintained, restored or augmented to meet designated Recovery Time Objectives (RTO) and provide limited interruptions to continuity of essential business operations Can be activated immediately or as needed during the response Duties: Facilitate the acquisition of and access to essential recovery resources, including business records Support Branches with relocation to alternate business sites Coordinate IT services with Logistics Section Assist Branches and impacted areas to restore normal operations Business continuity is an area that is greatly overlooked. Business recovery was once the arena only of the IT departments. However, the resumption on “normal” services and recovery of the facility is essential for community health and facility financial viability. It is very important that business continuity be addressed during the response phase and managed throughout recovery
 and provide limited interruptions to continuity of essential business operations. Can be activated immediately or as needed during the response. Duties: Facilitate the acquisition of and access to essential recovery resources, including business records. Support Branches with relocation to alternate business sites. Coordinate IT services with Logistics Section. Assist Branches and impacted areas to restore normal operations. Business continuity is an area that is greatly overlooked. Business recovery was once the arena only of the IT departments. However, the resumption on normal services and recovery of the facility is essential for community health and facility financial viability. It is very important that business continuity be addressed during the response phase and managed throughout recovery.")
124
Business Continuity Branch Director
Supervises: Information Technology Unit Leader Mission: Ensure IT business functions are maintained, restored or augmented Works closely with Logistics Section IT/IS Unit Service Continuity Unit Leader Mission: Ensure business/clinical/ancillary service functions are maintained, restored or augmented

125
Business Continuity Branch Director
Supervises: Records Preservation Unit Leader Mission: Ensure vital business/medical records are maintained and preserved Business Function Relocation Unit Leader Mission: Ensure business functions are moved to alternative work sites

126
Section Summary The Operations Section is responsible for
All tactical operations,** The tactical objectives and organization Directing all tactical resources Operations Section is led by a Chief Operations Section positions are activated as needed by the incident

127
Questions?

128
The Logistics Section

129
Logistics Provides support to other sections
Acquires resources from internal and external sources Activate existing MOUs, contracts and vendor agreements Employs standard and emergency procurement and contracting procedures With Liaison, links to local EOC and/or Regional Hospital Coordination Center for resource requests

130
Logistics and Operations
Logistics and Operations are closely linked and must work collaboratively together Logistics Section is the “getters” Operations Section is the “doers” Scope and Responsibilities overlap Logistics Supply Unit and Operations’ Infrastructure Branch Labor Pool and Credentialing Unit and Staging Manager– Personnel Team Leader These divisions might seem duplicative, but have been divided in the HICS IMT. Logistics is the “Radar O’Reilly” of the response, acquiring the resources needed to respond. The resources are then provided to the Operations Section to use. The examples of logistics and ops in this slide are to highlight the roles in each of the situations. #1: Scenario: the HVAC has failed. The Supply Unit and Facilities Units would work to get the needed items, or to contact the proper contractor to repair the HVAC. The Infrastructure Branch would oversee and participate in the actual repairs. #2: Scenario: Outbreak of infectious disease in the community with large number of victims over a prolonged period of time. Because of the size of the incident and the number of resources required, the Operations Section has activated their Staging Manager, including the Personnel Team Leader. The Labor Pool role will be to acquire the personnel, according to the needs of the departments and areas, and also credential volunteers. When the personnel arrives at the hospital, they would be sent to the Staging area to await assignment. In a scenario where the staging area is NOT activated, then the Labor Pool and Credentialing Unit would procure the personnel resources AND deploy those resources to the needed areas.

131
Logistics Section Chief
Mission: Organize and direct those operations associated with maintenance of the physical environment and with the provision of human resources, materiel, and services to support the incident activities. Participate in Incident Action Planning Duties: Oversee the acquisition of resources Maintain current status of all areas in the section

132
Logistics Section Chief
Supervises: Service Branch Director Support Branch Director Reports to the Incident Commander

133
Service Branch Director
Mission: Organize and manage the services required to maintain the hospital’s communication system, food and water supply for staff, and information technology and systems Oversees: Communications Unit Leader IT/IS Unit Leader Staff Food and Water Unit Leader

134
Service Branch Unit Leaders
Communications Unit Leader Mission: Organize and coordinate internal and external communications connectivity IT/IS Unit Leader Mission: Provide computer hardware, software and infrastructure support to staff Coordinates closely with Operations Section Business Continuity Branch, IT Unit Staff Food and Water Unit Leader Mission: Organize food and water stores and prepare for rationing during periods of anticipated or actual shortage Coordinates closely with Operations Section Infrastructure Branch, Food Services Unit

135
Support Branch Director
Mission: Organize and manage the services required to maintain the hospital’s supplies, facilities, transportation, and labor pool. Ensure the provision of logistical, psychological, and medical support of hospital staff and their dependents. Oversees: Employee Health and Well-Being Unit Leader Family Care Unit Leader Supply Unit Leader Facilities Unit Leader Transportation Unit Leader Labor Pool and Credentialing Unit Leader

136
Support Branch Unit Leaders
Employee Health and Well Being Unit (Known as the “Medical Unit” in ICS**) Mission: Provide medical screening, evaluation and follow-up of employees who are assigned to the incident** Ensure the availability of medical care for injured or ill staff Ensure the availability of behavioral and psychological support services to meet staff needs during and following an incident. Coordinate mass prophylaxis/vaccination/immunization of staff, if required. Coordinate medical surveillance program for employees Family Care Unit Ensure the availability of medical, logistic and mental health and day care for the families of staff members. Coordinate mass prophylaxis/vaccination/immunization of family members if required
 Mission: Provide medical screening, evaluation and follow-up of employees who are assigned to the incident** Ensure the availability of medical care for injured or ill staff. Ensure the availability of behavioral and psychological support services to meet staff needs during and following an incident. Coordinate mass prophylaxis/vaccination/immunization of staff, if required. Coordinate medical surveillance program for employees. Family Care Unit. Ensure the availability of medical, logistic and mental health and day care for the families of staff members. Coordinate mass prophylaxis/vaccination/immunization of family members if required.")
137
Support Branch Unit Leaders
Supply Unit Mission: Acquire, inventory, maintain, and provide medical and non-medical care equipment, supplies, and pharmaceuticals Facility Unit Organize, manage and support building systems, equipment and supplies. Ensure proper cleaning and disinfection of hospital environment.

138
Support Branch Unit Leaders
Transportation Unit Mission: Organize and coordinate the transportation of all ambulatory and non-ambulatory patients. Arrange for the transportation of human and materiel resources within or outside the facility Labor Pool and Credentialing Unit Collect and inventory available staff and volunteers at a central point (Labor Pool) for assignment by the Staging Officer. Maintain adequate numbers of both medical and non-medical personnel. Assist in the maintenance of staff morale Coordinates closely with Operations Section Staging Manager
 for assignment by the Staging Officer. Maintain adequate numbers of both medical and non-medical personnel. Assist in the maintenance of staff morale. Coordinates closely with Operations Section Staging Manager.")
139
Section Summary The Logistics Section supports the
resource requirements of the response Logistics Section has two branches: Support Service The Logistics Section is led by a Chief** Logistics works closely with the Operations Section

140
Questions?

141
Planning Section

142
Planning Section Section Mission: Lead by a Section Chief
Collect, evaluate, and disseminate incident action information and intelligence to Incident Commander* Prepare status report and display various information Develop the Incident Action Plan (IAP) Lead by a Section Chief
 Lead by a Section Chief.")
143
Planning Section Chief
Mission: Oversee all incident-related data gathering and analysis regarding incident operations and assigned resources, develop alternatives for tactical operations, conduct planning meetings, and prepare the Incident Action Plan (IAP) for each operational period Duties: Ensure distribution of critical information/data Compile scenario projections from all Section Chiefs and effect long range planning Document and distribute the facility action plan Conduct Section briefings, update Unit Leaders Maintain current status of all Sections
 for each operational period. Duties: Ensure distribution of critical information/data. Compile scenario projections from all Section Chiefs and effect long range planning. Document and distribute the facility action plan. Conduct Section briefings, update Unit Leaders. Maintain current status of all Sections.")
144
Planning Section Chief
Supervises: Resources Unit Leader Situation Unit Leader Documentation Unit Leader Demobilization Unit Leader

145
Resource Unit Leader Mission: Oversees:
Maintain information on the status, location, and availability of personnel, teams, facilities, supplies, and major equipment to ensure availability of use during the incident. Maintain a master list of all resources assigned to incident operations Oversees: Personnel Tracking Leader Materiel Tracking Leader

146
Tracking Leaders Personnel Tracking Leader Materiel Tracking Leader
Mission: Maintain information on the status, location, and availability of on-duty staff and volunteer personnel Materiel Tracking Leader Maintain information on the status, location, and availability of equipment and supplies within the hospital inventory and additional materiel received from outside agencies in support of the incident
![]()
147
Situation Unit Leader Mission:
Collect, process, and organize ongoing situation information; prepare situation summaries; and develop projections and forecasts of future events related to the incident. Prepare maps and gather and disseminate information and intelligence for use in the Incident Action Plan (IAP) Focus is on current and future situation management Writes and maintains situation updates and IAPs Maintains the HCC Status Boards This role and position is heavy clerical and paper focused, and must be staffed with adequate numbers of personnel to assist in performing functions.
 Focus is on current and future situation management. Writes and maintains situation updates and IAPs. Maintains the HCC Status Boards. This role and position is heavy clerical and paper focused, and must be staffed with adequate numbers of personnel to assist in performing functions.")
148
Situation Unit Leader The Situation Unit is very busy!
Staff with lots of clerical assistance Staff with people to monitor TV, media Networks closely with the Liaison Officer Supervises: Patient Tracking Leader Bed Tracking Leader

149
Tracking Leaders Patient Tracking Leader: Bed Tracking Leader:
Mission: Monitor and document the location of patients at all times within the hospital's patient care system, and track the destination of all patients departing the facility Bed Tracking Leader: Maintain information on the status, location, and availability of all patient beds, including disaster cots and stretchers
![]()
150
Documentation Unit Mission: Duties:
Maintain accurate and complete incident files, including a record of the hospital’s/HCC response and recovery actions and decisions; provide duplication services to incident personnel; and file, maintain, and store incident files for legal, analytical, and historical purposes Duties: Collects, organizes and archives all response and recovery documentation and paperwork (forms) Assists in writing the Incident Action Plan (IAP) Assists in preparing the After-Action Report and Corrective/Improvement Plan based on lessons learned** Works closely with the Situation Unit Leader
 Assists in writing the Incident Action Plan (IAP) Assists in preparing the After-Action Report and Corrective/Improvement Plan based on lessons learned** Works closely with the Situation Unit Leader.")
151
Demobilization Unit Mission: Duties:
Develop and coordinate an Incident Demobilization Plan that includes specific instructions for all staff and resources that will require demobilization Duties: Responsible for drafting demobilization and system/business recovery plan for the incident approved by the Command Staff/Incident Commander Demobilization starts EARLY in the response!

152
Section Summary The Planning Section is responsible for:
Collecting, evaluating and disseminating incident situation information and intelligence to the HCC Maintaining resource status Developing the Incident Action Plan (IAP) ** Archiving all response and recovery documentation Assisting with development of the After-Action Report The Planning Section is led by a Chief
 ** Archiving all response and recovery documentation. Assisting with development of the After-Action Report. The Planning Section is led by a Chief.")
153
Questions?

154
Finance/Administration Section

155
Finance/Administration Section
Section Mission: Account for costs incurred from the outset of the response Account for expenses from multiple cost centers Monitor, track and report personnel, time, repair, purchase, and replacement expenses and lost revenue Modify or expand daily (usual) accounting practices to meet the needs of the incident and outlined in the EOP Section led by a Chief
 accounting practices to meet the needs of the incident and outlined in the EOP. Section led by a Chief.")
156
Finance/Administration Section Chief
Mission: Monitor the utilization of financial assets and the accounting for financial expenditures. Supervise the documentation of expenditures and cost reimbursement activities Duties: Oversee the acquisition of supplies and services to carry out the medical mission Supervise the documentation of expenditures relevant to the emergency incident Directs financial RECOVERY

157
Finance/Administration Section Chief
Supervises: Time Unit Leader Procurement Unit Leader Compensation/Claims Unit Leader Cost Unit Leader

158
Time Unit Leader Mission:
Responsible for the documentation of personnel time records. Monitor and report on regular and overtime hours worked/volunteered Adjusts reports and tracking to meet the needs of the incident Tracking of altered or expanded work periods/shifts Developing specialized tracking forms to capture response and recovery time

159
Procurement Unit Leader
Mission: Responsible for administering accounts receivable and payable to contract and non-contract vendors Initiates emergency contracts Agreements should be already in place Confirm existing vendors can deliver in emergencies Confirm payment arrangements Manages purchase orders

160
Compensation/Claims Unit Leader
Mission: Responsible for receiving, investigating and documenting all claims reported to the hospital during the emergency incident, which are alleged to be the result of an accident or action on hospital property Duties: Manages claims and worker’s compensation issues Injury/illness to staff, volunteers and visitors Should have comprehensive line of duty death procedure to implement if needed Follow up coverage/compensation/benefits clearly outlined and shared with staff member Define what line of duty death is: a death of a staff or physician or volunteer member while on duty. Procedure should include information, grieving of staff and recognition of the dead person. Long term CISM may be necessary.

161
Cost Unit Leader Mission: Duties:
Responsible for providing cost analysis data for the declared emergency incident and maintenance of accurate records of incident cost Duties: Track and pay response and recovery costs Projects lost revenue Prepares documents for state/federal reimbursement when applicable Tracks payments Patient insurance and reimbursement Government

162
Section Summary The Finance/Administration Section**
Manages costs related to the incident Provides Accounting Procurement Time recording Cost analysis The Section is led by a Chief**

163
Questions?

164
Job Action Sheets

165
Purpose of the JAS An incident management tool to familiarize the user with critical aspects of the command position he or she is assuming. The series of action steps are intended to “prompt” the incident management team members to take needed actions related to their roles and responsibilities

166
Use of the JAS HICS provides 78 Job Action Sheets
In most cases only a portion of these positions will be necessary for a successful response Activation of HICS positions may be based on: Scope and magnitude of the event Hospital size Available resources Response needs

167
JAS Format The key format considerations for each JAS are the same and include the following information: Command Title – the name of the position Mission – a brief statement summarizing the basic purpose of the job Fundamental Information Box – Date and times Highlights reporting relationships Records to whom the position is assigned Location of the HCC or position Contact information and radio title

168
OPERATIONS SECTION CHIEF
JAS Format OPERATIONS SECTION CHIEF Mission: Develop and implement strategy and tactics to carry out the objectives established by the Incident Commander. Organize, assign, and supervise Staging, Medical Care, Infrastructure, Security, Hazardous Materials, and Business Continuity Branch resources. Date: Start: End: Position Assigned to: Initial: Position Reports to: Incident Commander Signature: Hospital Command Center (HCC) Location: Telephone: Fax: Other Contact Info: Radio Title:
 Location: Telephone: Fax: Other Contact Info: Radio Title:")
169
JAS Format Action Steps and Considerations
JAS provides position action steps and considerations Actions listed by operational periods Immediate –2 hours Intermediate –12 hours Extended Beyond 12 hours Demobilization/System Recovery (New)
")
170
JAS Format The JAS format enables users to:
Document each action undertaken with initials Record decision and action timeframes Many action steps are common to all positions Read the entire JAS Put on position identification Notify your usual supervisor of your HICS position Document using forms Coordinate with other HICS positions Include considerations for shift change report

171
Immediate Actions – Operations Chief
Immediate (Operational Period 0-2 Hours) Time Initial Receive appointment and briefing from the Incident Commander. Obtain packet containing Operations Section Job Action Sheets. Read this entire Job Action Sheet and review organization chart (HICS Form 207). Put on position identification. Notify your usual supervisor of your HICS assignment. Determine need to appoint Staging Manager, Branch Directors, and Unit Leaders in Operations Section; distribute corresponding Job Action Sheets and position identification. Complete the Branch Assignment List (HICS Form 204). Brief Operations Section Branch Directors and Staging Manager on current situation and incident objectives; develop response strategy and tactics; outline Section action plan and designate time for next briefing. Participate in Incident Action Plan preparation, briefings, and meetings as needed; assist in identifying strategies; determine tactics, work assignments, and resource requirements. Obtain information and updates regularly from Operations Section Branch Directors and Staging Manager; maintain current status of all areas; inform Situation Unit Leader of status information. In the JASs, there are actions and activities that are common to all ICS positions. An example of a few of the actions/duties that are common actions are listed in RED above.
 Time. Initial. Receive appointment and briefing from the Incident Commander. Obtain packet containing Operations Section Job Action Sheets. Read this entire Job Action Sheet and review organization chart (HICS Form 207). Put on position identification. Notify your usual supervisor of your HICS assignment. Determine need to appoint Staging Manager, Branch Directors, and Unit Leaders in Operations Section; distribute corresponding Job Action Sheets and position identification. Complete the Branch Assignment List (HICS Form 204). Brief Operations Section Branch Directors and Staging Manager on current situation and incident objectives; develop response strategy and tactics; outline Section action plan and designate time for next briefing. Participate in Incident Action Plan preparation, briefings, and meetings as needed; assist in identifying strategies; determine tactics, work assignments, and resource requirements. Obtain information and updates regularly from Operations Section Branch Directors and Staging Manager; maintain current status of all areas; inform Situation Unit Leader of status information. In the JASs, there are actions and activities that are common to all ICS positions. An example of a few of the actions/duties that are common actions are listed in RED above.")
172
Intermediate Actions – Operations Chief
Intermediate (Operational Period 2-12 Hours) Time Initial Communicate regularly with the Incident Commander, Public Information Officer and Liaison Officer; brief regularly on the status of the Operations Section. Designate time(s) for briefings and updates with Operations Section leadership to develop or update the Section action plan. Initiate the Resource Accounting Record (HICS Form 257) to track equipment used during the response. Schedule planning meetings with Branch Directors and Staging Manager to update the Section action plan and demobilization procedures. Coordinate patient care treatment standards and case definitions with public health officials, as appropriate. Ensure that the Operations Section is adequately staffed and supplied. Coordinate personnel needs with Labor Pool & Credentialing Unit Leader, supply and equipment needs with the Supply Unit Leader, projections and needs with the Planning Section, and financial matters with the Finance/Administration Section. Ensure coordination with any assisting or cooperating agency. Intermediate actions are listed as action items. The JAS also contain reminders or prompts for the user to complete position specific forms, as noted in red above. The JAS was also written to remind of other key positions that they should be coordinating with in the HCC… as listed in the second red area above.
 Time. Initial. Communicate regularly with the Incident Commander, Public Information Officer and Liaison Officer; brief regularly on the status of the Operations Section. Designate time(s) for briefings and updates with Operations Section leadership to develop or update the Section action plan. Initiate the Resource Accounting Record (HICS Form 257) to track equipment used during the response. Schedule planning meetings with Branch Directors and Staging Manager to update the Section action plan and demobilization procedures. Coordinate patient care treatment standards and case definitions with public health officials, as appropriate. Ensure that the Operations Section is adequately staffed and supplied. Coordinate personnel needs with Labor Pool & Credentialing Unit Leader, supply and equipment needs with the Supply Unit Leader, projections and needs with the Planning Section, and financial matters with the Finance/Administration Section. Ensure coordination with any assisting or cooperating agency. Intermediate actions are listed as action items. The JAS also contain reminders or prompts for the user to complete position specific forms, as noted in red above. The JAS was also written to remind of other key positions that they should be coordinating with in the HCC… as listed in the second red area above.")
173
Extended Actions – Operations Chief
Extended (Operational Period Beyond 12 Hours) Time Initial Continue to monitor Operations Section personnel’s ability to meet workload demands, staff health and safety, resource needs and documentation practices. Continue to maintain the Resource Accounting Record (HICS Form 257) to track equipment used during the response. Conduct regular situation briefings with Operations Section Branch Directors and Staging Manager. Address issues related to ongoing patient care: Ongoing patient arrival Bed availability Patient transfers Patient tracking Staff health and safety Mental health for patients, families, staff, incident management personnel Fatality management Staffing Staff prophylaxis Medications Medical equipment and supplies Personnel and resource movement through Staging Area Linkages with the medical community, area hospitals, and other healthcare facilities Documentation Upon shift change, brief your replacement on the status of all ongoing operations, issues, and other relevant incident information. The Extended actions will remind you to continue activities from the previous phases and prompt you to complete proper forms
 Time. Initial. Continue to monitor Operations Section personnel’s ability to meet workload demands, staff health and safety, resource needs and documentation practices. Continue to maintain the Resource Accounting Record (HICS Form 257) to track equipment used during the response. Conduct regular situation briefings with Operations Section Branch Directors and Staging Manager. Address issues related to ongoing patient care: Ongoing patient arrival. Bed availability. Patient transfers. Patient tracking. Staff health and safety. Mental health for patients, families, staff, incident management personnel. Fatality management. Staffing. Staff prophylaxis. Medications. Medical equipment and supplies. Personnel and resource movement through Staging Area. Linkages with the medical community, area hospitals, and other healthcare facilities. Documentation. Upon shift change, brief your replacement on the status of all ongoing operations, issues, and other relevant incident information. The Extended actions will remind you to continue activities from the previous phases and prompt you to complete proper forms.")
174
Demobilization/System Recovery Actions Operations Chief
Time Initial As needs decrease, return Operations Section staff to their usual jobs and combine or deactivate positions in a phased manner, in coordination with the Demobilization Unit Leader. Coordinate patient care restoration to normal services. Coordinate final reporting of patient information with external agencies through Liaison Officer and Public Information Officer. Work with Planning and Finance/Administration Sections to complete cost data information. Debrief staff on lessons learned and procedural/equipment changes needed. Upon deactivation of your position, brief the Incident Commander on current problems, outstanding issues, and follow-up requirements. Upon deactivation of your position, ensure all documentation and Operational Logs (HICS Form 214) are submitted to the Documentation Unit. Submit comments to the Incident Commander for discussion and possible inclusion in an after-action report; topics include: Review of pertinent position descriptions and operational checklists Recommendations for procedure changes Section accomplishments and issues Participate in stress management and after-action debriefings. Participate in other briefings and meetings as required. Demobilization/System Recovery is a new phase in HICS. Demob/Recovery can begin at any time during the response and should be considered very early in the response. The areas in blue are reminders to review the needs of your role/Section and demobilize people as needed. The JAS continues to remind you to coordinate with other sections. Upon deactivation of the position, reminds you of who to report to and submission of all documentation.
 are submitted to the Documentation Unit. Submit comments to the Incident Commander for discussion and possible inclusion in an after-action report; topics include: Review of pertinent position descriptions and operational checklists. Recommendations for procedure changes. Section accomplishments and issues. Participate in stress management and after-action debriefings. Participate in other briefings and meetings as required. Demobilization/System Recovery is a new phase in HICS. Demob/Recovery can begin at any time during the response and should be considered very early in the response. The areas in blue are reminders to review the needs of your role/Section and demobilize people as needed. The JAS continues to remind you to coordinate with other sections. Upon deactivation of the position, reminds you of who to report to and submission of all documentation.")
175
JAS Format Documents/Tools –
A listing of pertinent HICS forms this position is responsible for using Forms noted in JAS action steps Other tools that will help them fulfill their role and responsibilities Hospital plans, policies and procedures Technology tools Other adjuncts

176
Documents/Tools – Operations Chief
Incident Action Plan HICS Form 204 – Branch Assignment Sheet HICS Form 207 – Organization Chart HICS Form 213 – Incident Message Form HICS Form 214 – Operational Log HICS Form 257 – Resource Accounting Record Hospital emergency operations plan Hospital organization chart Hospital telephone directory Radio/satellite phone

177
Role of Deputies and Assistants
No JAS has been written for a Deputy Chief or assistants They work from the JAS of the position they assume Deputy Chief: Assigned for Command or General Staff Assistant: Assigned to Unit Leaders as needed and resources allow

178
JAS Use The format allows for the JASs to be used
To preliminarily document actions taken during the incident To develop a chronology of events, problems encountered, and decisions made Use the Operational Log (HICS Form 214) continuously to detail actions, decisions and activities
 continuously to detail actions, decisions and activities.")
179
JAS Use JASs are used continuously during the response
Actions in all operational periods should be continued and monitored JAS should transfer to your replacement and actions continued Upon shift change or position change

180
JAS Customization The JASs are designed to be customized for the needs of each hospital Hospitals can use the HICS JASs as prepared Hospitals can modify the HICS JASs based on: Hospital size Available resources Response needs Hospitals can craft their own, unique JAS

181
JAS Customization Hospitals are encouraged to use the HICS JAS model as a template for customized JASs Maintain the prescribed format and terminology to ensure the standardization benefit of NIMS Modify the Operational Period Actions and Documents/Tools section appropriately for the facility and community

182
JAS Customization Processes
Review all HICS Job Action Sheets Convene subject matter experts and stakeholders from within institution to review job action sheets Engage persons/staff who would fill those roles in an event Ensure JASs meet hospital needs Revise content as necessary with details (e.g. correct telephone numbers, etc) Place own hospital logo on each JAS if desired
 Place own hospital logo on each JAS if desired.")
183
JAS Training and Exercising
JASs should be used in trainings and exercising Enhance familiarity of position description, mission and actions Conduct focused drills with Branches and Sections to enhance understanding of the incident management team structure

184
Section Summary The Job Action Sheets are: An incident management tool
A series of actions to meet the incident response Are divided in time phases Immediate 0-2 hours Intermediate – 2-12 hours Extended – Greater than 12 hours Demobilization/System Recovery Standardized to facilitate interagency response Customizable for the unique facility needs/roles

185
Questions?

186
Incident Action Planning

187
Incident Action Plans Incidents Action Plans:
Provide all IMT personnel with direction for actions based on the objectives during the operational period** Are a means of communicating the overall incident objectives, including: Operational activities Support activities A tool to successful transition of operational activities to HCC relief staff Incident action planning requires an understanding the hospital’s policy and direction Incident action planning is essential for a successful response and recovery IAPlanning is not well done in hospitals. Please underscore the importance of Incident Action Planning and the planning process.

188
Incident Action Plans IAP processes use Management by Objectives
Setting the Operational Period Determining overall priorities Establishing specific, measurable, attainable objectives Selecting effective strategies and tactics to accomplish objectives Identify needed resources Develop and issue assignments Direct, monitor and evaluate response efforts to enhance response in the next op period Document results Corrective actions

189
Incident Action Planning
The IAP covers an Operational Period Elements of an IAP What must be done Who is responsible How information is communicated What should be done if someone is injured

190
Incident Action Planning Process
The Incident Commander sets times for IAP meetings The Section Chiefs develop their Section’s action plan for the next operational period Input from Branch and Unit staff Section IAP submitted to Planning Chief Assimilated into a single HCC IAP Documentation and Situation Unit Leaders compile the IAP

191
Incident Action Planning Process
Incident Action Planning Meeting conducted by the IC Command Staff and General Staff attend the meeting IAP is discussed and modified, as needed Next Action Planning Meeting is determined IC Approved and final IAP is distributed to HCC staff Distribution by the Documentation Unit Leader

192
Incident Action Planning
The IAP should be developed ASAP after the HCC is operational It becomes the preliminary guidance for a defined, short operational period HICS forms to utilize: HICS Form 201 – Incident Briefing HICS Form 202 – Incident Objectives** HICS Form 203 – Organizational Assignment List HICS Form 261 – Incident Action Plan Safety Analysis

193
Section Summary The IAP provides all IMT personnel with direction for actions based on the objectives during the operational period** Incident Action Planning uses the elements of Management by Objectives Incident Action Planning is done by Command and General Staff Incident Action Planning is essential for effective response and recovery

194
Questions?

195
Incident Planning Guides & Incident Response Guides

196
Incident Specific Planning
During the initial response period, activities are guided by: Emergency Operations Plan Incident-specific guides These plans/guides assist the IC: To conduct a situation assessment Set initial objectives Establish the HCC/ICS organization

197
HICS IPGs and IRGs An incident-specific scenario “sets the stage” for the IPGs and IRGs 13 internal scenarios Based on most likely internal hospital incidents 14 external scenarios Based on the Department of Homeland Security National Planning Scenarios

198
Incident Planning and Response Guides
Internal Guides Bomb Threat Evacuation Fire HazMat Spill Hospital Overload Hostage/Barricade Infant/child abduction Internal flooding Loss of HVAC Loss of Power Loss of Water Severe weather Work stoppage All-Hazards Guide External Guides Nuclear Detonation Biological attack - Anthrax Biological disease outbreak -Pandemic Influenza Biological Attack – Plague Chemical Attack – Blister Agent Chemical Attack – Toxic Industrial Chemicals Chemical Attack - Nerve agent Chemical Attack – Chlorine Natural Disaster – Earthquake Natural Disaster – Hurricane Radiological Attack – RDD Explosives Attack – IED Biological Attack – Food Contamination Cyber Attack There are only 14 external guides instead of the 15 in the National Planning Scenarios because number 14 is a veterinary problem of Foot and Mouth disease, that does not pose problem to hospital response and because the relative issues are addressed in the other external IPGs/IRGs

199
Introductory Scenario
Example: Internal Scenario - Fire Your hospital is in the middle of the annual flu season. It is mid winter and it is unusually cold outside. The time is 10:30 PM. The hospital inpatient beds are at 95% capacity and there are patients holding in the ED to be admitted. A fire has broken out and has engulfed the laboratory area, and the fire sprinkler system in that area has activated. The fire department quickly responds and extinguishes the fire before it can spread beyond the laboratory area. The fire department assists with the smoke and water removal. Two staff members from the laboratory are injured with burns and smoke inhalation, one seriously and one in critical condition. The lab is totally destroyed and is unusable. The extensive smoke and water damage has spread to the ICU and the patient rooms above the lab. The staff are asking if they should evacuate the hospital. The local press is now on scene and is demanding information and access to the hospital.

200
IPGs and IRGs Hospitals use these incident-specific guides
According to the facility HVA The community HVA Additional IRGs and IPGs may need to be developed by the facility to address a hazard

201
Incident Planning Guides

202
Incident Planning Guides
Outline strategic planning considerations for incident-specific situations Formatted to the emergency management phases Mitigation (including prevention) Preparedness Response Recovery Used to evaluate the facility’s Emergency Operations Plan Used to develop Incident Response Guides
 Preparedness. Response. Recovery. Used to evaluate the facility’s Emergency Operations Plan. Used to develop Incident Response Guides.")
203
IPG: Example - Fire Does your Emergency Management Plan Address the following issues? Mitigation & Preparedness Does the fire alarm and overhead announcement sound loudly enough to be heard in all locations? Does the fire alarm system include both audible and visual systems (e.g. alarm tone and flashing strobe lights)? Does the hospital have lighted emergency exits in all areas? Does the fire alarm automatically notify the local fire department? Does the hospital have a fire plan that includes closing and securing all doors and windows? Does the hospital have procedures to immediately shut off valves that control oxygen and other gases?
 Does the hospital have lighted emergency exits in all areas Does the fire alarm automatically notify the local fire department Does the hospital have a fire plan that includes closing and securing all doors and windows Does the hospital have procedures to immediately shut off valves that control oxygen and other gases")
204
Incident Response Guides

205
Incident Response Guides
Are incident-specific Are activated during response Provide critical considerations and actions for the Command and General Staff Are time based: Immediate – 0-2 hours Intermediate – 2-12 hours Extended – Greater than 12 hours Demobilization/System Recovery

206
Incident Response Guides
Should complement Emergency Operations Plan They complement the EOP but not replace the EOP Job Action Sheets Can be used as initial documentation

207
IRG – Example: Fire Directions
Mission: To reduce the loss of life and property during an internal fire incident. Directions □ Read this entire response guide and review incident management team chart Use this response guide as a checklist to ensure all tasks are addressed and completed Objectives Confine the fire/reduce the spread of the fire Rescue and protect patients and staff Implement internal emergency management plan – fire

208
IRG – Example: Fire Immediate Actions (Operational Period 0-2 Hours)
□ COMMAND (Incident Commander): -- Activate the facility emergency operations plan and the Incident Command structure -- Appoint Command Staff and Section Chiefs -- Consider the formation of a unified command with hospital and fire officials -- Determine need for and type of evacuation (PIO): -- Establish a media staging area -- Conduct regular media briefings to update situation status and provide appropriate patient and employee information -- Oversee patient family notifications of incident and evacuation/relocation, if ordered
: -- Activate the facility emergency operations plan and the Incident Command structure. -- Appoint Command Staff and Section Chiefs. -- Consider the formation of a unified command with hospital and fire officials. -- Determine need for and type of evacuation. (PIO): -- Establish a media staging area. -- Conduct regular media briefings to update situation status and provide appropriate patient and employee information. -- Oversee patient family notifications of incident and evacuation/relocation, if ordered.")
209
IRGs and IPGs Uses of the Guides
To evaluate the EOP A training tool Tabletop exercises As a planning basis for a functional exercise Guides will promote more immediate and higher quality decision-making

210
JAS versus IRGs & IPGs The IRGs are not intended to be a replacement for Job Action Sheets IRGs Overview position actions and decision making Are Incident Specific JASs Detail position actions, decisions and activities Are all-hazards focused

211
Section Summary IPGs and IRGs
Are incident-specific tools to assist hospitals with planning, training and response/recovery efforts Assist in meeting regulatory requirements Guide Command and General Staff with decision-making and action-taking Should be consistent with the EOP Do not replace the JAS

212
Questions?

213
HICS Forms

214
Using the HICS Forms Purpose: Use:
To provide the incident management team with the documents needed to manage a response Use: Each form has a specific purpose identified at the bottom of the form Instruction sheets for each form can be printed on reverse side of each form, if desired Forms have been modified from existing FEMA ICS forms for use in hospitals

215
Value of Using HICS Forms
Your facility will be consistent with other healthcare facilities and community responders Information can be more easily shared among all responders Documentation guides your response and assists in your recovery efforts

216
Value of Using HICS Forms
Serves as a road map in response: everyone acting from the same plan Serves as a foundation for corrective action Ensures consistency and compliance with regulatory guidelines Complies with NIMS Publications Management Standard*

217
Using the HICS Forms Forms format includes: 20 HICS forms
Form number Name of form Who is responsible for completion When form is to be completed 20 HICS forms Found in the Guidebook Appendix D Utilize current facility forms + HICS forms for response Develop additional forms to meet the incidents

218
Using HICS Forms Appropriate HICS forms completed by each HCC position
Forms can be done electronically or hand-written Write legibly and clearly Complete all areas on the form Completed forms distributed with a copy to the Planning Section Forms will be archived to document response Forms and other incident documentation used to craft the AAR

219
HICS Forms No. Name Responsible 201 Incident Briefing
Incident Commander 202 Incident Objectives Section Chiefs 203 Organizational Assignment List Resource Unit Leader 204 Branch Assignment List Branch Directors 205 Communications Log Communications Unit Leader 206 Staff Medical Plan Support Branch Director 207 Organization Chart 213 Incident Message Form All Positions 214 Operational Log Command Staff and General Staff 251 Facility System Status Report Infrastructure Branch Director The light blue areas are the forms used in the Incident Action Planning Process

220
No. Name Responsible 252 Section Personnel Time Sheet Section Chiefs
253 Volunteer Staff Registration Labor Pool & Credentailiting Unit Leader 254 Disaster Victim / Pt Tracking Form Patient Tracking Manager 255 Master Pt Evacuation Tracking Form 256 Procurement Summary Report Procurement Unit Leader 257 Resource Accounting Record 258 Hospital Resource Directory Resource Unit Leader 259 Hospital Casualty / Fatality Report 260 Patient Evacuation Tracking Form Inpt Unit Leader Outpt Unit Leader, Casualty Care Unit Leader 261 Incident Action Plan Safety Analysis Safety Officer

221
HICS 201 – Incident Briefing
Purpose Documents initial response information and actions taken at start-up Origination Incident Commander Copies to Command staff, Section Chiefs, and Documentation Unit Leader When to Complete Prior to briefing the current operational period Helpful Tips Distribute to all staff before initial briefing

222
HICS 201 – Incident Briefing
Instructions Print legibly and enter complete information Incident Name Date of briefing Time of Briefing Event History and Current Actions Taken Current Organization Notes (warnings, directives, etc.) Prepared by (name and position) Facility Name
 Prepared by (name and position) Facility Name.")
225
Lab/West Wing Fire 0800 Fire broke out at 7:00 am in the main laboratory on the 2nd floor. Large amount of smoke with foul odor. Fire sprinklers activated. 0705 HCC activated. EOP activated. Fire department enroute. Positions activated: Safety Officer, Operations Chief, Infrastructure Branch Director and Medical Care Branch Director 0800 Fire department arrived and unified command established. Evacuation of patient care areas near the lab in progress. All depts instructed to send casualty reports to HCC.

226
J. Smith B. Walters L. Henson A. Doe C. Barton N. DeGuzman R. O’Reilly A. Greenspan

227
HICS 202 – Incident Objectives
Purpose Defines objectives and issues for operational period Origination Planning Section Chief Copies to Command staff, General Staff and Documentation Unit Leader When to Complete Prior to briefing the current operational period Helpful Tips Serves as a roadmap to incident management

228
HICS 202 – Incident Objectives
Instructions Print legibly and enter complete information Incident Name Date prepared Time prepared Operational Period Date and Time General Command and Control Objectives for the Incident Weather / Environmental Implications for the Period General Safety / Safety Messages Attachments Prepared by (Planning Chief: use proper name) Approved by (Incident Commander) Facility Name
 Approved by (Incident Commander) Facility Name.")
230
Lab/West Wing Fire 0800 Ensure communications links to Fire Department, community hospitals and emergency operations center are functioning Initiate structural assessment of hospital Assess injuries to patients, visitors and staff 4. Establish alternate care sites as needed for patient evacuations Winds from NE at 12 mph. Low fog remains, expected to dissipate by Temperatures currently 41 degrees; high of 55 expected with overnight temps to high 30’s. Rain forecast by weekend.

231
HICS 203: Organization Assignment List
Lab/West Wing Fire 0900 J Smith Barbara Walters L. Henson Jane Doe Clara Barton

232
HICS 203: Organization Assignment List
Radar O’Reilly John Q. Public

233
HICS Form 204: Branch Assignment List

234
HICS Form 204: Branch Assignment List

235
HICS Form 213: Incident Message Form
C Barton, Operations R. O’Reilly, Logistics 1000 Call from the laboratory manager. States that the lab will not be functional due to major equipment damage from heat and smoke. Laboratory non-functional. Request transportation of stat lab specimens to the community laboratory for testing.

236
HICS Form 213: Incident Message Form
Community Laboratory called and will accept specimens and blood tubes for testing. Transporation van will pick up specimens and transport to the community lab at 1200. IMA Vampire 1100

237
HICS Form 214 Lab/West Wing Fire 2-27-07 2-27-07 0800-1500
Operations, Medical Care Branch 0820 Position Activated and situation briefing obtained 0900 West Unit patient care unit with major smoke damage. Patients with respiratory symptoms and anxiety. Ordered evacuation of the wing Clara Barton

238
HICS Form 254 Lab/West Wing Fire 2-27-07 2-27-07 0800-1500 1200
Transfer 1230 2135 Brad Pitt M 34 ED

239
HICS Form 255

240
HICS Form 257

241
HICS Form 258

242
HICS Form 258

243
HICS Form 258

244
HICS Form 261

245
Section Summary The HICS forms:
Provide the Incident Management Team with the documents needed to manage a response Assist in communication with external agencies and resources Assist in communication with hospital staff Provide documentation for response and recovery activities

246
Questions?

247
External Agency Coordination
Hospitals can no longer plan for emergencies in a silo Effective preparedness and response requires integration with other community responders Include local, regional and state responders Joint Commission requires community-wide planning and collaboration with responders

248
External Agency Coordination
Hospitals should be actively engaged in community planning and preparedness Public Safety Law enforcement/Medical Examiner or Coroner Fire EMS Public health Emergency Management (local agency) Behavioral/Mental Health Other public and private agencies
 Behavioral/Mental Health. Other public and private agencies.")
249
Community Planning Meetings with response partners serve to:
Increase understanding of response roles and limitations Develop regional response plans and procedures Plan, conduct and evaluate collaborative exercises Conduct multi-disciplinary training Build personal relationships across disciplines for better communication and response

250
Hospital Collaboration
Hospitals must also plan and prepare with other healthcare partners Within the corporate healthcare system Other community hospitals Clinics Long-term care facilities Regional Hospital Coordination Centers Regional Hospital Associations Within the integrated healthcare system: hospitals that are part of a corporate or not-for-profit integrated healthcare system must also coordinate their planning and response activities with the administrative sections of their parent organization. System hospitals may develop emergency planning committees to ensure consistent planning and response and plan collaborative exercises. Healthcare systems may also activate a system operations center during an incident to coordinate inter system hospital needs and information sharing.

251
Hospital Collaboration
Hospitals in a community should meet regularly Cooperative planning and training Conduct joint exercises Standardization between hospitals Terminology Use of HICS Mutual aid and scarce resource sharing Integrated plans and procedures Hospitals should strive to standardize emergency management practices in communities.

252
Hospital Collaboration
Develop and sign mutual aid agreements or MOUs How to request assistance from sister hospitals Sharing of resources Hospital resources Community resources Credentialing of staff/volunteers Initiation of patient transfers Standardizing purchases of equipment and supplies (cost savings and increased capacity)
")
253
Hospital Collaboration
Achieving the hospital collaboration points will meet four NIMS elements Element 1: Organizational adoption of NIMS Element 2: Utilization of ICS Element 3: Multi-agency coordination systems Element 17: Standardized and consistent terminology

254
Healthcare Provider Collaboration
Hospital collaboration with non-hospital facilities Clinics Urgent Care Centers and MD offices Long-term care facilities Include these providers in planning, training and exercises They can provide valuable resources Can augment healthcare capacity and preserve acute care hospitals for acute care

255
Hospital Command Center Activation
Once the HCC is activated Communication and information sharing with partners is vital Liaison Officer is the formal line of communications into and out from the facility But some positions also have communication and coordination lines with community providers and responders….

256
HICS Guidebook, Chapter 4, Page 21

257
HICS and Unified Command
Single agency command ** One agency involved in the response Hospitals using HICS are single agency command structures

258
HICS and Unified Command
Unified command is instituted ** When more than one responding agency is present or, The situation crosses political jurisdictions Leaders from the agency are co-located for collaborative decision making A unified IAP is developed Unified command may occur when hospitals are asked to respond to the incident scene

259
HICS and Unified Command
When does unified command apply to hospitals? When the hospital is the scene of the incident and other responders come to the facility Example: Hostage situation – Law Enforcement Hospital Fire – Fire Bomb threat –Bomb Squad/Law Enforcement Building collapse – Fire and Search & Rescue Water outage/rupture – Public Works

260
HICS and Unified Command
Unified command in the HCC A Unified Incident Management Team (UIMT) would be formed in the HCC Bomb Threat--- Hospital IC and Law Enforcement IC The UIMT facilitates Information sharing Individual agencies provide input into IAP Each agency retains individual authority over its assets and responsibilities Although there is equality, there still is a final authority In our example– who would that be?
 would be formed in the HCC. Bomb Threat--- Hospital IC and Law Enforcement IC. The UIMT facilitates. Information sharing. Individual agencies provide input into IAP. Each agency retains individual authority over its assets and responsibilities. Although there is equality, there still is a final authority. In our example– who would that be")
261
HICS and Area Command Area command is defined as:
A command structure to oversee the management of large or multiple incidents with individual ICS structures The area command structure Sets overall strategies and priorities Allocates critical resources Ensure incidents are properly managed Ensures overall objectives are achieved

262
HICS and Area Command Hospital example:
A large healthcare organization with multiple buildings on the facility grounds Main hospital Women’s hospital Multiple clinics A tornado occurs with scattered areas of activity and damage to multiple facilities All buildings activate their incident command structures/HCC The Main hospital serves as area command for all facilities, but each facility maintains an ICS structure

263
Section Summary Hospitals must plan collaboratively with community responders for effective emergency response and recovery Establishing and rehearsing pre-event MOUs or mutual aid agreements will ensure effective response Hospitals may utilize unified command and area command structures in certain situations

264
Questions?

265
HICS for Small and Rural Facilities

266
Rural and Small Hospital Challenges
Preparedness apathy: “It can’t happen here!” Relative isolation: Geography/distance may isolate the facility Remote distance from resources may delay assistance Limited resources and surge capacity: Fewer resources in the hospital and community Local government resources limited Limited reliable and redundant communications

267
Small and Rural Hospital Challenges
Limited healthcare personnel resources Overlapping community roles Healthcare providers serving on EMS units Reliance on community volunteers Limited funding Government grants based on population Population bases do not account for “seasonal” surge (i.e., vacation time, concerts, large events)
")
268
Small and Rural Hospital Challenges
Rural areas may be the destination for urban residents during an incident! Large numbers will quickly overwhelm resources National guidelines and recommendations Mostly focus on urban and suburban regions Do not account for variances in rural communities Yet, rural and small hospitals must meet all standards or recommendations!

269
Smaller and Rural Hospitals!
Using HICS in Smaller and Rural Hospitals! It Can Be Done!

270
The complete IMT is depicted
The complete IMT is depicted. How do we take 78 potential positions and scale it for small and rural facilities?

271
HICS for Smaller Facilities
Adapt HICS to your facility Consolidate positions Maintain the basic command structure The Medical/Technical Specialist role does not have to be maintained, but the basic command structure should be!

272
HICS for Smaller Facilities
Adapt HICS to your facility Combine the duties of like positions under the Branches Condense the JAS with critical duties for like positions listed Concentrate on the main Sections and Branches or critical Unit Leaders

273
Example Adapted IMT

274
HICS For Smaller Facilities
When adapting the IMT and consolidating positions, Create JASs for each position Include critical actions In mission statement In JAS elements Suggest having the full IMT JAS available If a large incident and help arrives Each position can then be activated

275
Section Summary The HICS IMT can be adapted for smaller and rural facilities JASs can be created for consolidated positions Maintaining mission statements and title Remember, you only activate positions as needed to meet the incident Keep all HICS JAS in the event positions need to be expanded

276
Questions?

277
Summary of the Day Today we have learned about:
NIMS and ICS concepts and principles NIMS Implementation Activities for Hospitals The origins of HICS The Hospital Incident Command System Incident Management Team Command and General Staff All HICS positions

278
Summary of the Day Today we learned about:
The importance of Incident Action Planning HICS Materials Job Action Sheets Incident Planning and Response Guides Forms Relationship of the Hospital to Community Responders HICS for Rural and Small Hospitals

279
Evaluation of the Day How was the course so far????

280
Thank You! See you tomorrow!

Similar presentations
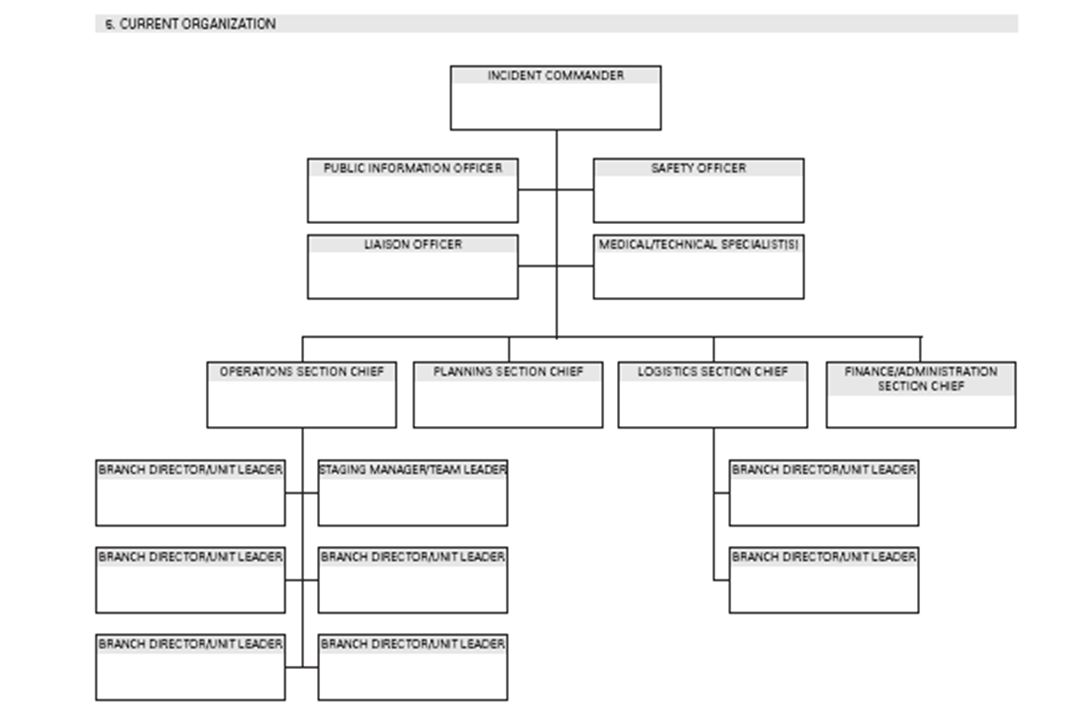

















 2006 Implementation.>")


