Download presentation
Presentation is loading. Please wait.

1
Tumor Markers

2
Tumor Tumor refers to the uncontrolled growth of cells that can develop into a solid mass and spread to other areas of the body Although it is often specified as a single disorder, cancer is a broad term used to describe more than 200 different diseases that affect more than 50 tissues It is important to understand that not all tumors are cancerous. There are benign tumors where the growth is limited to certain part of the body. A tumor becomes cancer when it is malignant.

3
Tumor The formation (tumorigenesis) and spreading (metastasis) of tumors are caused by a complex combination of inherited and acquired genetic mutations During tumorigenesis, these mutations include: activation of growth factors (e.g., epidermal growth factor [EGF]) and oncogenes (e.g., K-ras), in combination with inhibition of apoptosis, tumor suppressor, and cell cycle regulation genes (e.g., BRCA1, p53, cyclins) As cancer progresses toward metastasis, additional genetic changes are required such as: loss of cell adhesion proteins (e.g., Beta-catenin and E-cadherin) and activation of angiogenesis genes (e.g., VEGF)
 and spreading (metastasis) of tumors are caused by a complex combination of inherited and acquired genetic mutations. During tumorigenesis, these mutations include: activation of growth factors (e.g., epidermal growth factor [EGF]) and oncogenes (e.g., K-ras), in combination with inhibition of apoptosis, tumor suppressor, and cell cycle regulation genes (e.g., BRCA1, p53, cyclins) As cancer progresses toward metastasis, additional genetic changes are required such as: loss of cell adhesion proteins (e.g., Beta-catenin and E-cadherin) and activation of angiogenesis genes (e.g., VEGF)")
4
Stages of Tumor Cancer severity is generally classified by a combination of several factors. Depending on the type of cancer, these factors include tumor size, histology, regional lymph node involvement, and presence of metastasis. For most solid tumors (e.g., breast, lung, kidney), cancer is broadly classified (using roman numerals I–IV) into four stages
, cancer is broadly classified (using roman numerals I–IV) into four stages.")
6
Tumor Markers A Tumor marker is a biological substance synthesized and released by: The tumor or by the host in response to tumor tissue It may be used to: Detect the presence of a tumor Monitor the progress of disease Monitor the response to treatment

7
Tumor Antigens Tumor specific antigens Tumor associated antigens
Direct product of oncogenesis Disorganization of the genetic information leading to synthesis of antigens that are unique to the specific tumor cell Tumor associated antigens Most antigens are not specific for individual tumors but rather are usually associated with different tumors derived from the same or closely related tissue E.g. Oncofetal antigens: Antigens present in normal fetal growth and stimulated by malignancies later in life

8
How to identify tumor marker ?
On cell Immunocytochemistry, Flow cytometry On tissue Immunohistochemistry In body fluids Blood, urine, CSF, Amniotic fluid RIA, EIA

9
Tumor markers in Cancer Management
Screening Diagnosis Staging & Prognosis Therapy Monitoring Detecting recurrence

10
Tumor markers in Cancer Management

11
Screening Tumor markers play a limited role for tumor screening, because relatively low sensitivity lack of specificity Inappropriate for the detection of small in situ cancer However, successful cancer screening has been carried out by measuring tumor markers Eg. PSA → prostate cancer Carcinoma in situ is, by definition, a localized phenomenon, with no potential for metastasis unless it progresses into cancer.

12
Screening Susceptibility to cancer can be determined using molecular diagnostics in patients with breast, ovarian, or colon cancer Screening for susceptibility to breast and ovarian cancers is done by: identifying germline BRCA1 and BRCA2 mutations. Similarly, familial colon cancers can be identified by: the presence of the adenomatous polyposis coli gene (APC)
")
13
Diagnosis Tumor marker is not the key diagnostic examination, but can be a complementary sign to clinical finding or medical imaging AFP → hepatoma

14
Staging & Prognosis The major clinical value of tumor markers is in tumor staging, monitoring therapeutic response and detecting recurrence The tumor markers and medical imaging are complementary in the pre-therapeutic and post-therapeutic staging

15
Staging & Prognosis Serum concentration of tumor markers increases with tumor progression and usually reaches the highest levels when tumors become metastasized. The serum levels of tumor markers at diagnosis are likely to reflect the aggressiveness of the tumor and help predict the outcome for the patients. High levels indicate the presence of a malignant or metastatic tumor → poor prognosis.

16
Monitoring and Disease Recurrence
One of the most useful applications of tumor markers is monitoring therapy efficacy and detecting disease recurrence. After surgical resection, radiation, or drug therapy of cancer (chemotherapy), tumor markers are routinely followed. In patients with elevated tumor markers at diagnosis, effective therapy results in a dramatic decrease or disappearance of the tumor marker.
, tumor markers are routinely followed. In patients with elevated tumor markers at diagnosis, effective therapy results in a dramatic decrease or disappearance of the tumor marker.")
17
Monitoring and Disease Recurrence
If the initial treatment is effective, the appearance of circulating tumor markers can then be used as a highly sensitive marker of recurrence Many markers have a significant lead time of several months before disease would be detected by other methods, allowing treatment of an earlier-stage cancer.

18
Ideal Tumor Marker Characteristics
Sensitive & Specific Presence of a given marker identifies an exact malignancy Concentration proportional to tumor size Concentration changes with growth or reduction of malignancy Concentration is low after remission Concentration is a good indicator of prognosis Short half-life (concentration reflects current conditions)
")
19
Reality of tumor markers
Unfortunately, most tumor markers only possess some of the ideal characteristics (never all of them) Most tumor markers are not very sensitive and are poor screening tests for the detection of malignancies Most tumor markers are best utilized to confirm or monitor already diagnosed cancers ability to correctly identify people who have the disease
 Most tumor markers are not very sensitive and are poor screening tests for the detection of malignancies. Most tumor markers are best utilized to confirm or monitor already diagnosed cancers. ability to correctly identify people who have the disease.")
20
Different Types of Tumor Markers
Fetal antigens Proteins Hormones Enzymes Steroid Receptors

21
Oncofetal antigens Oncofetal antigens expressed transiently during normal fetal development and are then turned on again in the formation tumors

22
CEA (Carcinoembryonic Antigen )
Oncofetal antigen Best tumor marker for monitoring of colon cancer Also elevated in Smokers, Alcoholic cirrhosis & Ulcerative colitis Good correlation with treatment and prognosis of colon cancer ↓ CEA after surgical removal of tumor ↑ CEA if malignancy re-occurs or metastasizes Levels correlate well with chemotherapy and irradiation treatment Assay: ELISA and RIA

23
Alpha –FetoProtein (AFP)
Oncofetal antigen ↑ in pregnancy and certain malignancies Useful tumor marker for monitoring Liver cancer, hepatocellular carcinomas (HCC) Gonadal malignancies Serial measurements of AFP used to monitor treatment and post-surgery in patients with HCC. Assay: ELISA and RIA
 Gonadal malignancies. Serial measurements of AFP used to monitor treatment and post-surgery in patients with HCC. Assay: ELISA and RIA.")
24
Prostate Specific Antigen (PSA)
PSA is a tissue specific protein secreted by malignant prostate cells PSA is present in low concentrations of normal males, but elevated in malignancies and other conditions Good screening test for the detection of prostate cancer in older males and the monitoring of previously diagnosed tumors Complete removal of prostate should result in an undetectable total PSA in serum, any measurable tPSA would indicate residual prostatic tissue or metastasis. Assay: Immunoassays (ELISA) Total (t) PSA = free (f) PSA + complex (c) PSA
 Total (t) PSA = free (f) PSA + complex (c) PSA.")
25
CA 125 CA 125 is a protein that is associated with normal ductal tissue Utilized to evaluate gonadal ovarian cancers CA125 is not efficient in detecting early (more treatable) ovarian cancers CA125 is useful in detecting late ovarian cancers and recurrence of cancers False positives may occur, resulting in unnecessary treatment 75 % of ovarian cancers are not diagnosed until late in the disease. Assay: ELISA , RIA
 ovarian cancers. CA125 is useful in detecting late ovarian cancers and recurrence of cancers. False positives may occur, resulting in unnecessary treatment 75 % of ovarian cancers are not diagnosed until late in the disease. Assay: ELISA , RIA.")
26
Paraproteins Any of the incomplete monoclonal immunoglobulins that occur in plasma cell disorders Paraproteins are detectable in either serum or urine in 98-99% of patients with Multiple Myeloma. Their detection is valuable in the diagnosis of this condition Paraprotein concentrations correlate well with Tumor bulk Reduction in the amount of paraprotein is a good indicator of the efficacy of treatment.

27
Hormones as tumor markers
hCG is a hormone produced by the normal placenta (pregnancy) The presence of hCG in the plasma at other times indicates the presence of abnormal trophoblastic tissue tumors of the ovary and testis. The outermost layer of cells of the mammalian blastocyst that attaches the fertilized ovum to the uterine wall and serves as a nutritive pathway for the embryo. It is a prognostic indicator for ovarian cancer, a diagnostic marker for classification of testicular cancer Assay: ELISA Human Chorionic Gonadotropin
 The presence of hCG in the plasma at other times indicates the presence of abnormal trophoblastic tissue tumors of the ovary and testis. The outermost layer of cells of the mammalian blastocyst that attaches the fertilized ovum to the uterine wall and serves as a nutritive pathway for the embryo. It is a prognostic indicator for. ovarian cancer, a diagnostic marker. for classification of testicular cancer. Assay: ELISA. Human Chorionic Gonadotropin.")
28
Enzymes as Tumor Markers
Plasma enzyme activities are often increased in patients with cancer, usually a secondary effect of the tumor rather than a result of secretion of an enzyme by the tumor. Examples include the increase in alkaline phosphatase activity seen in patients with bone cancer. Increase in the plasma activity of the placental type in plasma occurs in many patients with lung, ovarian & others Measurement of placental alkaline phosphatase is of value in monitoring the response of such patients to treatment.

29
Steroid Receptors Hormonally dependent organs (breast) give rise to malignancies that may in themselves be hormonally dependent Eliminating hormonal stimulation by drugs leads to a regression of the respective malignancy Predicting which tumor respond to hormonal manipulation can be achieved by measuring steroid hormone receptors on tumors

30
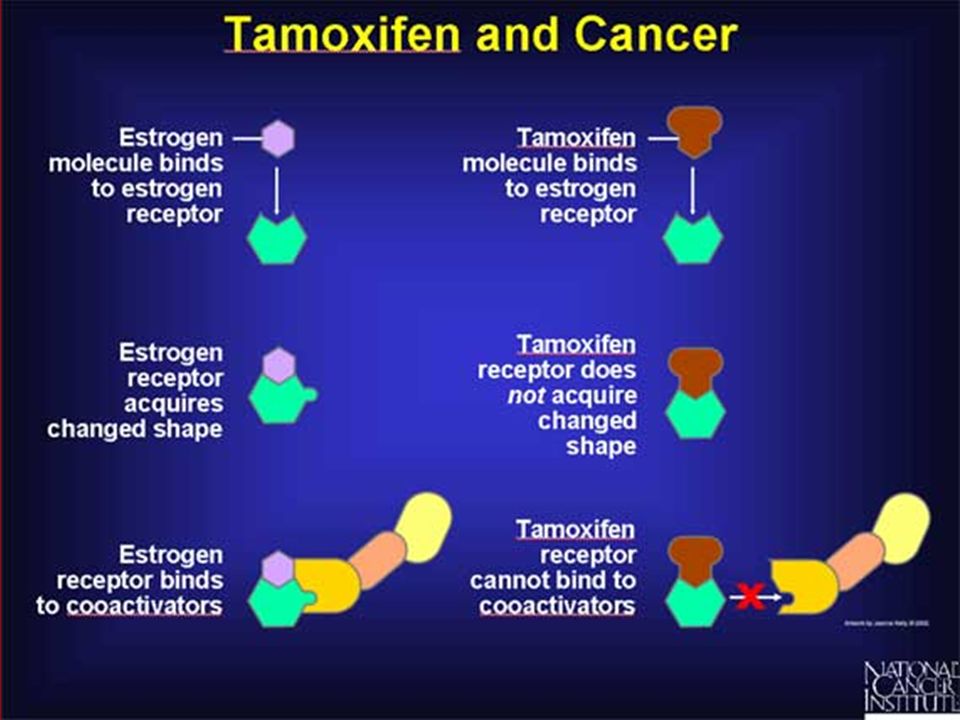
Estrogen & Progesterone Receptors
It is a protein localized in the nuclei of mammary and uterine tissue. Patients whose primary tumors demonstrated ER will respond to hormone therapy. ER and progesterone receptor assays are used to predict the therapeutic response of breast cancer patients to hormonal treatment

Similar presentations