Download presentation
Presentation is loading. Please wait.

1
PRACTICAL TRANSPLANT IMMUNOLOGY
Dr Nisar Anwar FRCP(Edin),Accredited Renal Physician (UK) Professor & Head : Department Of Nephrology KTH, Peshawar
,Accredited Renal Physician (UK) Professor & Head : Department Of Nephrology. KTH, Peshawar.")
2
TERMINOLOGY OF TRANSPLANTATION
Auto graft (e.g. skin grafts for burns, etc.) Syngraft (genetically identical twins; some stem cell therapies: nuclear transfer, iPS approaches) – No immunologic rejection for these two types
Allograft (genetically distinct member of same species; almost all medical transplants) Xenograft (different species; attractive due to shortage of organs for transplants) – Very severe rejection problems.
 Syngraft (genetically identical twins; some stem cell therapies: nuclear transfer, iPS approaches) – No immunologic rejection for these two types Allograft (genetically distinct member of same species; almost all medical transplants) Xenograft (different species; attractive due to shortage of organs for transplants) – Very severe rejection problems.")
3
IMMUNOLOGY OF TRANSPLANTATION
Major barrier to organ/tissue transplantation is immunological Immune system recognizes transplant as foreign and destroys it Memory and specificity have properties of adaptive immune response Memory is transferred by T cells (antibodies also can contribute).
.")
4
HISTOCOMPATIBILITY ANTIGENS
ABO blood group antigens
Pre-existing antibodies to A or B antigens lead to “hyperacute rejection” if not matched properly Major histocompatibility antigens Encoded by the MHC, originally discovered for their role in skin graft rejection in mice Minor histocompatibility antigens Allelic variants of normal cellular proteins.

5
Transplantation antigens
Major Histocompatibility Complex (MHC): Class I antigens: constitutively expressed on surface of most cells Class II antigens: expressed on cells of lymphoid system Expression of MHC molecules can be up regulated by ischemia, etc. nomenclature HLA (human) class I: A, B, C; class II: DR, DQ H-2 (mouse) class I: K, D, L; class II: IA, IE 5
: Class I antigens: constitutively expressed on surface of most cells. Class II antigens: expressed on cells of lymphoid system. Expression of MHC molecules can be up regulated by ischemia, etc. nomenclature. HLA (human) class I: A, B, C; class II: DR, DQ. H-2 (mouse) class I: K, D, L; class II: IA, IE. 5.")
6
MHC NOMENCLATURE Identified & characterized over 40 years ago
Antigens were identified using antisera obtained from multiparous women, new antisera can split HLA antigens in to narrower specificities DNA based techniques are more accurate in describing alleles Frequency of antigens, alleles and combinations vary considerably Most common HLA antigen A2 is found in 50% of the population.

7
MHC STRUCTURE

9
MHC CHARACTERISTICS Polymorphism Genes are co-dominantly expressed
Each MHC locus can express any one of hundreds of different molecules Set of different MHC molecules or alleles expressed on one chromosome is called a Haplotype A Genotype is the sum of two haplotypes Genes are co-dominantly expressed An individual expresses alleles from both chromosomes at each locus

10
INHERITANCE Each parental chromosome 6 provides a haplotype or linked set of MHC genes to the offspring. Haplotypes are usually inherited intact from each parent The child carries one representative antigen from each of class I & class II loci of each parent A child is a one haplotype match to each parent HLA haplotypes are inherited in a mendelian fashion 25% siblings will share two haplotype match, 50% will share one haplotype and 25% will have zero match

11
HLA-sensitization Exposure to non-self HLA antigens can cause production of HLA-directed antibodies Common causes of HLA-sensitization include blood transfusions, pregnancies, previous transplants In infants, tissue patches implanted during cardiac surgery cause sensitization 11

12
Does MHC (HLA) ‘Matching’ Prevent Rejection?
Reduces rejection but there are still ‘minor histocompatibility antigens’ (MiHA) MiHA are probably polymorphisms affecting peptides in the grooves But we cannot MHC-match most grafts: too much polymorphism, too little time, too few donors Therefore need immunosuppression 12
 MiHA are probably polymorphisms affecting peptides in the grooves. But we cannot MHC-match most grafts: too much polymorphism, too little time, too few donors. Therefore need immunosuppression. 12.")
14
Matching and Cross-Matching
Matching: finding a donor who shares the HLA antigens of the recipient, to minimize antigen disparities requires donor and recipient antigens to be identified Cross-matching: testing the SERUM of the recipient for antibodies against the donor antigens 14

15
Identifying MHC Polymorphisms (‘tissue typing’)
Formerly determined by antibodies against MHC molecules HLA typing MLR Now by DNA testing: allele-specific PCR, sequencing 15

16
Tissue Typing(or HLA-typing)
Used to identify HLA molecules on cells Ab against HLA1 + complement Recipient Donor Cells die, appear blue

17
MIXED LYMPHOCYTE REACTION:
Recipient Donor + (Irradiate) Cell Proliferation Strong Proliferation--->High incompatibility Weak proliferation--->Low incompatibility No proliferation---> 100% compatibility Helps to identify any antigenic differences between donor and recipient
 Cell Proliferation. Strong Proliferation--->High incompatibility. Weak proliferation--->Low incompatibility. No proliferation---> 100% compatibility. Helps to identify any antigenic differences between donor and recipient.")
19
CD4 & CD8 Subsets Of T Cells
CD 4 or Helper subset of T cells directly bind MHC class II molecules CD 8 or Cytolytic subset of T cells directly bind MHC class I molecules CD 4 cells mediate initial recognition of an allograft CD 4 deficient mice are unable to reject grafts while CD 8 deficient mice do reject grafts.

20
TCR SPECIFICITY AND SELF-MHC
MHC molecules are highly polymorphic During development in the thymus, T cells are selected
for moderate/weak binding to self-MHC + a self-peptide (“positive selection”) During development in the thymus, T cells are killed (or become regulatory T cells) if they have strong binding to self-MHC + a self-peptide (“negative selection”) Do the T cells of one person “see” MHC molecules from another person?
Actually about 1% of T cells bind such MHC with self peptide strongly--like a microbial antigen/MHC complex-- and become activated (“alloreactive T cells”)
 During development in the thymus, T cells are killed (or become regulatory T cells) if they have strong binding to self-MHC + a self-peptide ( negative selection ) Do the T cells of one person see MHC molecules from another person Actually about 1% of T cells bind such MHC with self peptide strongly--like a microbial antigen/MHC complex-- and become activated ( alloreactive T cells )")
22
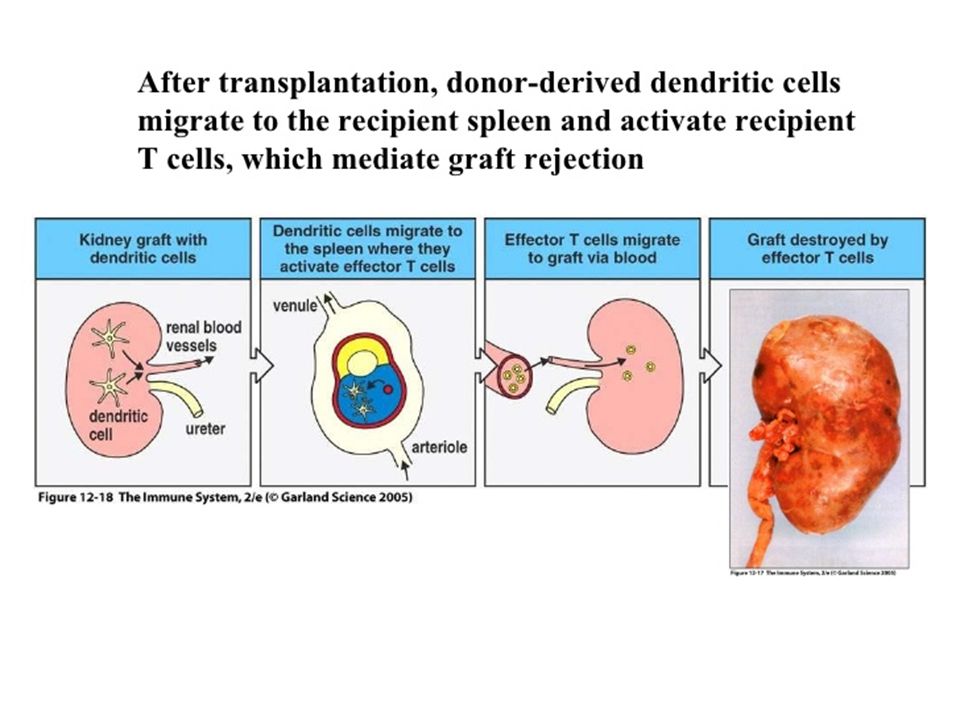
DIRECT PRESENTATION Direct presentation in transplantation (MHC + peptide: MHC is from graft; peptides are from cellular proteins, graft and/or host) Graft dendritic cell is induced to mature, express co-stimulatory molecules (B7) and migrate to lymph node by stress of surgery, etc. DC in lymph node activates allo-MHC recognizing CD4+ T cells and CD8+ T cells Activated T cells expand and then home to sites of inflammation where they find allo-MHC on graft cells and secrete cytokines/kill graft cells This is the critical pathway for CD8 T cell response.
 and migrate to lymph node by stress of surgery, etc. DC in lymph node activates allo-MHC recognizing CD4+ T cells and CD8+ T cells. Activated T cells expand and then home to sites of inflammation where they find allo-MHC on graft cells and secrete cytokines/kill graft cells. This is the critical pathway for CD8 T cell response.")
23
DIRECT PRESENTATION IN GRAFT REJECTION
Blue: host cell; pink: graft cell see also Abbas et al. Fig

24
Semi-direct Antigen Presentation the Membrane Patch Pathway
Host CD8+ cytotoxic cell Host CD8+ T cell Allogeneic Donor Cell Class I Shed membrane with donor MHC Intact donor MHC Host APC 24

25
INDIRECT PRESENTATION
Indirect presentation in transplantation (MHC + peptide: MHC is from host, peptide may be from graft MHC) Dendritic cell pick up antigens (e.g. allo-MHCs), and load peptides from these allo-MHC onto their own MHC II, migrate to lymph nodes and activate T cells CD4+ T cells are activated and then migrate to sites of inflammation where they are activated by host macrophages or DCs presenting graft antigens, leads to inflammatory reaction and tissue damage. The indirect pathway is probably responsible for chronic rejection (rejection after 1 year)
 Dendritic cell pick up antigens (e.g. allo-MHCs), and load peptides from these allo-MHC onto their own MHC II, migrate to lymph nodes and activate T cells. CD4+ T cells are activated and then migrate to sites of inflammation where they are activated by host macrophages or DCs presenting graft antigens, leads to inflammatory reaction and tissue damage. The indirect pathway is probably responsible for chronic rejection (rejection after 1 year)")
26
INDIRECT PRESENTATION IN GRAFT REJECTION

27
Allorecognition: Indirect Pathways
CD8+ cytotoxic cell CD4+ T cell IL-2 Class I Shed Allogeneic MHC (donor class I-derived peptide presented by host class II molecules) Allogeneic Donor Cell Donor MHC molecules are taken up and processed by host antigen presenting cell Host antigen presenting cell 27
 Allogeneic. Donor Cell. Donor MHC molecules are. taken up and. processed by host. antigen presenting cell. Host antigen presenting cell. 27.")
28
3 Signals for T Cell Responses
APC Ag signal 2 costimulation B7 CD28 cytokines IL etc signal 1 IL-2 signal 3 T cell activation G S M G2 replication key genes e.g.IL-2, CD40L Expression of effector activity 28

29
Three-Signal Model Halloran, N Eng J Med, 2004;351:3715

30
ROLE OF CO-STIMULATORY PATHWAY
Do Alloreactive T cells need co stimulation? Ordinarily T cell immune responses require co-stimulation (B7/CD28) Blocking co stimulation with CTLA4-Ig, “belatacept” protects against acute graft rejection in kidney patients (phase III clinical trials published in 2010; FDA approval in 2011) Most likely explanation:
-ischemia, stress to organ, release of DAMPs can induce expression of co-stimulators
-may explain why live donor organs have superior outcomes for kidney transplants compared to cadaver donor organs.
 Blocking co stimulation with CTLA4-Ig, belatacept protects against acute graft rejection in kidney patients (phase III clinical trials published in 2010; FDA approval in 2011) Most likely explanation: -ischemia, stress to organ, release of DAMPs can induce expression of co-stimulators -may explain why live donor organs have superior outcomes for kidney transplants compared to cadaver donor organs.")
31
CNIs Halloran, N Eng J Med, 2004;351:3715

32
CALCINEURIN PATHWAY

33
MECHANISM OF IMMUNOSUPPRESSION BY CYCLOSPORINE
NF-AT: nuclear factor of activated T cells NF-AT is required for transcription of the IL-2 gene and some other cytokine genes NF-AT cannot be activated in presence of cyclosporine.

34
Corticosteroids Corticosteroids Halloran, N Eng J Med, 2004;351:3715

37
Mycophenolates Halloran, N Eng J Med, 2004;351:3715

38
m-TOR inhibitors Halloran, N Eng J Med, 2004;351:3715

40
ROLE OF B LYMPHOCYTES Key role in hyper acute rejection.
B cells are less important than T cells in initiating an allo response but antibody formation can play a role in the effecter phase of graft destruction and chronic rejection.

41
LEUKOCYTE RECRUITMENT

42
Transplantation Antigens
ABO system ABH antigens are complex carbohydrate (polysaccharide) structures on surface of many cell types including graft cells & RBC; genes encode production of specific glycosyltransferases catalyze addition of terminal trisaccharide nomenclature H antigen: base chain; defines blood type O A trisaccharide on H chain: blood type A or A1 B trisaccharide on H chain: blood type B A and B trisaccharides on H chains: blood type AB 42
 structures on surface of many cell types including graft cells & RBC; genes encode production of specific glycosyltransferases catalyze addition of terminal trisaccharide. nomenclature. H antigen: base chain; defines blood type O. A trisaccharide on H chain: blood type A or A1. B trisaccharide on H chain: blood type B. A and B trisaccharides on H chains: blood type AB. 42.")
43
The ABO Blood Group Barrier in Organ Transplantation
‘ABO’ antigens: carbohydrate structures expressed on many tissues and organs, including endothelium of organ transplants Recipient pre-formed ‘natural’ anti-A or anti-B antibodies to non-self A/B antigens Transplantation of ABO-incompatible organs: ‘Hyperacute’ rejection 43

44
© 2007 New Science Press Ltd new-science-press.com
‘isohemagglutinins’ Figure The ABO blood cell antigen system Top: schematic representation of the carbohydrate structures corresponding to the A, B and H antigens. The H antigen is modified by the addition of a single sugar residue by the allelic glycosyltransferase enzymes that create the A and B antigens. The H antigen is present on the surface of A, B, AB and O individuals, as indicated in the lower panel, because not all H antigens are modified by the A or B glycosyltransferase. The H antigen is only recognized by antibodies made in rare individuals who lack enzymes that make this oligosaccharide structure, which is present on glycolipids and glycoproteins of red blood cells and some other cell types including endothelial cells. Also shown in the lower panel is the antibody to the A and B antigens present in individuals of different blood types. ABO compatibility between donor and recipient is crucial to avoid rapid graft rejection © 2007 New Science Press Ltd new-science-press.com 44

46
ABO Incompatible Renal Transplantation
Plasmapharesis IVIG CMV-IVIG Splenectomy Pre Transplant Immunosuppression

47
TYPES OF TRANSPLANT GRAFT REJECTION
Antibody-mediated rejection (AMR) Hyperacute rejection Acute or delayed AMR Cellular rejection ‘Chronic’ rejection 47
 Hyperacute rejection. Acute or delayed AMR. Cellular rejection. ‘Chronic’ rejection. 47.")
Similar presentations










>")



 from one part or individual to another (Merriam-Webster) May take place between different.>")






 Features of immune.>")






