Download presentation
Presentation is loading. Please wait.

1
Valvular Heart Disease
Asymptomatic 62 y/o male Long-standing heart murmur 2/6 SEM at base of heart PMI and carotid upstroke normal S2 splits normally ECG, CXR normal

2
Valvular Heart Disease
What would you do at this time? Refer to cardiologist Order an echocardiogram Follow without further testing until symptoms develop

3
Is the Murmur Significant?
Is the patient symptomatic? Are symptoms consistent with cardiac limitation? Is there chamber or cardiac enlargement on CXR or examination? Is there LVH or RVH on present ECG?

4
Clues from the Circulatory System
Jugular venous pulse Carotid upstroke: brisk, delayed or weak? Peripheral pulses and pulse pressure Apical impulse: displaced, sustained or normal? Right ventricular lift Thrill Heart rate and rhythm

5
Innocent Cardiac Murmurs
Midsystolic (never diastolic) A2 heard clearly Crescendo-decrescendo Variable intensity (grade 1-2/6) Does not radiate widely
 A2 heard clearly. Crescendo-decrescendo. Variable intensity (grade 1-2/6) Does not radiate widely.")
6
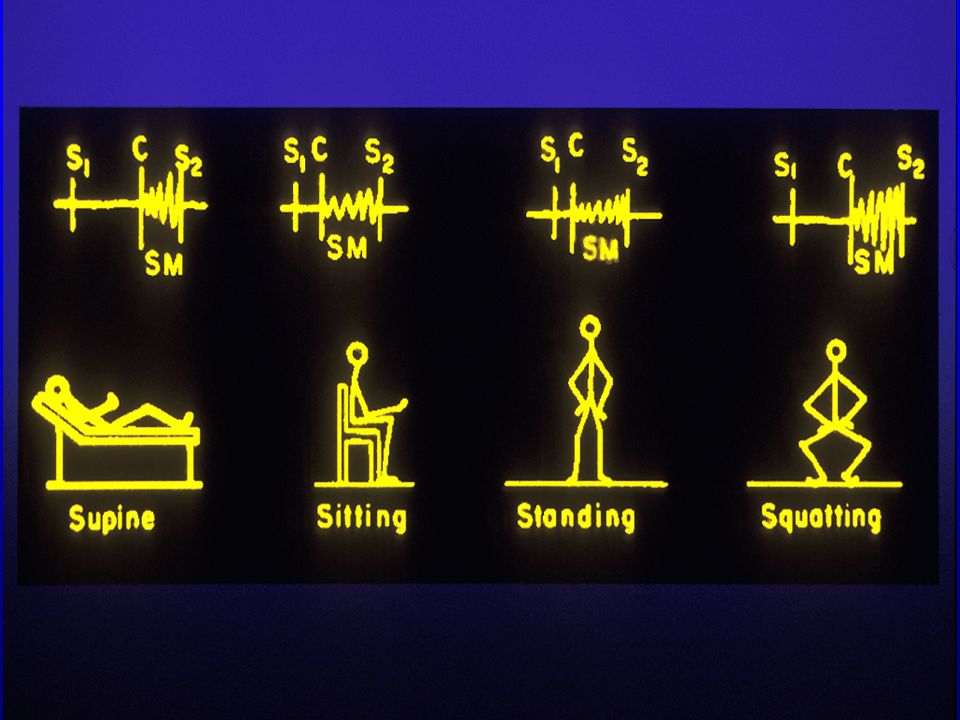
Useful Maneurvers Valsalva: decreased venous return during Phase 2
Squat-Stand: Decreased venous return like Valsalva Sustained Hand Grip: increased SVR, increased cardiac output, increased BP

7
The Second Heart Sound Normal: Single S2 in expiration
Wide: Right bundle branch block, RV pacing Fixed: ASD/common atrium Paradoxic: Left bundle branch block

8
Bedside Diagnosis of Pulmonary Hypertension
P2 > A2 with P2 heard at LV apex Secondary findings of tricuspid insufficiency, elevated CVP, pedal edema Appropriate clinical situation: known CHF, severe lung disease, loud heart murmur, cardiac arrhythmia

9
Most Common Misdiagnosed Systolic Murmurs
Mild Aortic Stenosis Mild Pulmonic Stenosis Atrial Septal Defect Mitral Valve Prolapse Hypertrophic Cardiomyopathy Question: Who warrants SBE prophylaxis?

10
SBE Prophylaxis-2007 Guidelines
Prosthetic cardiac valve Previous infectious endocarditis Complex congenital heart disease Cardiac transplantation recipients who develop cardiac valvulopathy

12
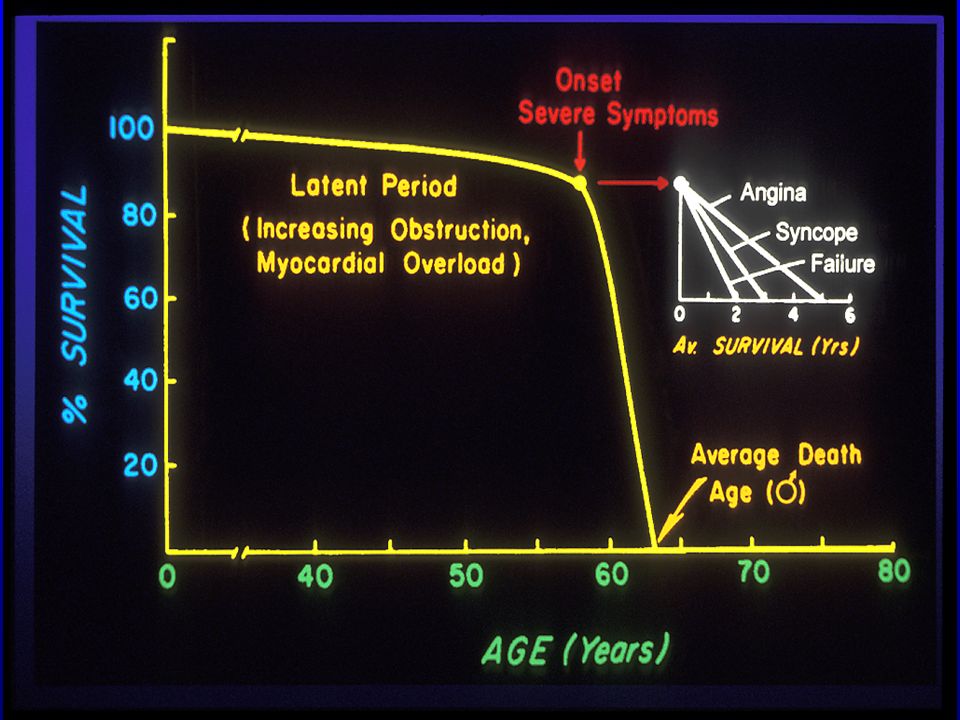
Valvular Heart Disease Mild to Moderate Aortic Stenosis
Yearly history and physical examination Focus on symptoms of angina, CHF, near syncope Echocardiogram q 3-5 years (peak velocity < 3 M/sec)
")
13
Valvular Heart Disease:Moderate to Severe Aortic Stenosis
Annual history and physical examination Angina, CHF or near syncope? Echocardiogram yearly Peak velocity > 3 M/sec

14
Pulmonic Stenosis Congenital lesion with systolic ejection click
Systolic ejection murmur at left upper sternal border Infraclavicular radiation Right ventricular lift

16
Atrial Septal Defects Primum ASD: Associated with cleft mitral valve and marked LAD on ECG Secundum ASD: Most common with female predominance Sinus venosus ASD: Associated with partial anomalous venous return All have wide/fixed split of S2

17
MVP: A Syndrome with Too Many Names
Myxomatous mitral valve prolapse Click/murmur syndrome Floppy mitral valve syndrome “Classic” MVP Barlow’s Syndrome

19
History of Mitral Valve Prolapse
Barlow describes MVP syndrome VPC’s and sudden cardiac death Prevalance 5-15%??? High risk markers for MVP complications identified Saddle shaped mitral annulus described

20
MVP: Clinical Exam Non-ejection click Mid-to-late systolic click
Pansystolic murmur Mid-to-late systolic murmur Precordial “Honk” Changes with maneuvers “Silent” MVP

22
Complications of MVP Syndrome
Ruptured chorda tendiniae Progressive mitral insufficiency Subacute bacterial endocarditis Sudden cardiac death Transient ischemic attacks

23
Complications in Classic and Nonclassic Mitral Valve Prolapse
Classic (N=319) Nonclassic (N=137) P Value SBE 3.5% (11) <0.02 Severe MR 11.9% (30) <0.001 MV surgery 6.6% (21) 0.7% (1) TIA/stroke 7.5% (24) 5.8% (8) ns
 Nonclassic (N=137) P Value. SBE. 3.5% (11) <0.02. Severe MR. 11.9% (30) < MV surgery. 6.6% (21) 0.7% (1) TIA/stroke. 7.5% (24) 5.8% (8) ns.")
24
Hypertrophic Cardiomyopathy
May occur with or without dynamic LVOT obstruction Systolic ejection murmur at lower left sternal border Murmur increases during Phase 2 of Valsalva Bisferiens pulse

25
Hypertrophic Cardiomyopathy Treatment: General Guidelines
Physical Activity: Avoid strenuous activity (no competitive sports), avoid dehydration Endocarditis Risk: Dental care Genetic Counseling: Screen first degree relatives, pregnancy counseling
, avoid dehydration. Endocarditis Risk: Dental care. Genetic Counseling: Screen first degree relatives, pregnancy counseling.")
26
Hypertrophic Cardiomyopathy: Treatment
General guidelines Medical therapy: Beta blockers, Ca channel blockers Catheter based septal ablation Surgical myectomy AICD implantation

27
HCM: ECG from 1995

28
HCM: ECG from 2002

29
HCM: ECG from January 2010

30
Is the Murmur Significant?
Is the patient symptomatic? Are symptoms consistent with cardiac limitation? Is there cardiac enlargement or chamber enlargement on CXR or exam? Is there LVH or RVH on ECG?

Similar presentations