Download presentation
Presentation is loading. Please wait.

1
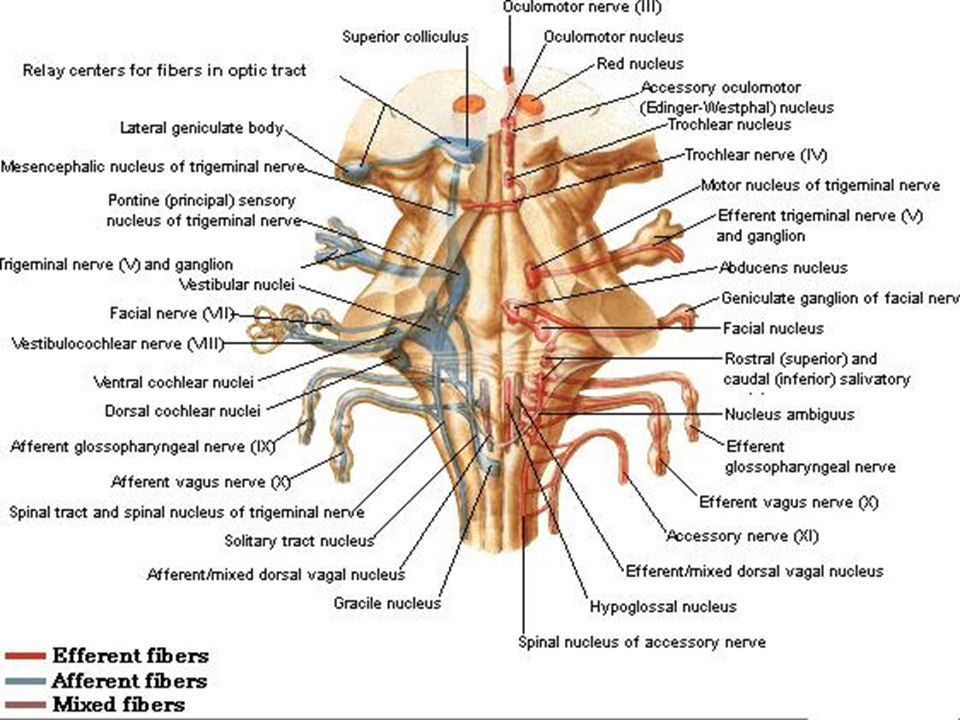
Brain stem Anterior view

2
Pons

3
Pons The pons may be divided into ventral or basal portion and a dorsal portion, also known as tegmentum The ventral portion is marked by numerous transversely oriented fascicles of pontocerebellar fibres that originate from scattered cell groups called pontine nuclei

6
Pons The pontocerebellar fibres pass to the contra- lateral side of the cerebellum through the massive middle cerebellar peduncle Corticospinal fibres appear as small and separate bundles running longitudinally between the fascicles of transverse pontine fibres

7
Pons The ascending fibres of the medial lemniscus become separated from the pyramid and displaced dorsally together with the spinal lemniscus and trigeminothalamic tract, by intervening transverse pontocerebellar fibres

10
Pons The medial lemniscus also rotates through 90º so that it lies almost horizontally, marking the boundary between ventral and tegmental portions of pons

11
Pons In the caudal pons, an additional group of transversely running fibres is located ventral to the ascending lemniscal fibres but dorsal to the pontocerebellar fibres This is the trapezoid body which consists of acoustic fibres crossing the brain stem from the cochlear nuclei

13
Pons They ascend into the midbrain as the lateral lemniscus and terminate in the inferior colliculus Beneath the floor of the fourth ventricle, in the pontine tegmentum lie a number of cranial nerve nuclei

14
Pons These nuclei include: Abducens nucleus for lateral rectus muscle
Facial motor nucleus for muscles of facial expression Trigeminal motor nucleus for muscles of mastication

17
Pons Each nucleus supply to their respective cranial nerves
Trigeminal sensory nucleus encountered in the medulla It reaches its maximum extent in the pons, adjacent to the origin of the trigeminal nerve

19
Section of Pons at the level of Facial colliculus

20
Section of pons at the level of trigeminal nuclei

21
Vestibular nuclei And Connections

22
Cochlear nuclei And Connections

23
Pontine syndromes Medial pontine Syndrome
Structures Associated CST Medial lemniscus 6th nerve fibers 7th nerve fibres Sign Contralateral spastic hemiparesis of the body Contralateral loss of position and vibration of the body Medial strabismus Raymond's Syndrome Alternating abducent hemiplegia Miller-gubler syndrome Alternating Facial hemiplegia.

24
Lateral pontine syndrome
Structure ICP Spinal 5 Spinothalamic Fibers of 7 Fibers of 8 Sign Ipsilateral limb ataxia Ipsilateral pain and temp loss - Face Contralateral pain and temp-Body Horner’s syndrome (Ipsilateral) Hearing loss Ipsilateral facial paralysis
 Hearing loss. Ipsilateral facial paralysis.")
25
Clinical Case A 50-year-old man with hypertension, congestive heart failure, and polysubstance abuse (cocaine, cigarettes, alcohol, and marijuana) experienced three days of acute onset of horizontal diplopia, left mouth drooling, and left-sided weakness. On examination he had right abducens nerve palsy, left-sided central paresis of the lower part of the face and limbs, and left hyperreflexia. Pupils were equal, round, and reactive to light and accommodation. He did not exhibit ptosis. There was no muscle tenderness. Sensation was normal and intact. Cerebellar coordination exam was normal on the right but limited on the left due to weakness.
 experienced three days of acute onset of horizontal diplopia, left mouth drooling, and left-sided weakness. On examination he had right abducens nerve palsy, left-sided central paresis of the lower part of the face and limbs, and left hyperreflexia. Pupils were equal, round, and reactive to light and accommodation. He did not exhibit ptosis. There was no muscle tenderness. Sensation was normal and intact. Cerebellar coordination exam was normal on the right but limited on the left due to weakness.")
26
Case . A 41-year-old woman presents to her physician with "double vision" and is unable to adduct her right eye on attempted left lateral gaze. Convergence is intact. Both direct and consensual light reflexes are normal. Which of the following structures is most likely to be affected? Left oculomotor nerve Medial longitudinal fasciculus Right abducens nerve Right oculomotor nerve Right trochlear nerve

27
Vestibulo Ocular Reflex

28
Internuclear ophthalmoplegia
Lesion involving left MLF Normal left gaze Defective left adduction and ataxic nystagmus of right eye Convergence intact if lesion discrete Demylination - usually bilateral Vascular disease Tumours of brainstem

29
Case 2. A patient with a bullet wound to the head is referred to you for neurological examination. Upon entering the hospital room you find the patient on a respiratory and cardiac monitor. You have difficulty arousing the patient and once awake you note the following: Right pupil is constricted; there is medial strabismus of the right eye and upon attempted right lateral gaze the left eye fails to adduct; loss of pain and temperature sensitivity on the right side of the face and left side of the body; deafness of the right ear; a pronounced intention tremor in the right arm and leg. The deep tendon reflexes on the right side are not as brisk as those on the left and there appears to be a complete facial paralysis on the right side. The likely site for this lesion is: The left internal capsule The right caudal pons The left cerebellar hemisphere The left side of the midbrain at the level of the superior colliculus The right side of the medulla at the level of the dorsal column nuclei

Similar presentations










.>")



>")
 Is it a stroke? (2) What part of the brain is affected? (3) What caused this stroke? Is it a haemorrhage or an infarct? Can.>")
>")


 contains three components: fiber bundles of the corticospinal tracts, pontine nuclei.>")






