Download presentation
Presentation is loading. Please wait.

1
PAEDIATRIC ORTHOPAEDICS

2
ORTHO - PAEDICS

3
Children are not small Adults

4
Anatomic differences Centers of ossification Radiolucent growth plate Thicker and stronger periosteum

5
Biomechanic differences Osteoid of a child’s bone is not significantly less calcified,but the density of a young’s bone is certainly less Pores prevent the extension of a fracture line Porous nature allows failure in compression Growth remodeling based in asymmetric growth of physis and periosteum

6
Clinical examination-The grate Art Children never lie Children cry Listen to the mother Congenital deformities Family history Abused child

7
Congenital deformities Infantile hip Dysplasia or Congenital dislocation of the Hip Coxa Vara-Coxa Valga Paediatric Foot

8
C.D.H-Incidence 1-6\1000 births Left hip is affected about twice as frequently as the right Highest risk for first born girls Family history Scoliosis[10 times grater incidence]
![C.D.H-Incidence 1-6\1000 births Left hip is affected about twice as frequently as the right Highest risk for first born girls Family history Scoliosis[10 times grater incidence]](http://images.slideplayer.com/26/8384891/slides/slide_8.jpg "C.D.H-Incidence 1-6\1000 births Left hip is affected about twice as frequently as the right Highest risk for first born girls Family history Scoliosis[10 times grater incidence]")
9
Etiology Familiar tendency Joint laxity Acetabular dysplasia Mechanical factors Deficiency in growth of the labrum[limbus] Hormonal abnormalities
![Etiology Familiar tendency Joint laxity Acetabular dysplasia Mechanical factors Deficiency in growth of the labrum[limbus] Hormonal abnormalities](http://images.slideplayer.com/26/8384891/slides/slide_9.jpg "Etiology Familiar tendency Joint laxity Acetabular dysplasia Mechanical factors Deficiency in growth of the labrum[limbus] Hormonal abnormalities")
10
Physical Assessment Apparent limb’s shortening Ortolani’s test Barlow’s test Limited abduction[no more than half way] Assymetrical skin creases Perineal gap Late walking,waddling gait
![Physical Assessment Apparent limb’s shortening Ortolani’s test Barlow’s test Limited abduction[no more than half way] Assymetrical skin creases Perineal gap Late walking,waddling gait](http://images.slideplayer.com/26/8384891/slides/slide_10.jpg "Physical Assessment Apparent limb’s shortening Ortolani’s test Barlow’s test Limited abduction[no more than half way] Assymetrical skin creases Perineal gap Late walking,waddling gait")
11
Radiologic assessment Xrays Ultrasonography Computed tomography Magnetic Resonance Imaging

13
Treatment Closed treatment:Pavlik harness,Von Rosen harness,Frejka pillow Surgical procedures:Salter acetabular osteotomy,Chiari acetabular osteotomy,femoral osteotomies

14
Slipped Capital Femoral Epiphysis

15
Incidence Boys age 12 to14, girls age 10 to 12 Caucasian children 1 to 3 per 100.000 Black males,higher incidence[7 to 8 per 100.000]
![Incidence Boys age 12 to14, girls age 10 to 12 Caucasian children 1 to 3 per Black males,higher incidence[7 to 8 per ]](http://images.slideplayer.com/26/8384891/slides/slide_15.jpg "Incidence Boys age 12 to14, girls age 10 to 12 Caucasian children 1 to 3 per Black males,higher incidence[7 to 8 per ]")
16
Etiologic factors Obesity Rapid growth spurts Endocrinopathies[hypothyroidism,renal rickets,hypogonadism] Mechanical factors
![Etiologic factors Obesity Rapid growth spurts Endocrinopathies[hypothyroidism,renal rickets,hypogonadism] Mechanical factors](http://images.slideplayer.com/26/8384891/slides/slide_16.jpg "Etiologic factors Obesity Rapid growth spurts Endocrinopathies[hypothyroidism,renal rickets,hypogonadism] Mechanical factors")
17
Clinical Presentation Preslip Acute slip Chronic slip[3 weeks] Acute on chronic slip
![Clinical Presentation Preslip Acute slip Chronic slip[3 weeks] Acute on chronic slip](http://images.slideplayer.com/26/8384891/slides/slide_17.jpg "Clinical Presentation Preslip Acute slip Chronic slip[3 weeks] Acute on chronic slip")
18
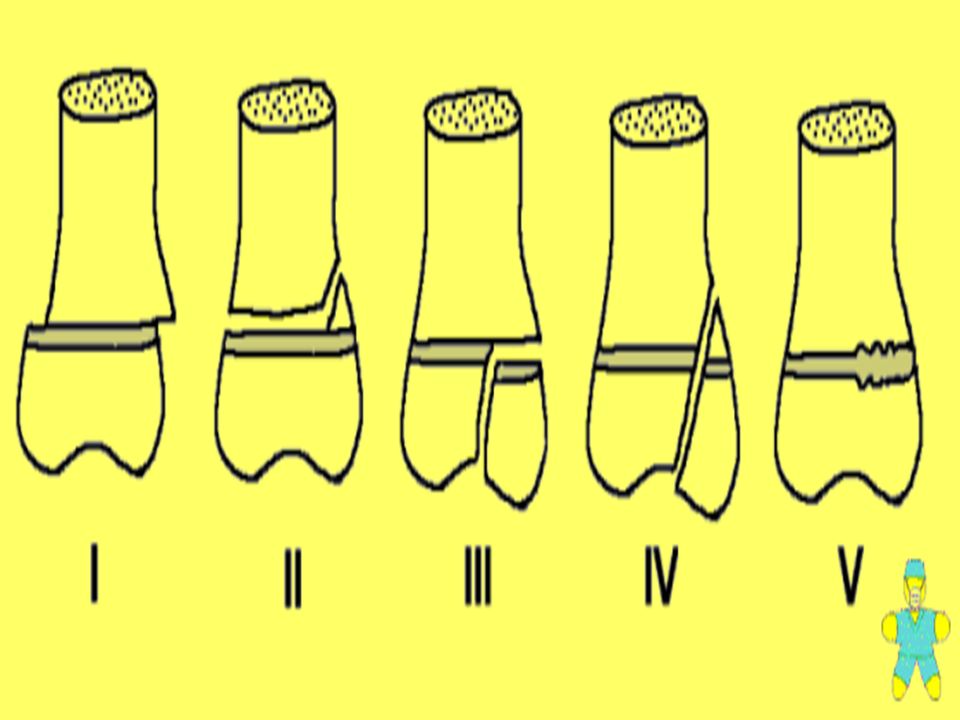
Diagnostic Imaging Lateral Head-shaft Angle[Southwick’ method] >60, 30-60,30> Klein’s line Epiphyseal height Physeal widening One third uncovered metaphysis,grade 1 Two thirds,grade 2 More than two thirds,grade 3
![Diagnostic Imaging Lateral Head-shaft Angle[Southwick’ method] >60, 30-60,30> Klein’s line Epiphyseal height Physeal widening One third uncovered metaphysis,grade 1 Two thirds,grade 2 More than two thirds,grade 3](http://images.slideplayer.com/26/8384891/slides/slide_18.jpg "Diagnostic Imaging Lateral Head-shaft Angle[Southwick’ method] >60, 30-60,30> Klein’s line Epiphyseal height Physeal widening One third uncovered metaphysis,grade 1 Two thirds,grade 2 More than two thirds,grade 3")
20
Treatment Manipulation Pinning Osteotomies

21
Legg-Calve-Perthes’ Deasease

22
Incidence 1 in 10.000 Particularly rare in black children Usually 4-8 years old Boys are affected 4 times as often as girls Higher incidence in underprivileged communities

23
Pathogenesis Blood supply of femoral head:1/metaphyseal vessels which penetrate the growth disc 2/lateral epiphyseal vessels running in the retinacula 3/scanty vessels in the ligamentum teres Between 4 and 7 years of age blood supply and venous drainage depends almost entirely on the lateral epiphyseal vessels

24
Pathology Stage 1: Ischaemia and bone death Stage 2:Revascularizasion and repair Stage 3: Distorsion and remodeling

28
Treatment Analgesia-? Skin traction Supervised neglect Containment:1/Hips widely abducted,in plasteror in removable splint 2/Varus osteotomy of femur or pelvis

29
Fractures Greenstick fractures Injuries of physis

32
Thank you

Similar presentations











 MB BS BSc MSc (SEM) MRCS (Eng) Diploma in MM (UIAA)>")
>")












