Download presentation
Presentation is loading. Please wait.

2
Nutrition Counseling Dr. A.Nadjarzadeh PhD, Nutritionist

3
Objective Learn how to counsel a patient to improve diet and physical activity in a manner that is effective, minimizes frustration, shows respect for the patient and maintains good communication

4
Case study Ms X is a 51 year old nurse who came in 3 weeks ago and saw a doctor for her sinus infection. That doctor was not her PCP and referred her to her PCP, Dr. D for a health maintenance visit and follow-up of her sinus infection. He also had her come in last week for a fasting lipid profile and blood glucose.

5
Lab: Total Cholesterol 270 LDL “ 175 HDL “ 30 Fasting Glucose 125 Today’s vital signs: Weight 195# Height 5’4” Blood Pressure 150/95 BMI 33.54

6
And now Dr. D will demonstrate how to counsel Ms. X to improve her lifestyle and reduce her reduce CHD risk!

7
Is Dr. D’s advice likely to help Ms. X?

8
By the end of the counseling session, Dr. D should have known Ms. X’s diet and habits known whether she is interested in changing any aspect of her lifestyle known whether she is ready to implement a weight loss plan in the next month appropriately counseled her regarding her risks, diet, and lifestyle

9
A Quick Guide to Lifestyle Counseling: The 5A Technique

10
The 5-A Technique ASK ADVISE ASSESS ASSIST ARRANGE

11
ASK Would the patient would benefit from changes in nutrition or physical activity?

13
ASK Would the patient would benefit from changes in nutrition or physical activity? If yes, perform diet, habit, and nutrition assessments

14
Diet and Habit Assessment AFFECTSAFFECTS

15
The 5-A Technique ASK ADVISE ASSESS ASSIST ARRANGE

16
ADVISE Advise patient to change the behavior Make it personally relevant Make it brief “I’d advise you to change this behavior because...” the risks of behavior benefits of changing behavior

17
Advice Example: Physical Activity “ you should get 30 minutes of physical activity most days because you have several risks for CHD and physical activity can lower all of these risks (Obesity, High LDL Cholesterol, Low HDL Cholesterol, Diabetes, Hypertension, risk of MI)”
")
18
Possible Dietary Advice Calories to maintain ideal body weight Less than 30% of calories from fat Low saturated and trans fat (as low as possible below 10% of calories) 20-35 grams of fiber/day At least 5 fruits and vegetables/day < 2.5 grams sodium (6 grams salt)/day 0.4 mg of folate and 1200 mg of calcium/day Less than 2 alcohol drinks/d (1 for women)
 grams of fiber/day At least 5 fruits and vegetables/day < 2.5 grams sodium (6 grams salt)/day 0.4 mg of folate and 1200 mg of calcium/day Less than 2 alcohol drinks/d (1 for women)")
19
The 5-A Technique ASK ADVISE ASSESS ASSIST ARRANGE

20
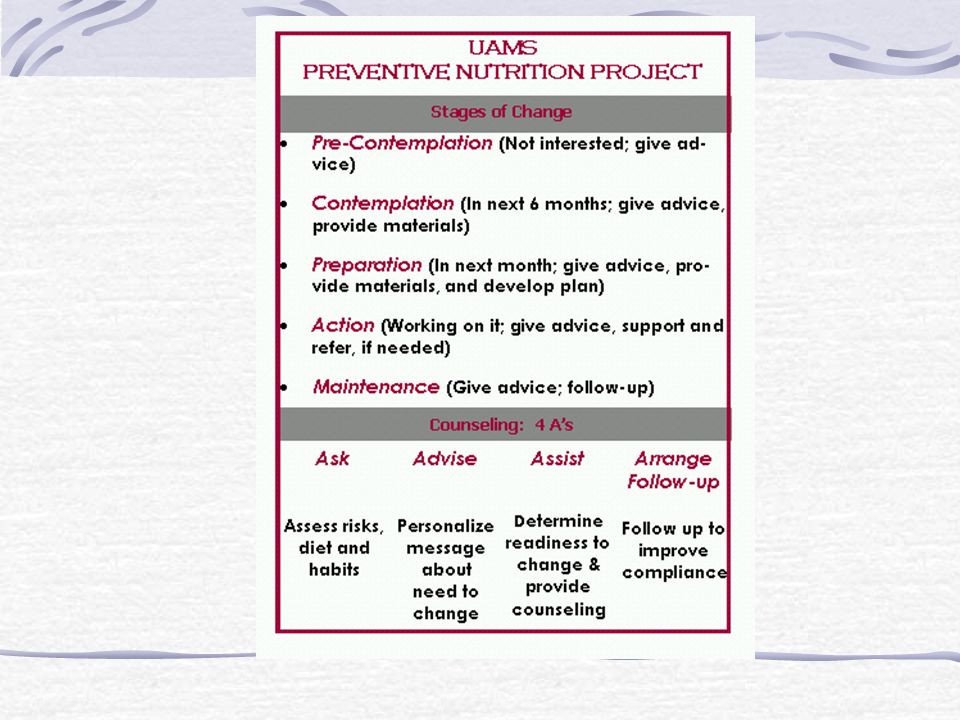
Assess Patient’s Readiness to Change: Pre-contemplation (not interested) Contemplation (within 6 months) Preparation (within a month) Action (working on it) Maintenance
 Contemplation (within 6 months) Preparation (within a month) Action (working on it) Maintenance")
22
The 5-A Technique ASK ADVISE ASSESS ASSIST ARRANGE

23
Assist How to assist depends upon readiness to change and barriers to change

24
Pre-contemplation (not interested) ASSISTANCE: Offer educational material Invite future inquires
 ASSISTANCE: Offer educational material Invite future inquires")
25
Contemplation, Preparation, Action, Maintenance ASSISTANCE: 1. Identify barriers to change 2. Address barriers: Provide educational materials Inform of programs available in the community Offer referral as needed for intensive counseling

26
Barriers to Change Typical barriers might include: u Hunger or withdrawal symptoms u Fear of failure u Lack of support (family, friends, co-workers) u Depression u Unrealistic goals u Environmental barriers u Financial concerns
 u Depression u Unrealistic goals u Environmental barriers u Financial concerns")
27
Barriers to Change Solutions might include: u Problem solving u Support groups u Psychotherapy u Medication

28
Educational Materials

29
Support Programs

30
Referral Psychotherapist Personal trainer Group program Health educator Dietician

31
Counseling Services that can be Provided by Dieticians Detailed diet assessment, including readiness to change and barriers to change In depth dietary counseling (counting calories, choosing healthier foods, shopping, motivational tools, food models, etc.) Frequent follow-up
 Frequent follow-up")
33
The 5-A Technique ASK ADVISE ASSESS ASSIST ARRANGE

34
ARRANGE FOLLOW-UP During current visit: schedule follow up (generally within 2 weeks) At the follow-up visit: find out how patient is doing recycle patients who have restarted unhealthy behavior or are having problems
 At the follow-up visit: find out how patient is doing recycle patients who have restarted unhealthy behavior or are having problems")
35
Counseling to modify lifestyle: The 5A’s Ask: assess risks Advise: give brief advice to change (all patients!) Assess: determine stage of readiness to change Assist: provide materials; identify and address barriers and/or make referrals if ready Arrange: follow-up to improve compliance
 Assess: determine stage of readiness to change Assist: provide materials; identify and address barriers and/or make referrals if ready Arrange: follow-up to improve compliance")
36
And now Dr. P will demonstrate how to counsel Ms. X to improve her lifestyle

37
What are this patient’s diet and lifestyle habits?

38
Diet and Habit Assessment

39
What is Ms. X’s stage of readiness to change her diet? 1. Pre-contemplation 2. Contemplation 3. Preparation 4. Action 5. Maintenance

40
What is Ms. X’s stage of readiness to increase physical activity? 1. Pre-contemplation 2. Contemplation 3. Preparation 4. Action 5. Maintenance

41
What is Ms. X’s stage of readiness to quit smoking? 1. Pre-contemplation 2. Contemplation 3. Preparation 4. Action 5. Maintenance

42
Is Dr. P’s advice likely to help Ms. X lose weight?

43
Treating Obesity Without Frustration Define “success” generously Use a systematic approach: 5A’s Assess readiness to change Assess barriers to change Use appropriate tools to assess motivation Address obstacles creatively Determine whether referral is appropriate and to whom patient should be referred Frequent follow-up for patients in preparation, action, or maintenance

44
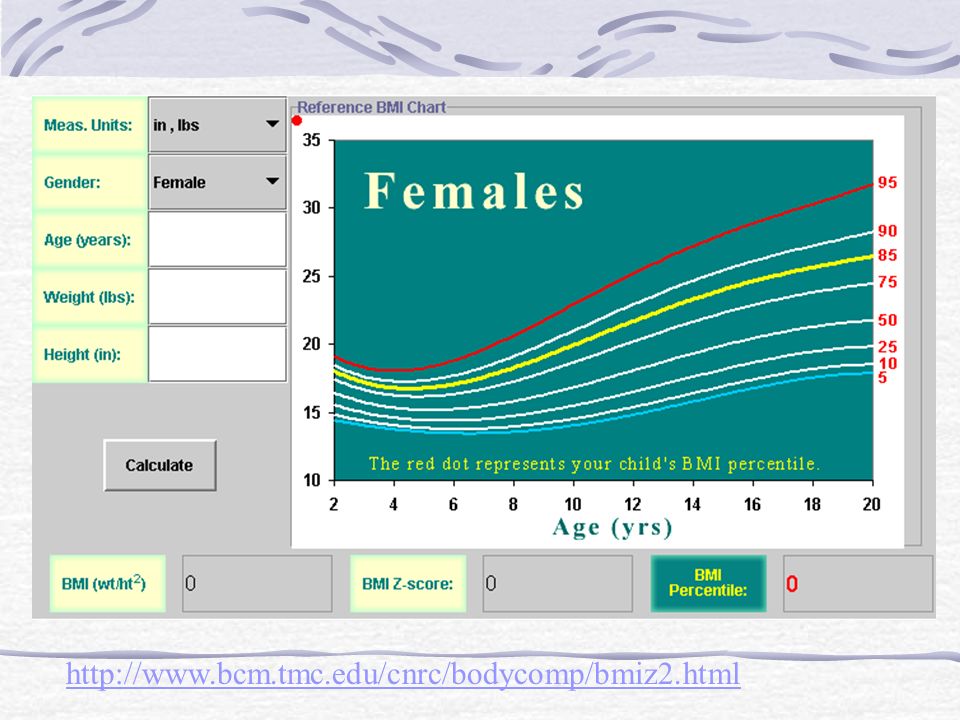
Counseling Overweight Children Step 1: Calculate BMI Step 2: Determine BMI Percentile Step 3: Interpret the Risk Step 4: Choose a course of action ARKANSAS CLINICIAN’S GUIDE TO WEIGHT PROBLEMS IN CHILDREN AND ADOLESCENTS

46
http://www.bcm.tmc.edu/cnrc/bodycomp/bmiz2.html
47
At Risk of Overweight: Patients with a personal or family history of co-morbidities need full evaluation for overweight If no history of co-morbidities, encourage healthy lifestyle and follow up in 1 year to recheck BMI

48
Overweight: Needs full evaluation and treatment for overweight

49
Assess Overweight Age first noted Perceived causes by child and parent Prior weight loss attempts Time in sedentary activities (TV, video games, computer) Time in physical activity (sports, walking, outdoor play) Body image, family stress and any depressive symptoms
 Time in physical activity (sports, walking, outdoor play) Body image, family stress and any depressive symptoms")
50
Assess Co-Morbidities Family History: obesity, diabetes, hyperlipidemia, HTN, MI, stroke PMH: chronic diseases ROS: sleep apnea, worsening asthma, exercise intolerance, reflux, limb pain, emotional difficulties, menstrual irregularities

51
Assess Diet Milk/dairy (should be 3-5 servings a day of skim or 1%) Fruits and vegetables (should be 5-9 servings a day) Intake of soft drinks and fruit and sugar drinks Fast food consumption Food behavior (large portions, skipping meals, eating while watching TV, high calorie snacking, binge eating)
 Fruits and vegetables (should be 5-9 servings a day) Intake of soft drinks and fruit and sugar drinks Fast food consumption Food behavior (large portions, skipping meals, eating while watching TV, high calorie snacking, binge eating)")
52
Physical Examination Body habitus, BP (age appropriate), chest, extremities, acanthosis nigricans, thyromegaly, striae Labs Cholesterol panel Consider fasting glucose if FHx of type 2 diabetes or signs of insulin resistance Other lab based on individual findings
, chest, extremities, acanthosis nigricans, thyromegaly, striae Labs Cholesterol panel Consider fasting glucose if FHx of type 2 diabetes or signs of insulin resistance Other lab based on individual findings")
53
Clinical Pearls First goal is no further weight gain. Children may "grow into" their weight as their height increases. Increase fruits and vegetables, use skim or 1% milk. Decrease sugared drinks, candy, junk and fast foods. Turn off the TV while eating. Remove unhealthy snacks from view. Put out fruits and vegetables. Regular meal times including breakfast. Child’s fist- size portions only. Limit snacking to healthy foods.

54
Encourage anything that increases breathing and heart rate (brisk walking, bicycling, dancing, other sports). Work up to one hour a day. Set limits on TV, video, and computer time (2 hrs/day total). Self-monitoring is one of the most helpful tools. Have them record physical activity and diet, weigh every 2-4 weeks. Review records when patient comes back and give praise and/or problem solve.
. Self-monitoring is one of the most helpful tools. Have them record physical activity and diet, weigh every 2-4 weeks. Review records when patient comes back and give praise and/or problem solve..")
55
Parents should act as role models, play with children, and eat meals together at the table at home. If child continues to have inappropriate weight gain, reassess for compliance or the presence of emotional problems. Consider referral for problems beyond your scope of management such as co-morbidities, possible abuse or severe psychopathology

56
Counseling Practice Session Objectives Determine the patient’s stage of readiness to change Provide brief, personalized advice explaining the behavior that should be changed and why Assist the patient in a manner that is appropriate for the stage of readiness to change

57
Counseling Practice Session: Logistics 4 cases For each case, one student role plays patient (script available) Two students role play physician (may tag team and or use time in-time out) Educational handouts will be available on physical activity, diet, and smoking Clinician’s guide is available for content on the pediatric case
 Two students role play physician (may tag team and or use time in-time out) Educational handouts will be available on physical activity, diet, and smoking Clinician’s guide is available for content on the pediatric case")
Similar presentations




 describes relative weight for height: weight (kg)/height (m 2 ) Overweight = 25–29.9 BMI Obesity = >30 BMI.>")








 is a measure used to determine childhood overweight.>")






