Download presentation
Presentation is loading. Please wait.

1
The spectrum of renal scarring
Parvex, Willi, Kossovsky, Girardin, pediatric nephrology, Geneva University, Switzerland

2
Background UTI is common condition in childhood with a prevalence of 3%, the prevalence of pyelonephritis (PNA) is not clearly reported Infant and children presenting unexplained fever of ≥ 38° and positive urine culture will be diagnosed with PNA

3
Background The goal of medical management of PNA
Initiate early treatment to decrease renal inflammation and subsequently scars Identify risk factor to avoid new infections episodes and prevent scars development Exclude urologic anomalies (renal echography) Detect vesico-ureteral reflux (cystography)
 Detect vesico-ureteral reflux (cystography)")
4
Pathogenesis of scars It is important to differentiate acquired segmental scarring associated with VUR and PNA From congenital “scars” corresponding to an anomaly in the metanephric development in boys and associated with high grade VUR Histological analyses of these later lesions showed renal dysplasia which may mimic scarring without an acute episode of PNA

5
Renal scintigraphy Since 1980, renal scintigraphy with TechnetiumTc labeled with dimercapto-succinyl-acid DMSA replaced IVP and improved in the detection of renal scars has been validated to be the most sensitive method for imaging in the diagnosis of acute PNA and for renal scars

6
Normal kidney Acute PNA Renal scars

7
What is known form the literature
Did early antibiotic treatment avoid scar formation? How important is the grade of VUR? Is the risk to do scars related to age? Are scars leading to hypertension (HTA) in adulthood?
 in adulthood")
8
Early treatment (T)? Recent data suggest that if early T decrease renal inflammation in the acute phase However in this patients (n=186) early T seems not to decrease the risk of later scars (T<24H or T>24H) Doganis, D. et al. Pediatrics 2007;120:e922-e928
 early T seems not to decrease the risk of later scars (T<24H or T>24H) Doganis, D. et al. Pediatrics 2007;120:e922-e928.")
9
Role of VUR? VUR is considered to be the principal risk factor to favor PNA and therefore renal scars The incidence of VUR in children presenting PNA varies among studies from 30 to 50% Even if scars can develop without VUR or low grade VUR however the risk increased with high grade VUR

10
VUR and severity of scars
Gonzalez et al. The Journal of Urology , Volume 173 , Issue 2 , Pages

11
Age and risk factor Benador et al Vol 379, January 1997, Pages 17-19

12
Vol 379, January 1997, Pages 17-19

13
HTA One of the main concern are further development of hypertension in children presenting scars Hypertension affects among series 5-27% of children; however the literature have not showed strong evidence until known

14
Risk for the future: HTA
A 15 years follow-up of BP studied 78 Pts with reflux nephropathy All were normal BP at time of inclusion 18/78 pts became HTA(>95th) during the following 15 years; 6 from them had a family history for HTA
 during the following 15 years; 6 from them had a family history for HTA.")
15
Systolic and diastolic BP at 5,10,15 years follow-ups
Chulananda et al. Vol 347, March 9,1996

16
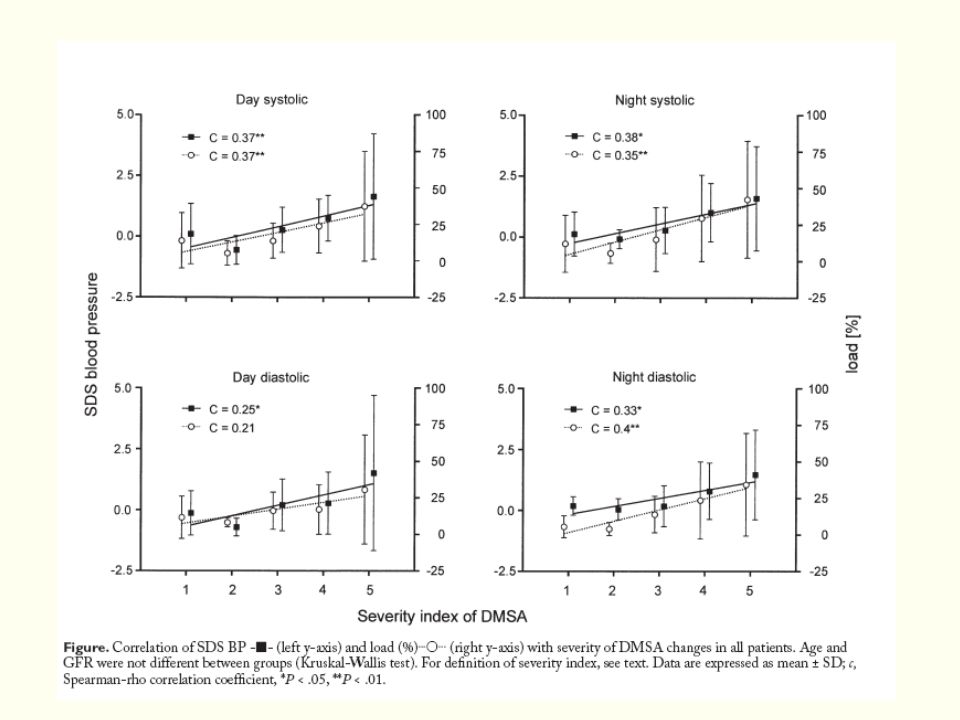
Risks for the future: HTA
The following recorded 24HBP in 61 pts classified in different groups according to the severity of DMSA lesions Type 1: normal reniforme shape but polar area with photon deficiency Type 2: focal defect in a nondeformed kidney Type 3: Smaller kidney compared to controlateral Type 4a:Loss of renal contour with normal size kidney Type 4b:similar from above with small kidney

18
Is this increase of BP at night a sign of further evolution of HTA in adulthood needs to be confirmed by long term studies J Pediatr. Patzer et al 2003 Feb;142(2):
:")
19
What is the long term significance of scars?

20
Background The presence of lesions on DMSA 6 month after PNA are considered to be definitive kidney scars According to the literature the rate of acute lesions and later scars varies among studies

22
Questions? Did these lesions still have the potential to evolve after 6 month Did this lesions interfere with normal renal growth

23
Aim of the study To analyze long term progression of renal lesions in children with presence of scars on the first DMSA To assess long term renal growth To identify variables which could impact on renal growth in this children

24
Material This prospective study was conducted over two years and included Children from 0-18 years with a diagnosis of PNA and who presented renal scars 6 month after the first episode of PNA Exclusion criteria Children with complex uro-genital malformations, dysplastic kidneys, megaurether, hydronephrosis

25
Methods Each patient with scars was contacted to have a repeated DMSA 3 years later At the same time we repeated a renal echography to measure kidney size

26
To analyze progression of DMSA defects, RU was divided in 3 areas
Scar progression was analyzed separately for each area by 3 observers in a blinded fashion and classified as follow No change Partial resolution Total disappearance Upper pole Mid zone Lower pole

27
b b a a 1B 1A 1A DMSA 6 month after PNA 1B DMSA 3 years later: we observe 2 types of lesions: a) the lesion situated in the mid-zone of left kidney did not change b) The lesion located in the right upper pole improved. 2A a a 2A b 2B b 2A DMSA 6 month 2B DMSA 3 years later: we observe a) disappearance of mid-zone lesion of left kidney b) no change in lower lesion of right kidney Parvex et al The Journal of Urology on Press
 the lesion situated in the mid-zone of left kidney did not change b) The lesion located in the right upper pole improved. 2A. a. a. 2A. b. 2B. b. 2A DMSA 6 month 2B DMSA 3 years later: we observe a) disappearance of mid-zone lesion of left kidney b) no change in lower lesion of right kidney. Parvex et al The Journal of Urology on Press.")
28
Kidney growth (cm) Kidney size was measured Time 0 corresponding to the PNA (T0) and 3 years later Time 3 (T3) at the same time of the repeated DMSA
 Kidney size was measured Time 0 corresponding to the PNA (T0) and 3 years later Time 3 (T3) at the same time of the repeated DMSA.")
29
*AJR Am J Roentgenol 1984;142(3):467-9.
Renal size was measured at T0 and T 3 and values compared to standard deviation score (SDS ) renal sizes* relative to age The following equation were used*to calculate Z-score *<1 year length (cm)= x age(mths)(t90 = 6.86, p<0.001;SD=0.69;r2=0.3437 *≥ 1 year length (cm)= x age(years)(t326 = 28, <0.001;SD=0.79;r2=0.7077 Renal growth between T0 and T3 was calculated with the ∆z-score = or + ∆z-score correspond to adequate renal growth - ∆z-score correspond in loss of renal growth *AJR Am J Roentgenol 1984;142(3):467-9.
 renal sizes* relative to age. The following equation were used*to calculate. Z-score. *<1 year length (cm)= x age(mths)(t90 = 6.86, p<0.001;SD=0.69;r2= *≥ 1 year length (cm)= x age(years)(t326 = 28, <0.001;SD=0.79;r2= Renal growth between T0 and T3 was calculated with the ∆z-score. = or + ∆z-score correspond to adequate renal growth. - ∆z-score correspond in loss of renal growth. *AJR Am J Roentgenol 1984;142(3):")
30
Results 50 (30G:20B) children; M age of 4.1
Boys were younger 15/20 ≤2years(75%) against 9/30 (30%) girls VUR was present in 36% of patients and 25% of renal units (RU)
 against 9/30 (30%) girls. VUR was present in 36% of patients and 25% of renal units (RU)")
31
Incidence and evolution of VUR

32
Number of scars & Grade of VUR
P=0.01 Number of scars NO VUR VUR GI-II VUR GIII-IV Parvex et al The Journal of Urology in Press

33
Progression of renal scars
% scar improvement 27% 63% 9% no change partial improvement total disappearance Altogether 72% of lesions improved over 3 years

34
Impact of scars on kidney growth
Analyze Coefficient ∆z-score Significance (p) 95% conf. interval 1 defect* Reference - 2 defects -0.32 0.41 -1.09 to 0.45 3 defects -0.81 -2.75 to 1.14 4 defects -1.59 0.000 -2.10 to -1.09 5 defects -1.73 0.006 -2.94 to -0.51 Table1: Univariate linear regression analysis of the association between the numbers of defects and renal growth (coefficient=∆ z-score) Parvex et al The Journal of Urology in Press
 95% conf. interval. 1 defect* Reference. - 2 defects to defects to defects to defects to Table1: Univariate linear regression analysis of the association between the numbers of defects and renal growth (coefficient=∆ z-score) Parvex et al The Journal of Urology in Press.")
35
Analyze coefficient Significance (p) 95% conf. interval Sex (M vs. F) 0.49 0.14 -0.16 to 1.14 Age (years) ≤ 1* (n=13) > 1 to ≤ 4 (n=20) > 5 (n=17) - 0.28 0.72 0.42 0.12 -0.41 to 0.96 -0.18 to 1.62 Total n° of defects (Per additional defect) -0.70 <0.001 -1.05 to -0.35 Lesions progression (Improvement vs. no change) 0.70 0.15 -0.26 to 1.66 Grade of VUR at time of PNA No reflux * Grade I or II Grade III or IV 0.34 -0.21 to 1.72 -0.36 to 1.02 Improvement of VUR >3 years (Yes vs. No) 0.25 0.23 -0.17 to 0.67 Persistence of VUR >3 years (Yes vs. No) -1.67 to 0.30 Surgery (Yes vs. No) 0.41 -0.36 to 0.86 Table 2: Multivariable analysis of factors associated with renal growth (coefficient = ∆z-score) Parvex et al The Journal of Urology in Press
 ≤ 1* (n=13) > 1 to ≤ 4 (n=20) > 5 (n=17) to to Total n° of defects. (Per additional defect) < to Lesions progression (Improvement vs. no change) to Grade of VUR at time of PNA. No reflux * Grade I or II Grade III or IV to to Improvement of VUR >3 years (Yes vs. No) to Persistence of VUR >3 years (Yes vs. No) to Surgery (Yes vs. No) to Table 2: Multivariable analysis of factors associated with renal growth (coefficient = ∆z-score) Parvex et al The Journal of Urology in Press.")
36
In summary The topographic analyses of renal defects over 3 years showed 72% of improvement The number of scars were statistically significantly higher in RU with high grade VUR versus low grade or no VUR. Parvex et al The Journal of Urology in Press

37
Loss of kidney growth over 3 years was observed
with an increased number of scars and this was highly significantly >3 scars persistence of VUR>3 years The kidney growth did not seem affected by Sexe, age Grade of VUR Improvement of DMSA defects Parvex et al The Journal of Urology in Press

38
Conclusion Renal defects seen at 6 month post PNA can still evolve with time and this raise the question of the definition of scars From this study preventing additional renal defects seems to be the best way to optimize kidney growth during childhood Parvex et al The Journal of Urology on Press

39
Open questions and further perspectives
Improve knowledge of the congenital “scar” associating renal dysplasia and HGVUR To define if the best way to prevent renal lesions in high grade VUR is prophylaxis? surgery? Long term studies to assess the risk HTA in scarred kidneys, with decreased renal growth

40
Thanks' for your attention

Similar presentations





 patients Policy.>")





 Lecture 5: Discussion Dr. Avraham Samson Faculty of Medicine in the Galilee 1.>")








