Download presentation
Presentation is loading. Please wait.

1
Is surgical resection justified for myasthenia gravis? Long-term results in over 1000 cases. Andrew J. Kaufman, MD; Justin Palatt, MD; Mark Sivak, MD, Peter Raimondi, BS, Dong-Seok Lee, MD; Andrea Wolf, MD, MPH; Fouad Lajam, MD, Faiz Bhora, MD; Raja M. Flores MD. Department of Thoracic Surgery, Mount Sinai School of Medicine Andrew J. Kaufman MD Assistant Professor, Thoracic Surgery Mount Sinai School of Medicine Chief, Thoracic Surgery Mount Sinai Beth Israel New York, New York

2
Disclosures None

3
Background Myasthenia gravis (MG) is a rare autoimmune disease Prevalence 0.5 to 20.5 per 100,000 Symptoms: Ocular, bulbar, and generalized Frequently causes severe disability in those affected Uncommonly fatal Treatment: 1930’s Anticholinesterases 1950’s Immunosuppressants 1970’s Plasma exchange (PLEX) and IVIG 1913, 1939-1945 Thymectomy introduced Role of thymectomy remains controversial AAN recommendation as “Optional” 1. 1 Gronseth GS, Barohn RJ. Neurology 2000;55:7-15

4
Goal of Study Evaluate the role of thymectomy in the treatment of MG. Focus of Study: Long-term outcomes Appropriate statistical analysis Endpoints: Accurately determine rate of complete stable remission (CSR) Determine if surgical technique affects rate of CSR Describe patient characteristics affecting rate of CSR
 Determine if surgical technique affects rate of CSR Describe patient characteristics affecting rate of CSR.")
5
Methods Retrospective review of a prospectively maintained database of thymectomy patients from 1941-2013. 1002 included in study. Inclusion Criteria: Thymectomy Age at time of surgery Gender Duration of symptoms before surgery Osserman Classification before and after surgery Surgical technique Presence of thymoma Date of remission, and status at last follow-up

6
Methods Statistical design: Complete stable remission and patient variables were analyzed: Chi squared Wilcoxin signed-rank test Crude rate percentage Interval-censored Kaplan-Meier Estimate Interval-censored Cox proportional hazards model

7
Methods Definitions: Complete Stable Remission: asymptomatic off all medications for 1 year postoperatively. Modified Osserman Classification: Class I: ocular Class II: mild generalized/bulbar weakness Class III: moderate generalized/bulbar weakness Class IV: severe generalized weakness or respiratory dysfunction or both.

8
Surgical Technique Thymectomy consisted of removal of all thymic tissue including cervical poles and standard resection of mediastinal fat between the phrenic nerves, from thyroid to diaphragm. Using 4 approaches: Transcervical : no sternal split Trans-sternal: no formal neck dissection Thoracotomy VATS

9
Results: Patient Characteristics Total N = 1002 Complete Stable Remission N = 191 No Remission N = 811 p -value Years follow-up median (IQR) 6.0 (1-10)9.0 (7-12)4.0 (1-10)<.0001 Age at time of thymectomy, mean in years (SD) 40.8 (17.4)37.2 (16.5)41.7 (17.5)0.0012 Gender (N,%) Male350 (34.9%)67 (35.1%)283 (34.9%)0.9619 Female652 (65.1%)124 (64.9%)528 (65.1%) Years from Dx to thymectomy, Median (IQR) 1.0 (0-3) 0.3708
 6.0 (1-10)9.0 (7-12)4.0 (1-10)<.0001 Age at time of thymectomy, mean in years (SD) 40.8 (17.4)37.2 (16.5)41.7 (17.5) Gender (N,%) Male350 (34.9%)67 (35.1%)283 (34.9%) Female652 (65.1%)124 (64.9%)528 (65.1%) Years from Dx to thymectomy, Median (IQR) 1.0 (0-3)")
10
Results: Patient Characteristics Total N = 1002 Complete Stable Remission N = 191 No Remission N = 811 p -value Preop Osserman (N,%) Class I74 (7.4%)12 (6.3)62 (7.6%) Class II777 (77.5%)159 (83.2%)618 (76.3%)0.1068 Class III118 (11.8%)18 (9.4%)100 (12.3) Class IV33 (3.3%)2 (1.1%)31 (3.8%) Presence of Thymoma (N,%) Yes163 (16.3%) 13 (6.8%)150 (18.5%) No893 (83.7%)178 (93.2%)661 (81.5%)<.0001
 Class I74 (7.4%)12 (6.3)62 (7.6%) Class II777 (77.5%)159 (83.2%)618 (76.3%) Class III118 (11.8%)18 (9.4%)100 (12.3) Class IV33 (3.3%)2 (1.1%)31 (3.8%) Presence of Thymoma (N,%) Yes163 (16.3%) 13 (6.8%)150 (18.5%) No893 (83.7%)178 (93.2%)661 (81.5%)<.0001")
11
Results: Patient Characteristics Total N = 1002 Complete Stable Remission N = 191 No Remission N = 811 p -value Surgical Technique (N,%) Transcervical744 (74.25%)158 (82.7%)586 (72.3%) Trans-sternal199 (19.86%)25 (13.1%)174 (21.5%) Thoracotomy43 (4.29%)6 (3.1%)37 (4.5%) VATS16 (1.6%)2 (1.1%)14 (1.7%)0.0306
 Transcervical744 (74.25%)158 (82.7%)586 (72.3%) Trans-sternal199 (19.86%)25 (13.1%)174 (21.5%) Thoracotomy43 (4.29%)6 (3.1%)37 (4.5%) VATS16 (1.6%)2 (1.1%)14 (1.7%)0.0306")
12
Crude Rate Results Category of ResponseNumber of PatientsPercent of Patients Complete Stable Remission191/100219% Improvement164/100216.3% Stable580/100258% Progression67/10026.7%

13
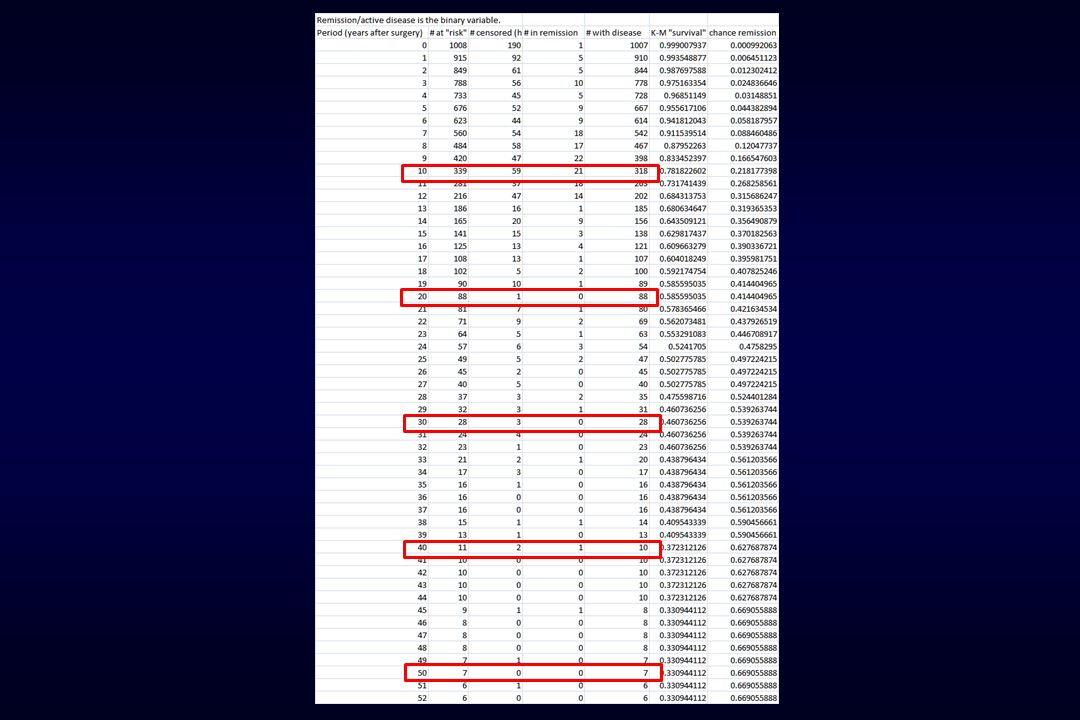
Interval-censored Kaplan-Meier estimate of time to complete stable remission Time to Remission in years Cumulative Probability of CSR

14
Multivariate Cox Model Chi SquareP-value Hazard Ratio of CSR 95% CI Age at time of Surgery0.05560.81361.0010.992-1.011 Gender0.94170.33181.1720.851-1.615 Duration of Symptoms3.36090.06680.9710.942-1.002 Presence of Thymoma7.4730.00630.4080.215-0.776 Preop Osserman Class IRef Class II1.05970.30330.7250.393-1.377 Class III4.61210.03170.4320.200-0.929 Class IV5.66450.01730.1570.031-0.721 Surgical Technique TranscervicalRef Trans-sternal5.73790.0160.5770.345-0.899 Thoracotomy0.06440.79971.1240.455-2.775 VATS1.88990.16922.7440.651-11.56

15
Key Points Our Study, is the largest single-center retrospective study of thymectomy patients to date, and reports long- term outcomes. Thymectomy associated with high rate of CSR: 47.3% maximal rate. CSR rates increase steadily over time Crude rate underestimates CSR Thymoma decreased the likelihood of CSR. Trans-sternal thymectomy lower probability of CSR Osserman Classification III and IV patients fared worse.

16
Limitations of the Study Retrospective Long time span of the study Did not use MGFA Classification of symptoms Lack specific data: Antibody status (AchR-ab, MUSK) Histology WHO classification and Masaoka Staging of thymomas Medication regimen and dosing not accounted for
 Histology WHO classification and Masaoka Staging of thymomas Medication regimen and dosing not accounted for")
17
Conclusions Thymectomy is associated with a high rate of complete stable remission Thymectomy should be recommended for patients with myasthenia gravis Especially those with nonthymomatous myasthenia and mild symptoms

18
Acknowledgements Joan Bratton Department of Neurology Icahn School of Medicine at Mount Sinai Emilia Bagiella PhD and Evie Andreopoulos Director, Center for Biostatistics Department of Population and Health Sciences Icahn School of Medicine at Mount Sinai

19
Thank You

20
Discussion

Similar presentations


, FACS, FCCP Department of Surgery. Division of Cardiothoracic.>")










 following definitive chemoradiotherapy.>")





