Download presentation
Presentation is loading. Please wait.

1
NAME: Dr. ANGGRAINI DWI S.,dr.,Sp.Rad (K) BORN : PASURUAN, SEPTEMBER 12, 1961 EDUCATION : GP, MEDICAL FACULTY OF AIRLANGGA UNIVERSITY, 1987 RADIOLOGIST, AIRLANGGA UNIVERSITY, 1996 ATTACH PROGRAM NNI SINGAPORE, 2002 NEURORADIOLOGIST CONSULTANT, 2004 DOCTOR, MEDICAL FACULTY OF AIRLANGGA UNIVERSITY, 2013 POSITION : STAFF OF DEPT. RADIOLOGY MED. FAC. AIRLANGGA UNIVERSITY HEAD OF DIPLOMA PROGRAM FOR RADIOGRAPHER MEMBER OF NEURORADIOLOGICAL DIVION. MEDICAL FACULTY AIRLANGGA UNIV. MEMBER OF IDI MEMBER OF DKJ FORUM MEMBER OF PDSRI MEMBER OF AONHCR MEMBER OF ASCI OFFICIAL JOURNAL OF INDONESIAN NEURORADIOLOGY OF THE EUROPEAN NEURORADIOLOGY JOURNAL SENIOR CONSULTANT IN NEURORADIOLOGY, SOETOMO HOSPITAL AND SEVERAL HOSPITALS IN SURABAYA HEAD OF RADIOLOGY, HUSADA UTAMA HOSPITAL MEDICAL MANAGER, HUSADA UTAMA HOSPITAL Curriculum Vitae
 BORN : PASURUAN, SEPTEMBER 12, 1961 EDUCATION : GP, MEDICAL FACULTY OF AIRLANGGA UNIVERSITY, 1987 RADIOLOGIST, AIRLANGGA UNIVERSITY, 1996 ATTACH PROGRAM NNI SINGAPORE, 2002 NEURORADIOLOGIST CONSULTANT, 2004 DOCTOR, MEDICAL FACULTY OF AIRLANGGA UNIVERSITY, 2013 POSITION : STAFF OF DEPT. RADIOLOGY MED. FAC. AIRLANGGA UNIVERSITY HEAD OF DIPLOMA PROGRAM FOR RADIOGRAPHER MEMBER OF NEURORADIOLOGICAL DIVION. MEDICAL FACULTY AIRLANGGA UNIV. MEMBER OF IDI MEMBER OF DKJ FORUM MEMBER OF PDSRI MEMBER OF AONHCR MEMBER OF ASCI OFFICIAL JOURNAL OF INDONESIAN NEURORADIOLOGY OF THE EUROPEAN NEURORADIOLOGY JOURNAL SENIOR CONSULTANT IN NEURORADIOLOGY, SOETOMO HOSPITAL AND SEVERAL HOSPITALS IN SURABAYA HEAD OF RADIOLOGY, HUSADA UTAMA HOSPITAL MEDICAL MANAGER, HUSADA UTAMA HOSPITAL Curriculum Vitae.")
2
Differential Diagnosis of Brain Infection, Tumor, Metastatic Process on CT Scan and MRI Dr. dr. Anggraini Dwi S.,Sp.Rad.(K) Radiology Dept., Medical Faculty, Airlangga University/Soetomo Hospital, Surabaya
 Radiology Dept., Medical Faculty, Airlangga University/Soetomo Hospital, Surabaya.")
3
Clinical findings? Atlas Scott, 2007

4
Plain X-rayUSGCT ScanMRIPET Scan Radiation exp.+-++-+++ Tissue contrast+++ +++- Calcification++++++- Hydrocephalus-+++++++++- Contrast--++++++- Uptake rad farm----+++ Metabolite---+++- Tissue Perfusion--++ - Tissue Diffusion---+- Techniques in Neuroimaging

5
5 Brain lesion (infection, primary, metastatic): 1.Initial recognition and characterization of the lesion 2. The mechanical effects and structural deformities resulting from intracranial neoplasm

6
The Most effective Uses of CT in Neuroradiology Rulling out SAH Acute head trauma Fracture of skull, face, orbits Sinusitis Salivary gland calculous disease Subtle bony irregularities Detection of calcification in lesion Odontoic lesion Degenerative disease CTA CT perfusion Bony spinal stenosis MR is contraindicated Immediate postop evaluation Temporal bone disease

8
MR imaging has the most potential of any imaging technique to allow a complete and accurate diagnosis and initial management strategy to be formulated for a brain tumor

9
Brain Tumor Imaging with MR: Objectives Specific Diagnosis Neoplasma VS other Histology (Grading) Therapy Planning Localize for biopsy Delineate extent or spread RT portal design Guide minimally invasive surgery - Define peritumoral “eloquent” - Define neuroanatomic pathway involvement Post Treatment Residual Tumor Reccurent tumor VS treatment-related necrosis
 Therapy Planning Localize for biopsy Delineate extent or spread RT portal design Guide minimally invasive surgery - Define peritumoral eloquent - Define neuroanatomic pathway involvement Post Treatment Residual Tumor Reccurent tumor VS treatment-related necrosis")
10
Fundamentals of lesion localization and characterization: -The age of the patient -Single or multiple? -Intraaxial or extra axial? -Density/intensity? -Presence of contrast enhancement? -Hemorrhage -Calcification -Necrosis?

11
Basic protocol brain MRI 1.T1 2.T2 3.T2FLAIR 4.Gre T2* 5.DWI 6.2-3 planes post Gad T1 7.Pefusion CBV 8.MR Spectroscopy (?) 9.DTI (?) 10.Functional MRI (?)
 9.DTI ( ) 10.Functional MRI ( )")
14
Brain Lesions

15
MedScape, 2011

17
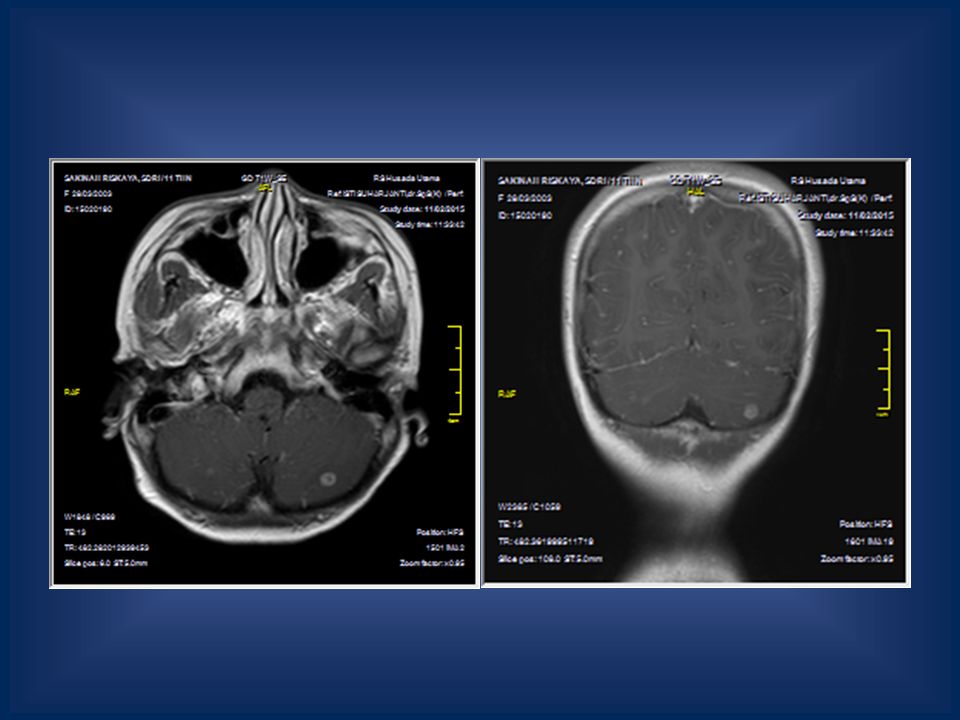
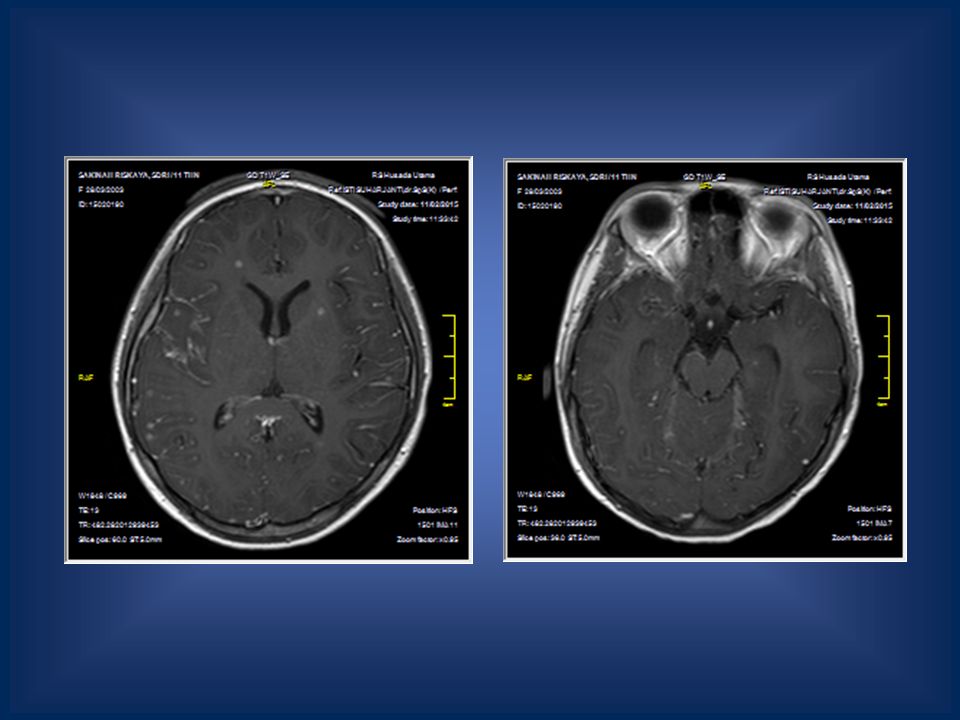
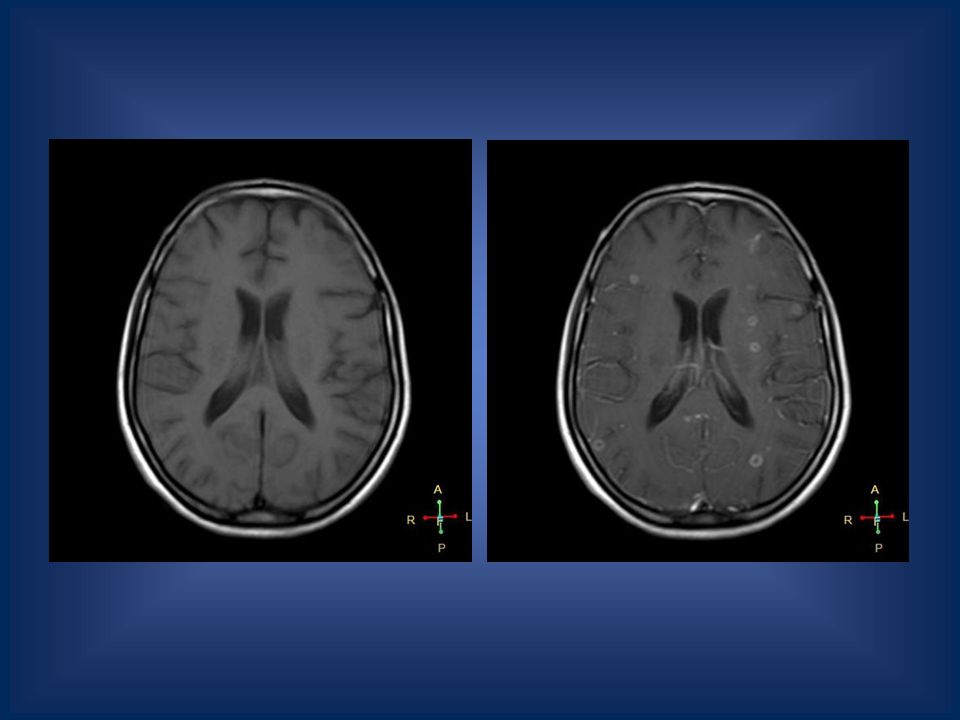
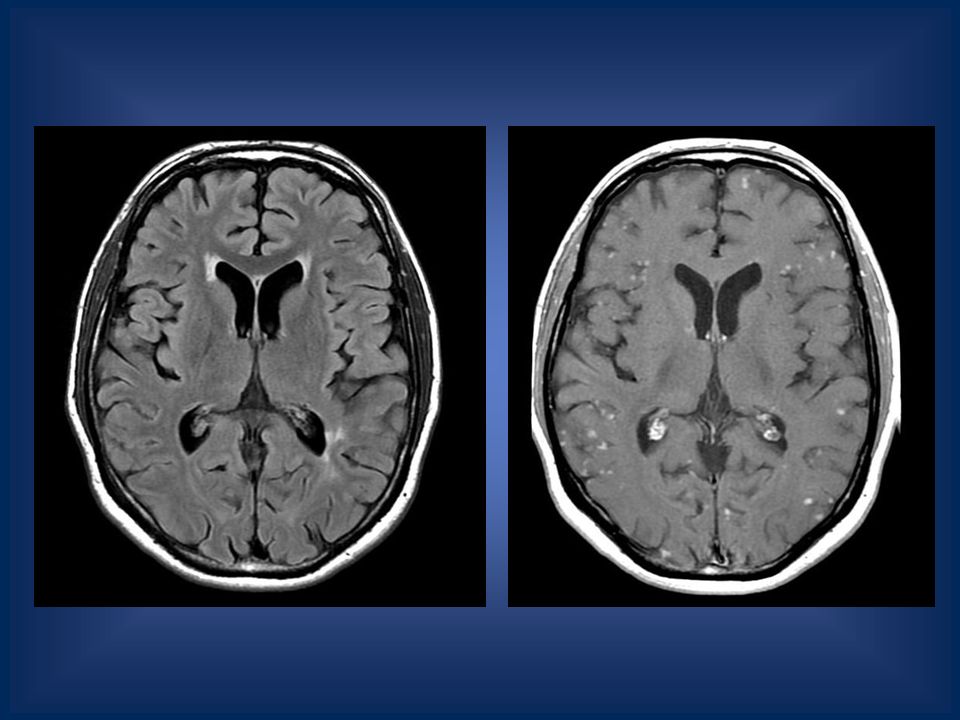
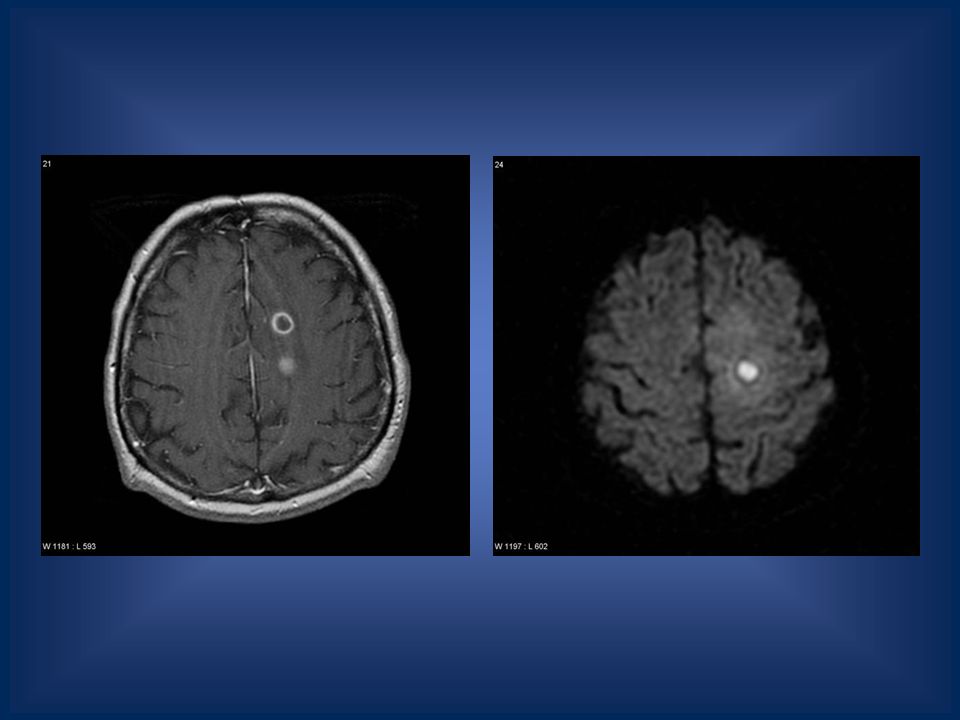
Multiple Small Ring Enhancing Lesions

18
Tuberkuloma CT Isodense or slight hyperdense basal cistern Basal homogenous meningeal enhancement Hydrocephalus (C and NC) Tuberculoma, rim enhancement, 1/3 with target sign (central calcification) MRI Cisternal enhancement ++ Meningeal enhancement (better in FLAIR than T2), patchy meningitis Hydrocephalus (C and NC) Tuberculoma, rim enhancement, 1/3 with target sign (central calcification)
 Tuberculoma, rim enhancement, 1/3 with target sign (central calcification) MRI Cisternal enhancement ++ Meningeal enhancement (better in FLAIR than T2), patchy meningitis Hydrocephalus (C and NC) Tuberculoma, rim enhancement, 1/3 with target sign (central calcification)")
23
Metastatic CT Hyperdense, hypodense or isodense Small, round zones Extensive collateral edema Intratumoral hemorrhage 80% enhancement, sometimes a ring MRI Detects 2-3x> MRI Typically hypointense on T1 Hyperintense on T2 Melanoma? Enhancement: uniform, punctate, ring T2FLAIR: perifocal edema MRS: No Cho↑ at perifocal edema, NAA↓

27
Neurosarcoidosis CT Leptomeningitis Suprasellar manifestation (diabetes incipidus) Hydrocephalus Single or multiple granuloma slightly hyperdense foci up to 1cm Up to 60% negative MRI T1: iso or hypointense T2: variable T1+C: homogenous enhancement Pituitary + hypothalamic Leptomeningeal involv. Cranial nerve (II,VIII)
.")
29
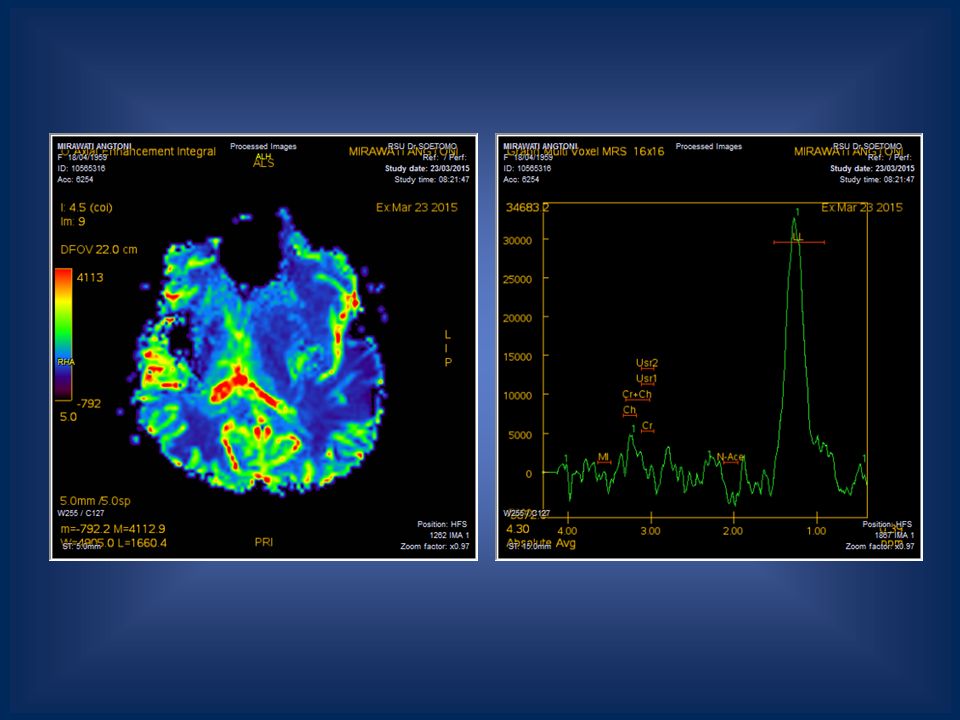
Cerebral Abscess CT Varies with stage of abscess Early cerebritis: hypodense Subacute: ring-like structure Necrotizing tissue Gas forming +/- Enhancing ring: 3-6mm, uniform Dughter abscess MRI Varies with stage of abscess T1W T2W FLAIR DWI (+) : hypercellularity, brain ischemia, cellular swelling due to cytotoxic edema Central liquefactive necrosis MRS : NAA, Cho,Cr ↓, LL↑
 : hypercellularity, brain ischemia, cellular swelling due to cytotoxic edema Central liquefactive necrosis MRS : NAA, Cho,Cr ↓, LL↑")
32
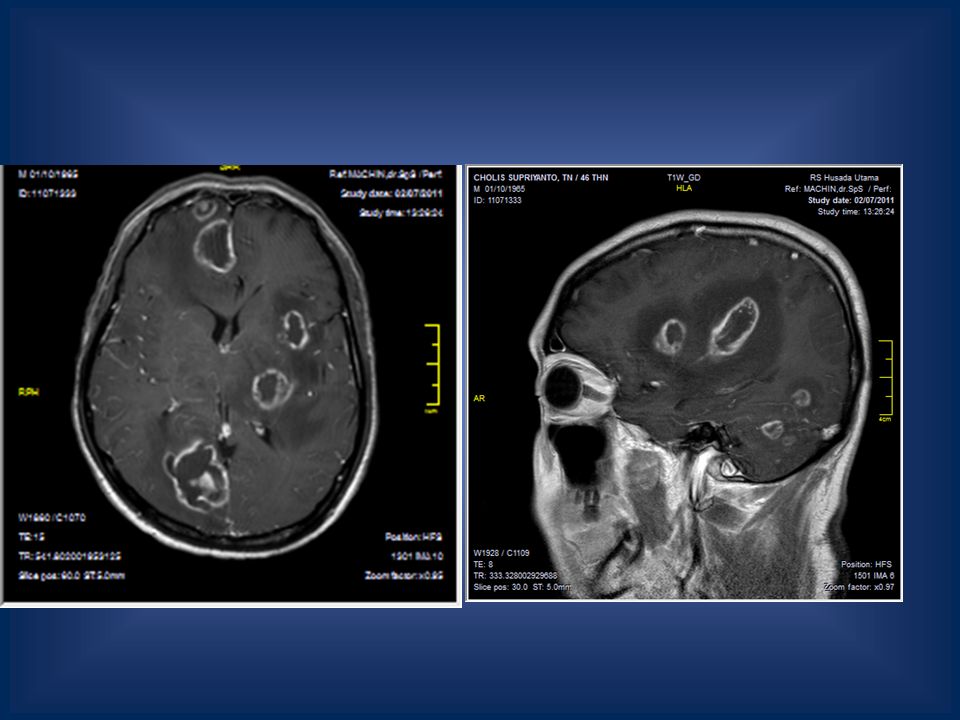
Multiple Large Enhancing Lesions

33
Abscess

37
Metastatic

41
Glioma

44
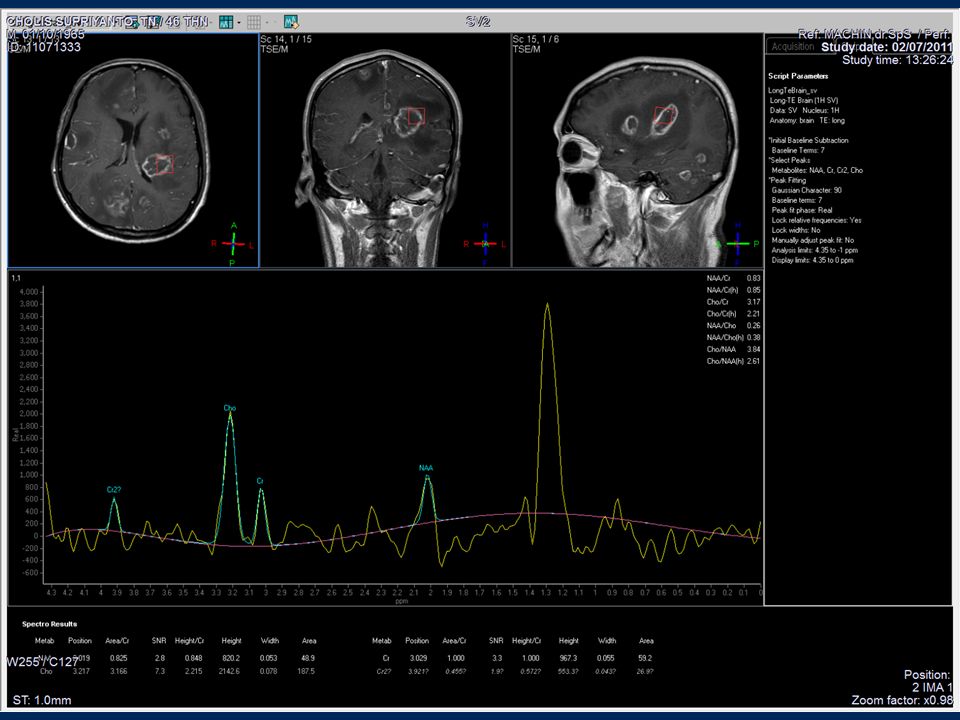
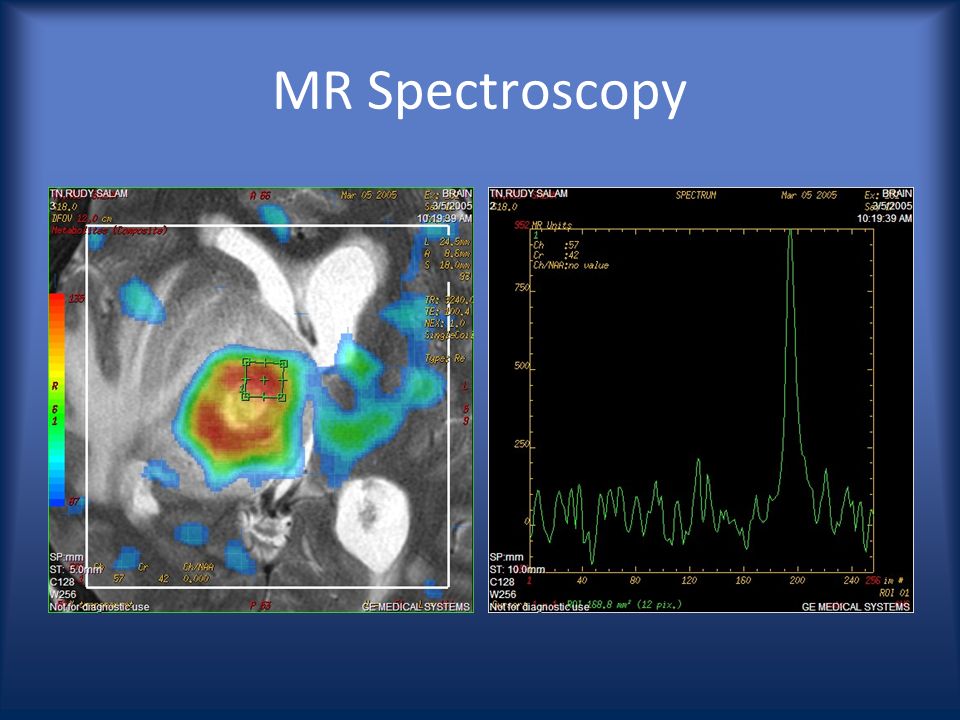
MR Spectroscopy

46
Tumeactive Demyelinating Lesion

51
HIV? Toxoplasma?

52
Unenhanced CT Scan MRI T1 WI

53
T1 WI

54
T2W axial

57
Enhanced T1W

58
Before Tx After Tx

59
Lymphoma?

63
TDL: tumeactive demyelinating lesion Metastase MR Spectroscopy Is there perienhancement infiltration Over 1 Cho/NAA ? Low grade neoplasm LymphomaPerfusion MR Is perfusion over 1,75 rCBV? Is there necrosis On CE MRI? Low grade neoplasm or encephalitis Conventional CE MRI Does the lesion enhance? MR Spectroscopy Is the elevation of Cho/NAA over 2,2? DWI, diffusing facilitated > 1,1/100 mm 2 /ADC? Intraaxial Brain Mass NO YES NO YES TDL or abscess Abscess High grade neoplasm NO YES NO YES High grade glioma YES NO

70
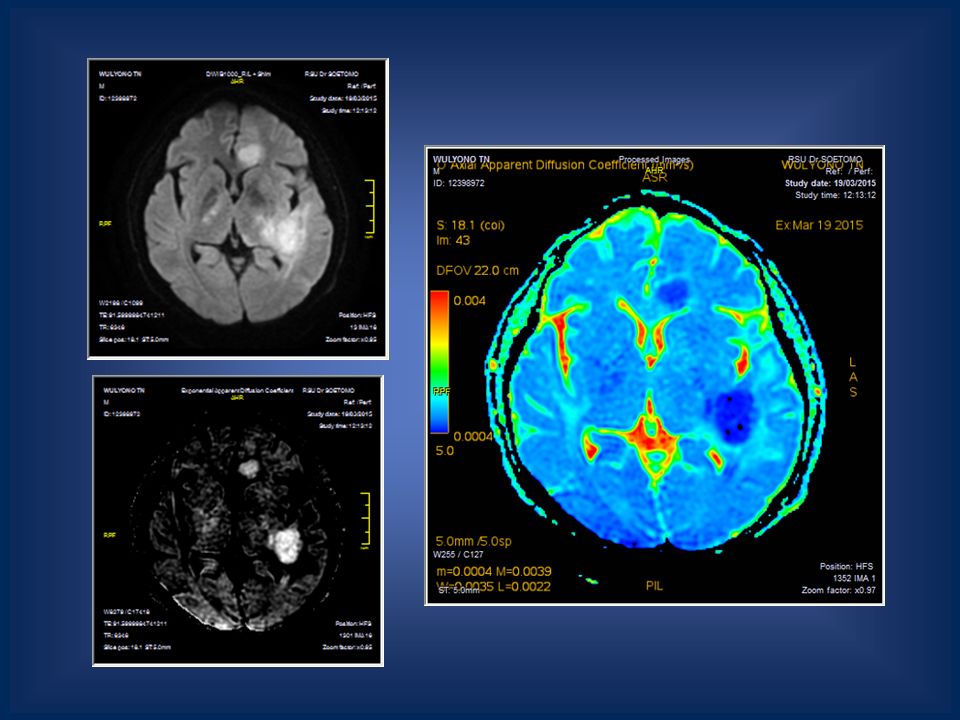
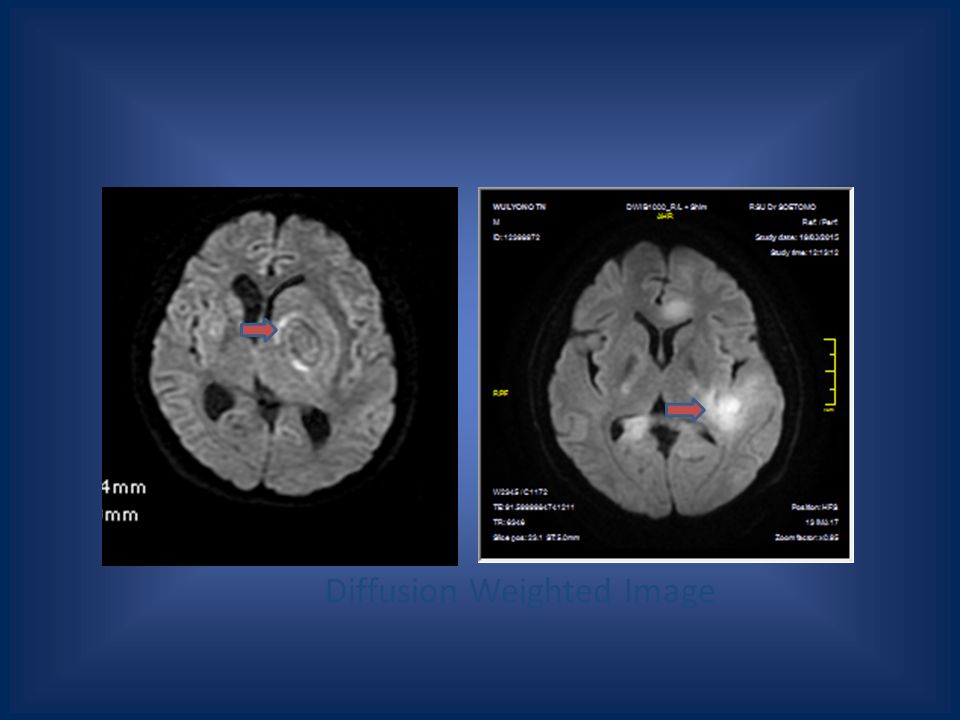
Diffusion Weighted Image

72
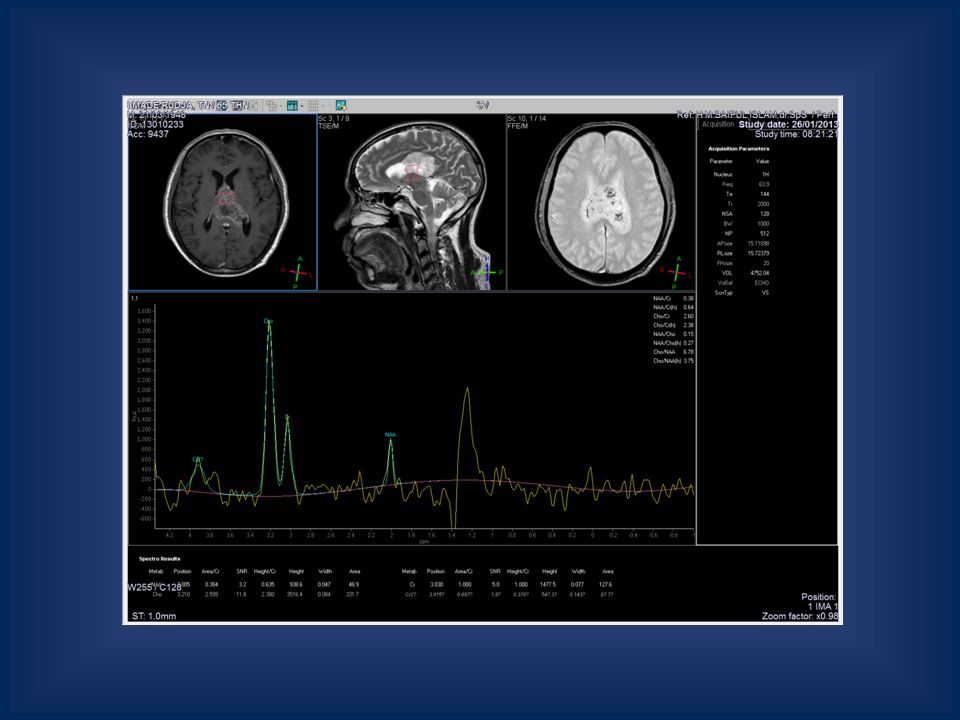
MR Spectroscopy

75
The Peritumoral region (PTR) demonstrated most significant differences in metabolite ratios. The Cho/Cr ratio in glioblastomas was significantly higher than that in metastases. PCLs significantly elevated Cho/Cr levels were also noted in compared with those in metastases. PCLs also demonstrated significantly higher lipids+lactate/Cr levels compared with glioblastomas and metastases. Proton magnetic resonance spectroscopy in differentiating glioblastomas from primary cerebral lymphomas and brain metastases. Chawla S Chawla S 1, Zhang Y, Wang S, Chaudhary S, Chou C, O'Rourke DM, Vossough A, Melhem ER, Poptani H.Zhang YWang SChaudhary SChou CO'Rourke DMVossough AMelhem ERPoptani H

76
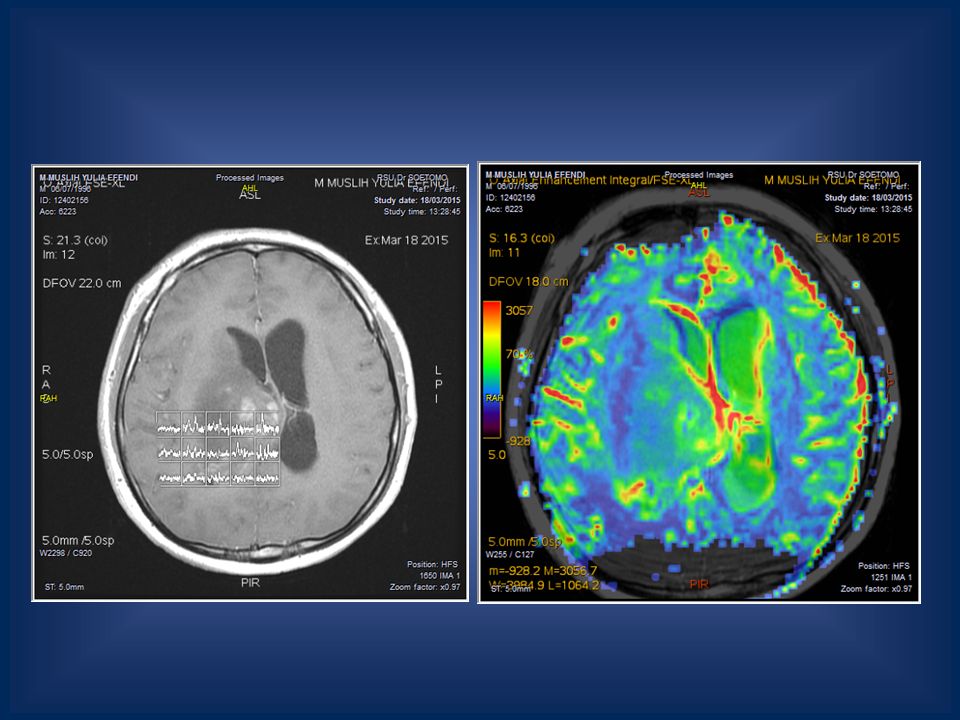
MR Perfusion

79
Take home message 1.CT Scan plays in emergency cases and some abnormality (blood, calcification, hemorrhage) 2.MRI play a better role than CT in differentiate infection, primary and metastatic tumor 3.MR imaging has the most potential of any imaging technique to allow a complete and accurate diagnosis and initial management strategy to be formulated for a brain tumor 4.Advanced imaging help enhancing the specifity of the lesions
 2.MRI play a better role than CT in differentiate infection, primary and metastatic tumor 3.MR imaging has the most potential of any imaging technique to allow a complete and accurate diagnosis and initial management strategy to be formulated for a brain tumor 4.Advanced imaging help enhancing the specifity of the lesions")
80
Thank You

Similar presentations