Download presentation
Presentation is loading. Please wait.

1
A Practical Guide to Prescribing on Day 1! Dr. Liz Gamble
DRUGS FOR TAKE A Practical Guide to Prescribing on Day 1! Dr. Liz Gamble

2
OBJECTIVES Identify sections of the drug chart
Prescribing abbreviations When not to prescribe Use of the BNF Use of hospital protocols Prescribe common / emergency Rx

3
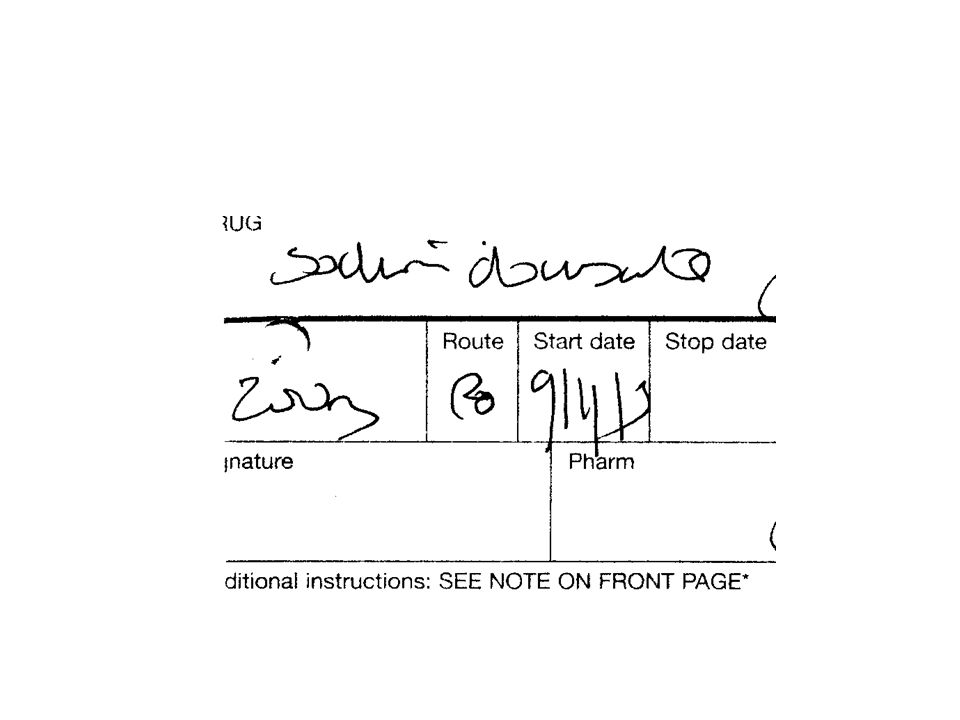
THE DRUG CHART FRONT Patient details Allergies Once only medication
Drug doses omitted

4
THE DRUG CHART MIDDLE Regular medication BACK As required medication

5
ABBREVIATIONS Route of administration Timing

6
How not to prescribe…..

8
WHEN NOT TO PRESCRIBE Prescribing is not the answer
You need to do something else first You could do more harm than good You feel it is not appropriate

9
USE THE BNF & HOSPITAL PROTOCOLS
Useful things in the BNF Hospital protocols

10
Oxygen; general principles
Aims to relieve hypoxia & maintain or restore a normal PaCO2 Deliver a defined percentage according to patients needs Hudson mask or nasal cannulae give very variable FiO2 Nasal cannulae become less efficient at flow rates > 3l/min

11
Hudson mask: variable performance

12
Nasal cannulae

13
Oxygen delivery devices

14
Venturi devices: fixed performance

15
Monitoring oxygen therapy
Use oximetry +/- arterial blood gases SaO2 of 93% is approximately equivalent to a PaO2 of 8kPa, below a SaO2 of 92% PaO2 falls rapidly Oximetry gives no information about PaCO2 or pH

16
General rules Correct hypoxia with an appropriate delivery device
Check ABGs if SaO2 <93% or suspicion of ventilatory impairment or acidosis Some patients (esp. COPD) with chronic hypoxia rely on hypoxic drive and will hypoventilate on high flow O2 If hypoxia suddenly occurs check cylinder, tubing etc.
 with chronic hypoxia rely on hypoxic drive and will hypoventilate on high flow O2. If hypoxia suddenly occurs check cylinder, tubing etc.")
17
Acute Severe Asthma Priorities Treat hypoxia
Treat bronchospasm & inflammation Assess need for intensive care Treat any underlying cause e.g. infection, pneumothorax

18
Acute Severe Asthma: therapy
Sit the patient up High flow oxygen Nebulized beta 2 agonists: salbutamol 5mg every min if required Add ipratropium bromide 500mcg 4-6hrly if initial response poor Steroids: hydrocortisone 200mg IV Antibiotics if evidence of infection

19
Severe asthma: iv bronchodilators
Magnesium sulphate: 1.2-2g iv over 20 mins Salbutamol: 5-20 mcg/min infusion Aminophylline: loading dose 250 mg iv over 20 mins, then mg/kg/hr infusion

20
Indications for ITU admission
Hypoxia: PaO2 <8kPa despite FiO2 of 60% Rising PaCO2 or PaCO2 >6 Exhaustion, drowsiness or coma Respiratory arrest Failure to improve despite adequate therapy

21
Sepsis Body’s response to an infection
Infection is the invasion of the body by microorganisms – can be local or widespread Worldwide 1400 people die every day from sepsis – projected to grow by 1.5% per year Three forms of sepsis: uncomplicated sepsis severe spesis septic shock

22
Sepsis Severe sepsis – sepsis with failure of one or more of the vital organs. Mortality from severe sepsis 30-50% Septic shock – sepsis with hypotension that does not respond to fluid administration Mortality from septic shock 50-60% Majority of sources of infection in severe sepsis/shock are pneumonia and intraabdominal

23
Surviving Sepsis Campaign
In 2004 an international group of critical care and infectious disease physicians developed guidelines for the management of severe sepsis and septic shock Society of Critical Care Medicine, European Society of Intensive Care, International Sepsis Forum Introduction of the sepsis care bundle

24
Care Bundle A group of interventions related to a disease process that result in better outcomes when executed together rather than individually 2 bundles – sepsis resuscitation bundle (6h) sepsis management bundle (24h)
 sepsis management bundle (24h)")
25
Sepsis Resuscitation Bundle
1) Measure serum lactate 2) Obtain blood culture prior to antibiotics 3) Broadspectrum antibiotics within 3h of presentation 4) In the event of hypotension or lactate > 4 mmol/L Deliver an initial minimum of 20ml/kg of crystalloid Apply vasopressors for hypotension not responding to initial fluid resuscitation to maintain MAP > 65 mm Hg
 Measure serum lactate. 2) Obtain blood culture prior to antibiotics. 3) Broadspectrum antibiotics within 3h of presentation. 4) In the event of hypotension or lactate > 4 mmol/L. Deliver an initial minimum of 20ml/kg of crystalloid. Apply vasopressors for hypotension not responding to initial fluid resuscitation to maintain MAP > 65 mm Hg.")
26
Sepsis resuscitation bundle
5) In the event of persistent hypotension despite fluid resuscitation (septic shock) or lactate > 4 mmol/L Achieve CVP > 8 mm Hg Achieve central venous oxygen saturation (ScvO2)> 70%
 In the event of persistent hypotension despite fluid resuscitation (septic shock) or lactate > 4 mmol/L. Achieve CVP > 8 mm Hg. Achieve central venous oxygen saturation (ScvO2)> 70%")
27
What can we do in MAU? Make prompt diagnosis Measure lactate
Blood cultures Antibiotics within 3 hours Fluid challenge ITU review early Central line, try to get CVP>8mm Hg Glucose control

28
Community acquired pneumonia
Non-severe: amoxycillin 500mg tds + clarithromycin 500mg bd. Penicillin allergic: moxifloxacin 400mg bd Severe: Co-amoxiclav 1.2g iv tds + clarithromycin 500mg bd. Penicillin allergic: levofloxacin 500mg iv bd

29
Acute alcohol withdrawal
Symptoms: anxiety, tremor, hyperactivity, sweating, nausea, tachycardia, hypertension, mild pyrexia. Seizures may occur Delirium tremens (untreated mortality 15%): course tremor, agitation, confusion, delusion, hallucinations Look for hypoglycaemia, Wernicke-Korsakoff, subdural haematoma, hepatic encephalopathy
: course tremor, agitation, confusion, delusion, hallucinations. Look for hypoglycaemia, Wernicke-Korsakoff, subdural haematoma, hepatic encephalopathy.")
30
General Management Rehydrate (avoid saline in liver disease)
IV pabrinex 2 pairs 8hourly Oral therapy: thiamine 100mg bd, vit B co strong 2 tabs tds, vit C 50mg bd Monitor glucose Check phosphate; give iv if <0.6mM Exclude infection

31
Sedation Chlordiazepoxide 30mg qds for 2 days
Then 20mg daily (divided doses) for 2 days Then 10mg daily (divided doses) for 2 days Then 5mg daily for 2 days For fits lorazepam 1-2mg iv
 for 2 days. Then 10mg daily (divided doses) for 2 days. Then 5mg daily for 2 days. For fits lorazepam 1-2mg iv.")
32
Acute coronary syndrome
Symptoms resulting from myocardial ischaemia STEMI / NSTEMI / unstable angina Need continuous ECG monitoring and defibrillation facilities IV access

33
General measures Aspirin 300mg stat Oxygen Diamorphine 2.5-10mg prn
Metaclopramide 10mg iv GTN spray 2 puffs sl (unless low bp) FBC, U&Es, glucose, lipids, TnI
 FBC, U&Es, glucose, lipids, TnI.")
34
Other measures Patients with STEMI: urgent reperfusion (thrombolysis or PCI) Patients with NSTEMI: clopidogrel 300mg stat then 75mg od, enoxaparin 1mg/kg bd Cardiology input Correct K+ Treat arrhythmias, cardiac failure

35
TACKLING PAIN Regular analgesia Regular paracetamol
Regular co-codamol 30:500 NSAIDS Morphine Other pains

36
SIMPLE REMEDIES FOR MINOR PROBLEMS
Nausea Constipation Cough Indigestion Leg cramps Insomnia Agitation

37
JUGGLING BLOOD SUGARS Highs and lows Type 1 or Type 2?
Adjusting insulin doses Sliding scales

38
SCARY SITUATIONS What if you get there first? Additional management
OSCEs Doses IV or IM?

39
SCARY SITUATIONS Respiratory depression & pinpoint pupils
Severe heart failure Myocardial infarction Severe asthma Hypoglycaemia Possible meningococcal disease Anaphylactic shock Status epilepticus

40
SUMMARY The drug chart Prescribing abbreviations When not to prescribe
The BNF Hospital protocols Simple remedies for minor problems Common emergencies

Similar presentations
>")






 for severe sepsis and septic shock treatment>")











