Download presentation
Presentation is loading. Please wait.

1
Chapter 20 OXYGENATION (97 slides)
NURSING FUNDAMENTALS Chapter 20 OXYGENATION (97 slides)
")
2
Picture of Normal Lungs

3
Oxygen Measures 21% in the earth’s atmosphere
Oxygen is essential to sustain life Each of the millions of cells in the human body uses oxygen to metabolize nutrients and produce energy Without oxygen, cell death occurs rapidly, a human cannot live more than a few minutes without O2

4
Human respiration is subdivided into 3 stages:
1. External respiration 2. Internal respiration 3. Cellular respiration or oxidation

5
External Respiration Also known as breathing or ventilation
This consists of breathing in (inspiration) and breathing out (expiration)
 and breathing out (expiration)")
6
Ventilation Movement of air in and out of the lungs

7
Inspiration When the elasticity of lung tissue allows the lungs to stretch and fill with air when breathing in As air is inhaled, warmed, moistened, it is filtered on its passage into the air sacs of the lungs known as alveoli

8
Alveoli Alveoli are the air cells or sacs of the lung
Once this 1st process occurs, the concentration of oxygen in the alveoli is greater than in the bloodstream because it has all of the inhaled O2 in it O2 diffuses from an area of greater concentration like in the alveoli, to an area of lesser concentration, like that of the bloodstream…then it goes into RBCs on the hemoglobin protein to be carried to all parts of the body (this is external respiration)
")
9
Now the reverse happens…
When the O2 is breathed in and travels to the alveoli and then to the hemoglobin of the RBCs, carbon dioxide in the bloodstream becomes high and diffuses into the alveoli (the O2 and CO2 trade places) we then expel the CO2 off along with some water vapor out into the air as we exhale (this is internal respiration) The amount of O2 breathed in dictates how much CO2 we will blow off
 we then expel the CO2 off along with some water vapor out into the air as we exhale (this is internal respiration) The amount of O2 breathed in dictates how much CO2 we will blow off.")
10
Cellular respiration Involves the use of O2 to release energy stored in nutrients Remember how O2 is needed for oxidation of food during digestion, we get the O2 from breathing it in, it helps create the energy we need throughout our body Cellular respiration is a chemical reaction that occurs within the cells when they receive O2, energy is able to be given off

11
What makes us breathe For people without disease to the lungs, increased blood levels of carbon dioxide and hydrogen ions triggers the stimulus to breathe This means that when we “suck” in O2, it transfers to carbon dioxide and hydrogen ions, our body uses the O2 for many things and we blow off the CO2…THIS inhaling of O2 that produced CO2 stimulates us to breathe out

12
Ventilation Ventilation occurs from pressure changes within the thoracic cavity produced by contraction and relaxation of respiratory muscles

13
During Inspiration The dome-shaped diaphragm contracts and moves downward in the thorax The intercostal muscles move the chest outward by elevating the ribs and sternum This combination expands the thoracic cavity. We need this expansion so air can fill up into the lungs

14
This expansion in the thoracic cavity…
Creates more chest space and causes the pressure within the lungs to fall below that in the atmosphere Because air flows from an area of higher pressure to lower pressure, air is pulled in through the nose, and fills the lungs

15
If there is an acute need for oxygen…
Your accessory muscles (sternocleidomastoid in the neck, and pectoralis minor), contract to assist with even greater chest expansion This activity however, can only go on for so long before the person tires out
, contract to assist with even greater chest expansion. This activity however, can only go on for so long before the person tires out.")
16
During expiration The respiratory muscles relax
The thoracic cavity decreases The stretched elastic lung tissue recoils Intrathoracic pressure increases as a result of the compressed pulmonary space and air moves out of the respiratory tract

17
Assessing Oxygenation
Several measures can determine the quality of one’s oxygenation status: Physical assessment data objective info. Such as: Arterial blood gas Pulse oximetry Skin and nail bed color And by subjective information such as the pt telling you he is S.O.B.

18
Hypoxemia Decreased oxygen in the arterial blood
Pt’s get agitated, restless and become cyanotic and have a seizure

19
Hypoxia An oxygen deficiency
A decreased concentration of oxygen in the inspired air

20
What do nurses monitor in physical assessment
Respiratory rate Breathing pattern and effort Chest symmetry Auscultation of lung sounds Color of skin, lips and nail beds Heart Rate and blood pressure Level of consciousness

21
Arterial Blood Gases Known as ABG
This test is drawn from blood that is in an artery…ouchie…deep needle stick It assesses oxygenation, ventilation and acid-base balance It measures the partial pressure of oxygen dissolved in plasma (PaO2), the percentage of HGB saturated with oxygen (SaO2) and the partial pressure of carbon dioxide in plasma (PaO2) in plasma, the ph of blood, and the level of bicarbonate ions in the blood
, the percentage of HGB saturated with oxygen (SaO2) and the partial pressure of carbon dioxide in plasma (PaO2) in plasma, the ph of blood, and the level of bicarbonate ions in the blood.")
22
Why not just perform a venous blood gas from a vein?
Arterial blood is preferred for sampling because arteries have greater oxygen content that do veins and are responsible for carrying oxygen to all cells

23
Who obtains this ABG Floor nurses DO NOT Phlebotomy Doctors
Respiratory therapists Usually do. ICU nurses may do this. Blood is usually obtained from the radial site in the wrist

25
Normal Lab Values of an ABG
Ph : – <7.35 – acidosis > alkalosis PaO2: mm Hg mm hg-mild hypoxemia 40-60mm hg- moderate hypoxemia PaCO2: mm Hg <35 mm hg – hyperventilation > 45 mm hg – hypoventilation SaO2: % <95% - hypoventilation HCO3: meq <22 or >26 – compensation for acid base balance

26
HGB Respiratory therapists have a saying:
They say that HGB has 4 seats for O2 for every HGB molecule. Therefore, 4 O2 molecules can sit on 1 HGB, when a person has all 4 seats full of O2, the person’s pulse ox is 100%

27
Pulse Oximetry Noninvasive, transcutaneous technique
Uses a band aid type or clip on type device with an infra-red light that penetrates through to detect the amount of light absorbed by hemoglobin. We tell our patients that the light detects the amount of O2 in the tissue You will see a reading in a percent form We like to see one’s pulse ox >95%, this is a person without lung disease of any type

29
Promoting Oxygenation
Many factors affect ventilation but there is something nurses CAN do to increase ventilation: Positioning is #1 thing that nurses can do

30
Positioning Fowler’s Position – an upright seated position
This position eases breathing by allowing the abdominal organs to descend away from the diaphragm, now the lungs have the potential to fill with a greater volume of air

31
Variation of Fowler’s position
Orthopneic position – this is a seated position with the arms supported on pillows or the arm rests of a chair, and the client leans forward over the bedside table or a chair back. The orthopneic position allows room for maximum vertical and lateral chest expansion and provides comfort while resting or sleeping

33
Breathing Techniques Deep Breathing Pursed-lip breathing
Diaphragmatic breathing The use of nasal strips

34
Deep Breathing Taking in a large volume of air that fills the alveoli to a greater capacity and improves gas exchange This maximizes ventilation Deep breathing is effective for people who tend to breathe shallowly or those who are inactive

35
How to encourage deep breathing more often
We can teach pts about use of the incentive spirometer to get them to breathe more deeply If a pt can deep breathe alone, without the use of a spirometer, then they will benefit from this. Others cannot perform this well without the device

36
Incentive Spirometer The use of a calibrated device that encourages clients to reach a goal-directed volume of inspired air I.S. has calibrated marks on the side that the patient can use to reach his goal The goal of I.S. is to inhale, expanding the lungs while holding it for 3-6 seconds before releasing the air (exhaling)
")
37
Using the I.S. The pt sits up if possible, he takes a normal breath in and then exhales He then inserts the mouth piece and seals his lips around it He inhales slowly and deeply, removes the mouth piece, and holds it for 3-6 seconds He then exhales slowly This should be performed 10xs Q hr W.A.

38
Pursed-Lip Breathing Is a form of controlled ventilation in which the pt consciously prolongs the expiration phase of breathing This helps the pt to eliminate more than the usual amount of carbon dioxide from the lungs

39
Pursed-Lip Breathing The pt inhales slowly through the nose while counting to three He then purses the lips as though whistling The abdominal muscles then contract He then exhales through pursed lips for a count of 6 or more Laboring mothers do this between contractions

40
Diaphragmatic Breathing
This type of breathing promotes the use of the diaphragm rather than the upper chest muscles It is used to increase the volume of air exchanged during expiration, used to try and decrease CO2 levels caught in the lungs as in COPD This type of breathing reduces respiratory effort and relieves rapid, ineffective breathing

41
How to use diaphragmatic breathing
Pt lays down with knees slightly bent Place one hand on abdomen and one on the chest Inhale slowly with pursed lips and deeply through the nose while letting the abd. Rise more than the chest Contract the abd. Muscles and begin to exhale Press inward and upward with the hand on the abd. While continuing to exhale

42
Nasal Strips These are adhesive strips that are applies to the bridge of the nose to reduce airflow resistance by widening the breathing passageways of the nose These have been successful in relieving snoring as well

43
Oxygen Therapy When positioning and breathing techniques are inadequate and the pulse ox remains below 95%, oxygen therapy is necessary

44
Oxygen Therapy Is an intervention for administering more oxygen than present in the atmosphere to prevent or relive hypoxemia

45
Oxygen equipment needed for O2 therapy
An oxygen source A flowmeter An oxygen humidifier An oxygen delivery device

46
Oxygen Source O2 is supplied from one of 4 sources: 1. Wall outlet
2. Portable tank 3. Liquid oxygen unit 4. Oxygen concentrator

47
Wall Outlet Oxygen is supplied through a wall outlet in every pt’s room The outlet is connected to a large reservoir filled with O2 on a routine basis

48
Portable Tank O2 is contained in portable tanks resembling steel cylinders that hold various volumes under extreme pressure A large tank of O2 contains 2,000 lbs of pressure per square inch The tanks are delivered with a protective cap to prevent accidental force against the tank outlet

49
Use of a new tank When attempting to use a new tank, it must be “cracked” which is a technique for clearing the outlet of dust and debris. This is done by turning the tank valve slightly to allow a brief release of pressurized oxygen. This force causes a loud, hissing noise which may be frightening Always crack the tank away from the pt’s bedside

51
Danger If a tank has been cracked and any accidental force has been applied to the outlet, it could cause the tank to take off like a rocket with disastrous results

52
Liquid Oxygen Unit It’s a device that converts cooled liquid oxygen to a gas by passing it through heated coils Pts at home use these, they are lightweight, portable units that allow greater mobility inside and outside the house Each unit holds 4-8hrs of O2 Problems include: liquid O2 is more expensive, unit may leak in warm weather and frozen moisture may occlude the outlet

53
Oxygen Concentrator Is a large machine that collects and concentrates oxygen from room air and stores it for client use The air from the room is compressed and mixed with a chemical called zeolyte. It removes the nitrogen from the air, leaves pure O2 which is stored in a 2nd chamber and releases the nitrogen back into the air

54
Oxygen concentrator This type of device eliminates the need for a central reservoir or piped O2 This type of O2 is used in home health care and long-term care facilities This type of O2 is also good if there is a power failure, a pt can still receive O2

55
Equipment Used in Oxygen Administration
Flowmeter Oxygen Analyzer Humidifier

56
Flowmeter Is a gauge used to regulate the amount of O2 delivered to the client and is attached to the oxygen source It measures the O2 in liters per minute It is regulated by turning the dial until the indicator is directly beside the indicated amount to be delivered

57
Oxygen Analyzer Is a device that measures the % of
delivered O2 to determine if the client is receiving the amount prescribed by the Physician This device is a box with a cord and a sensor at the end of the tip. The R.T. holds the tip in the air to detect room air is 21%, then it checks what the pt’s O2 device is reading at. If it is not what the Dr. ordered, the R.T. adjusts the flowmeter to give the pt what was ordered This device is used in isolettes of newborns, in croup tents and in pts who are on a vent

58
Humidifier Is a device that produces small
water droplets and may be used during Oxygen administration because O2 is drying to the mucous membranes When more than 4 liters is administered or O2 is administered for a long period of time, humidification is applied

59
Humidified O2 Humidification is performed by attaching or screwing on a bottle of pre-filled distilled water to the flowmeter. You use a green Christmas tree/triangular piece This water filters into the O2 as it is delivered or evaporates and the container will empty. R.T. or nurses must check this frequently

60
Common Delivery Devices
Nasal Cannula Masks Face tents Tracheostomy collars T-Piece Nasal Catheter Oxygen Tent C-Pap/Bi-pap Transtracheal Oxygen

61
Nasal Cannula A hollow tube made of ½ inch
prongs that are placed downward in the nostrils The cannula is held in place by wrapping the tubing around the ears and adjusting the slide clamp under the chin like a cowboy hat Nasal cannulas are used for pts receiving 2 Liters or less of O2 usually for short periods of time

62
Masks Several types of masks are available: Simple Mask
Partial re-breather Mask Non-re-breather Mask Venturi Mask

63
Simple Mask Fits over the nose and mouth
Allows atmospheric air to enter and exit through side ports An elastic strap holds it in place Allows for higher levels of O2 better than the cannula Works well for mouth breathers Must deliver a minimum of 5 liters/min

65
Problems with simple face masks
Seal around edges can break, causes O2 to leak and not be delivered well to the pt Can make the pt feel as though he is suffocating Can cause skin breakdown around edges Pt can’t eat or talk well with this mask on Straws can be stuck through the side hole for sipping

66
Partial re-breather Mask
This mask has a reservoir bag at the bottom of the face mask that can be filled with O2 by pressing the valve located under the mask This mask allows a mixture of atmospheric air, O2 from its source and O2 contained within the reservoir to be delivered to the pt No humidification can be added to this bag

67
Partial re-breather Mask
This mask uses 6-10 liters of O2/min The pt breathes in controlled O2, exhales, and 1/3 of the exhaled air goes back into the bag and the other 2/3 goes out of the side holes. This means that all of the exhaled air leaves the mask, some enters the bag but most of it exits through the holes No humidification can be added to this mask

68
Non re-breather mask This mask causes ALL of the exhaled air to leave the mask rather than partially re-entering the reservoir bag like the partial re-breather This mask is designed to deliver % O2 This mask contains one-way valves that allow ONLY O2 from its source as well as O2 in the reservoir bag to be inhaled, no air from the atmosphere is inhaled. All air exhaled leaves through the mask and does not enter the reservoir bag These pts who wear this mask require high levels of O2, they are usually critically ill

70
Patients with any mask All pts with masks need to be checked, especially ones wearing non re-breathers and re-breather masks The reservoir bags MUST ALWAYS BE FULL…this keeps most or all of the CO2 out of the bag so the pt won’t re-breath it

71
Venturi Mask This mask mixes a precise amount of O2 and atmospheric air Also called a Venti mask This mask has a large ringed tube coming from it Color-coded adapters extend off the ringed tube and can be changes according to the amount of room air and O2 needed This color-coded system ensures that the Venti-mask delivers the exact amount of prescribed O2 Humidification can be added to these masks

72
Venti-mask

73
Face Tent Provides O2 to the nose and the mouth at the same
time without the use of a mask Pts feel less claustrophobic The only problem with this O2 delivering device is that due to its openness, it may not deliver the exact amount of O2 ordered d/t environmental losses

74
Tracheostomy collar Delivers O2 near an artificial opening in the neck
This is applied over a trach which is an opening into the trachea through which a client breathes Because there is no passage of air into the nose, warming and moisturizing of O2 is done via this collar with humidification A trach. must have a DSD applied around the outer piece that sticks out and this dressing becomes moist and needs to be changed frequently

75
T-Piece This piece fits securely onto a tracheostomy tube
It is similar to a trach collar but fits directly over the piece sticking out of the neck Again, the gauze around the trach collects moisture from the O2 blowing and it needs to be change frequently Problem: the weight of this connection may cause the trach to be pulled on causing the pt to cough and possibly can cause the trach to pop out

77
Nasal Catheter Also known as a nasal obturator
This slides into the nostril and goes to the posterior nasal pharynx This type is not used often d/t it being uncomfortable d/t irritation of the nasopharynx

78
Oxygen Tent A clear plastic enclosure that provides cooled, humidified O2 Mostly used in the care of infants and toddlers O2 concentrations are difficult to control with this device The edges of the tent must be tucked under the mattress to avoid air leaks Also, one must keep tent closed so O2 doesn’t escape An O2 analyzer must be used to check levels in the tent

79
O2 Tent

80
Snoring or collapsing of airway
Pts who snore inhale then collapse their airway upon expiration and then the next inhalation is insufficient O2 is not able to get in and overtime, loss of O2 can cause the heart to get enlarged which may leads to cardiac arrest and death Sleep apnea MUST be dealt with

81
C-pap Continuous positive air pressure This maintains a (+)
pressure within the airway throughout the respiratory cycle It keeps the alveoli partially inflated even during expiration The face mask is attached to a portable ventilator The noise of this machine can keep others awake If there is a problem with the machine, it alarms

82
C-pap Is also worn at night for sleep apneic patients
The residual oxygen within the alveoli continues to diffuse into the blood during apneic episodes that may last 10 seconds or more

83
Bi-pap Allows for 2 pressures to be set, inspiration and expiration pressure Bi-pap is used when C-pap fails

84
Transtracheal Oxygen A hollow tube is inserted within the trachea to deliver oxygen This device is less noticeable than a nasal cannula but is much more invasive. The pt is oxygenated with lower flows of O2 Surgery is required to place a stent to create an opening and it remains there until the wound heals and a channel is formed An inner cannula remains and the pt must care for this properly

85
Oxygen Hazards There are always potential hazards with the use of O2:
Fire Potential Oxygen Toxicity

86
Fire Potential O2 itself does not burn It is combustible therefore,
It is necessary to control all possible sources of open flames or ungrounded electricity

87
O2 Safety Use of signs like “Oxygen in use”
Prohibit the burning of candles during religious rituals rites Check to see that electrical equipment has 3 prong plugs so they are properly grounded Inspect wires for frays or loose wires Avoid using petroleum, aerosol, and acetone products where O2 is used. These are ignitable substances, we don’t want to ignite them and then the O2

88
Oxygen Toxicity This is when lung damage develops after oxygen concentrations of more than 50% are administered for longer than hours It is believed that O2 given at this rate reduces the surfactant (a lipoprotein produced by cells in the alveoli that promotes elasticity of the lungs and enhances gas diffusion

89
Related Oxygen Techniques
The use of a chest tube The use of a hyperbaric O2 chamber

90
Chest Tube A technique for evacuating air or blood from the pleural cavity which helps to restore negative intrapleural pressure and re-inflate the lung A thick tube is placed from the outside of the body into the pleural space by surgical application, drainage and air drain by suction or gravity into a container. When all of the air or fluid is removed, the tube is pulled out

91
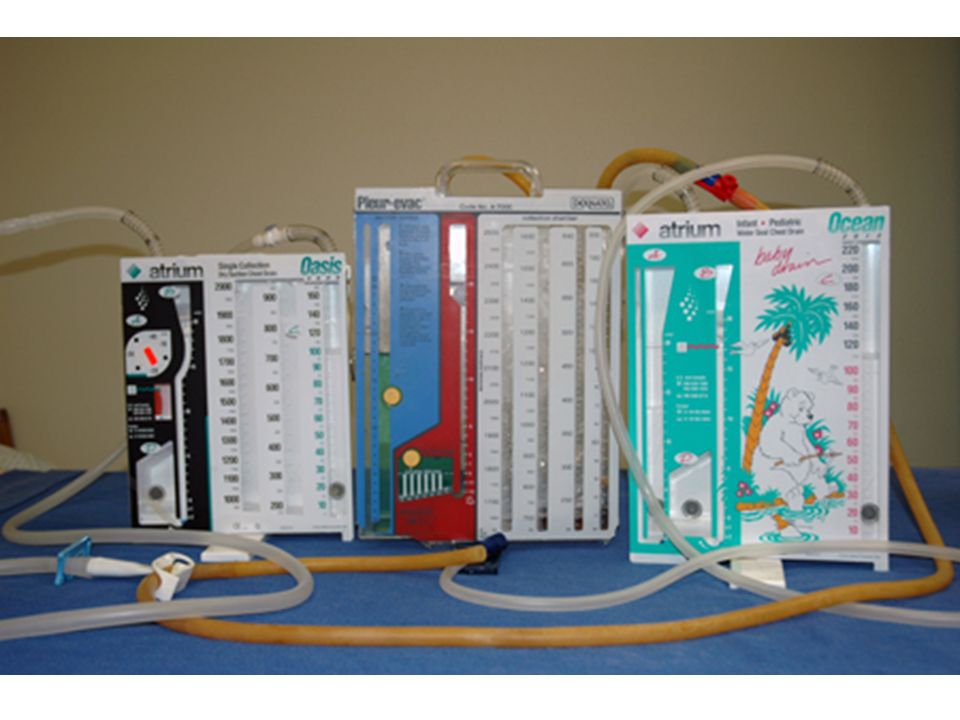
Chest tubes usually have 3 chambers
Chamber #1 – collects blood or acts as an exit route for pleural air Chamber #2 – holds water that prevents atmospheric air from re-entering the pleural space, this is called the “water seal” Chamber #3 – if used, facilitates the use of suction which may speed the evacuation of blood or air

93
Hyperbaric Oxygen Therapy
Consists of delivery of 100% O2 at three times the normal atmospheric pressure within an airtight chamber These treatments last approximately 90 minutes and are repeated over days, weeks or months of therapy

94
Providing pressurized oxygen increases the oxygenation of blood plasma from a normal level of mm hg to more than 2,000 mm hg Providing brief periods of breathing room air helps to prevent O2 toxicity

95
Purpose of hyperbaric O2 therapy
Regenerates new tissue at a faster rate, it’s most popular for promoting wound healing It’s other uses are to treat carbon monoxide poisoning, gangrene associated with Diabetes or other vascular insufficiency, and decompression sickness experienced by deep-sea divers

96
NANDA Diagnoses Ineffective Breathing Pattern Impaired Gas Exchange
Anxiety Risk for Injury (related to oxygen hazards)
")
97
The End

Similar presentations