Download presentation
Presentation is loading. Please wait.

1
Management of the Neonatal Airway Based upon American Academy for Pediatrics (AAP) Guidelines Presented by: Michael R. Jackson RRT-NPS CPFT & the NRP Instructors* of the NICU Respiratory Care Service * AAP Certified Instructors of the Newborn Resuscitation Program

3
32 weeks & under

4
Oral airway Used for: Micrognathia (pictured here) Pierre Robin Choanal atresia airway may cause gagging
 Pierre Robin Choanal atresia airway may cause gagging")
5
Oral airway Predict size measure from ear to corner of mouth Placed right side up in the oropharynx (no need to rotate into place as with adult oral airways) Choanal Atresia
 Choanal Atresia")
7
Lesson 3: Insertion of Orogastric Tube Measuring correct length © 2000 AAP/AHA

8
Pressure/Volume ratlung http://www.brighamandwomens.org/respiratorytherapy/Images/ratlung.swf

10
Nasopharangeal Tube for CPAP Nasal tubes more easily secured in position than oral tube Are associated with nasopharangeal irritation, swelling, mucous plugging Greater movement in airway with head motion than oral tubes Require greater (~1cm) insertion depth than oral tube
 insertion depth than oral tube")
11
Nasotracheal Tube for Ventilation Nasal tubes more easily secured in position than oral tube Are associated with nasopharangeal irritation, swelling, mucous plugging Greater movement in airway with head motion than oral tubes Require greater (~1cm) insertion depth than oral tube
 insertion depth than oral tube")
13
DuoDerm Nare protection from CPAP prongs Nasal seal for CPAP prongs

14
Leone TA, Rich W, Finer NN, Neonatal Intubation Success of Pediatric Trainees, J Pediatr 2005;146:638-641 Preferred number of experiences to achieve competency is 45. Opportunities have diminished since we stopped intubating active meconium babies. Rates of Intubation Success

15
AAP Newborn Resuscitation: Endotracheal Intubation Indications l Meconium present and baby is not vigorous l Prolonged positive-pressure ventilation required l Bag-and-mask ventilation ineffective l Chest compressions necessary l Epinephrine administration necessary l Special indications: prematurity, surfactant administration, diaphragmatic hernia © 2000 AAP/AHA

16
ETTUBEETTUBE

17
Neck mass by ultrasound During EXIT* procedure *ex utero intrapartum treatment

20
Surfactant & Tube position

21
90 degree ETT to airway entrance Blue line of ETT superior

22
Equipment and Supplies l Equipment should be clean, protected from contamination. Wear gloves l Sterile disposable endotracheal tubes with uniform diameters preferred. Size is based on gestational age. l Stylette is optional © 2000 AAP/AHA ETT Size Wt. Gest. (mm) (kg) (wks) (mm) (kg) (wks) 2.5 < 1 <28 2.5 < 1 <28 3.0 1 – 2 28-34 3.0 1 – 2 28-34 3.5 2 - 3 34-38 3.5 2 - 3 34-38
 (kg) (wks) (mm) (kg) (wks) 2.5 < 1 < < 1 < – –")
23
Lesson 5: Preparation of Laryngoscope: Supplies Select blade size –No 0 for preterm newborns –No 1 for term newborns l Check laryngoscope light l Connect suction source to 100 mm Hg l Use large suction catheter (greater than or equal to 10F) for secretions l Small suction catheter for ET tube © 2000 AAP/AHA
 for secretions l Small suction catheter for ET tube © 2000 AAP/AHA")
24
Anatomic Landmarks © 2000 AAP/AHA Flash intubation http://www.brighamandwomens.org/respiratorytherapy/Images/intube.swf

25
Positioning the Newborn Prepare for Intubation © 2000 AAP/AHA l Prepare resuscitation bag and mask l Turn on oxygen l Get stethoscope l Cut tape or prepare endotracheal tube stabilizer Flash intubation http://www.brighamandwomens.org/respiratorytherapy/Images/intube.swf

26
Lesson 5: Endotracheal Intubation Step 1: Preparation for Insertion l Stabilize head l Provide free-flow oxygen © 2000 AAP/AHA

27
Lesson 5: Endotracheal Intubation: Holding the Laryngoscope © 2000 AAP/AHA

28
Lesson 5: Endotracheal Intubation Step 2: Insert Laryngoscope l Slide blade over right side of tongue l Push tongue to left side of mouth l Advance blade tip to vallecula © 2000 AAP/AHA

29
Lesson 5: Endotracheal Intubation Step 3: Lift Blade l Lift blade up & away l keep handle @ 60 degrees to baby’s chest l Visualize pharyngeal area l Do not use rocking motion © 2000 AAP/AHA 60

30
Visualize Landmarks l Vocal cords appear as vertical strips or as inverted letter “V” l Downward pressure on cricoid may help bring glottis into view l May need to suction secretions © 2000 AAP/AHA

31
Pass tube from right side of mouth (not down blade – which would obstruct view) Hold tube in right hand Insert until cord guide is at cords Wait for cords to open l Limit attempt to 20 seconds
 Hold tube in right hand Insert until cord guide is at cords Wait for cords to open l Limit attempt to 20 seconds")
32
Tube Location in Trachea © 2000 AAP/AHA

33
Remove Laryngoscope l Use a finger to hold the tube against the hard palate l Remove laryngoscope (and stylet, if used) © 2000 AAP/AHA
 © 2000 AAP/AHA")
34
Signs of correct tube position l Chest rise with each breath l Breath sounds over both lung fields l No gastric distention with ventilation l Vapor condensing on inside of tube during exhalation l Carbon dioxide detector will change color (or reads more than 2%-3% during exhalation)
")
35
Depth of insertion Weight (kg)(cm from upper lip).506.756.5 1*7 28 39 410 Predicted Tube Location in Trachea Tip-to-lip measurement © 2000 AAP/AHA
(cm from upper lip) * Predicted Tube Location in Trachea Tip-to-lip measurement © 2000 AAP/AHA")
36
The fulcrum for movement of this lever arm is the upper cervical spine. Fulcrum for movement of this lever arm is the upper cervical spine.. 5 5.5 8.3 10 Vocal Cord Vocal Cord Epiglottis Thy. Cartilage Epiglottis FLEXION NEUTRAL EXTENSION

39
ETCO2 display On/off Respiratory Rate Display 1 Place sensor & turn unit on. Place sensor & turn unit on. (unit will self-test) Confirm position by · CO2 value (ideally > 20) · CO2 waveform on monitor
 Confirm position by · CO2 value (ideally > 20) · CO2 waveform on monitor.")
41
Figure 1. Sensitivity = 94%, Specificity = 98%, P P Value = 98%, N P Value = 94% _ _ _ False positive (tube in esophagus) technical error. False negative (tube in trachea CO2 reading low) severe bronchospasm, hyperventilation, technical error, huge leak around ett, cardiopulmonary arrest.
 technical error. False negative (tube in trachea CO2 reading low) severe bronchospasm, hyperventilation, technical error, huge leak around ett, cardiopulmonary arrest..")
42
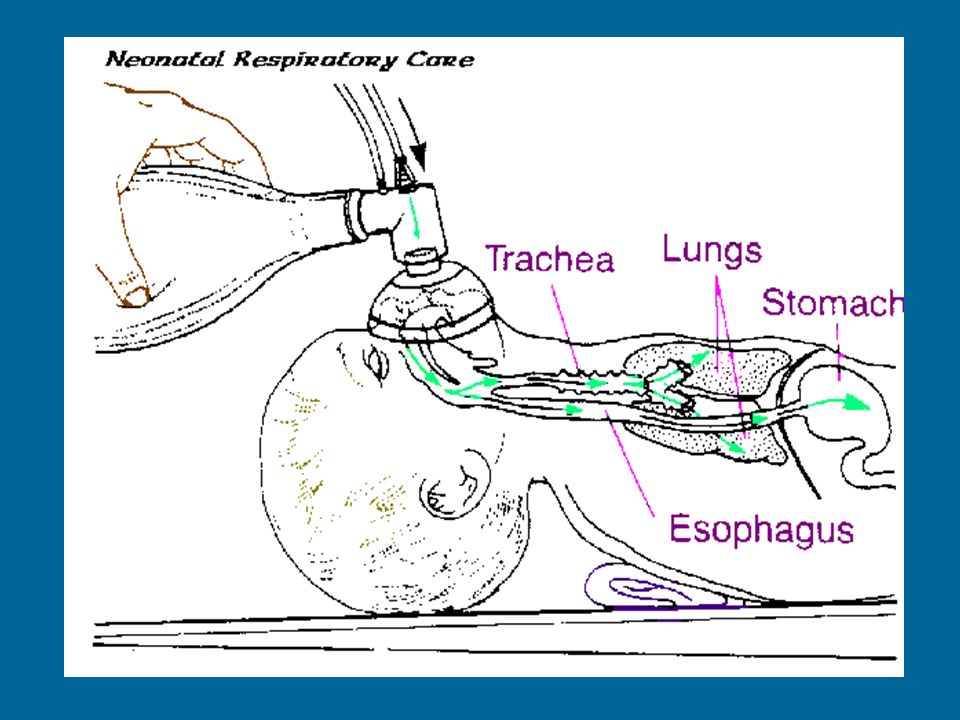
Where is the tube?

43
esophageal intubation

44
Every few years, another BPD baby requires a trach at Brigham & Women’s Hospital.

45
Bivona 3.0 TTS Custom FlexTend cuff Water port Pilot balloon stylette Airway connect

46
Suction at least a few mm past the length of trach tube –pre- measure distance to suction Trach Suction Trach Feeding Assess ability of patient to coordinate suck, swallow & breathe Test swallowing ability ~ 5 days after tracheostomy- (maybe earlier)
")
47
Changing a trach tube Humidification Remove stitches On new trach tube Remove tracheostomy tube Insert new tube same size Monitor # of “noses”used per day Check if patient is aspirating saliva Frequent coughing may be a clue

Similar presentations