Download presentation
Presentation is loading. Please wait.

1
Particulate and Lung Disease David Brown Sc.D. EHHI How should the Public Health system work with uncertain but plausible health hazards?

2
Can We Assume That Compliance With Federal Clean Air Standards Protects Against Short Term Health Impacts? Standards are set by expert committees There are safety factors built in standards Standards must have a bright line for attainment Compliance is monitored

4
DIESEL PARTICLE PM 2.5 RANGE WATER ADSORBED IRRITANT GAS ABSORBED IN WATER Irritant gases Deep lung exposure to irritants How particles increase exposure of irritants to the deep lungs

5
Results from the Harvard Six-cities study: All Cause Mortality Rates most exposed to least exposed City Fine Particles All cause death 1.26 (1.08-1.47) Lung Cancer 1.37 (0.81-2.31) Cardio pulmonary 1.37 (1.11-1.68) Other causes 1.01 (0.79-1.30) Range of exposure 11-29.6 ug/m3 Dockery, NEJM 1993; 329: 1753-1759
 Lung Cancer 1.37 ( ) Cardio pulmonary 1.37 ( ) Other causes 1.01 ( ) Range of exposure ug/m3 Dockery, NEJM 1993; 329:")
6
Health actions from exposures of 2 hours or less. Peters etal. pm 2.5 & myocardial infarction –1.48 odds ratio 2 hr after 25ug/m3 increase –1.69 odds ratio 1 day after 20ug/m3 increase Gent etal. Severe asthma & O3, pm 2.5 –35% increase wheeze 1 hr after 50ppb O 3 inc. –47% increase in chest tightness 1 hr after. –1.24 odds ratio Chest tightness 12-18ug/m3 pm

7
Moral stewardship in search of an intellectual framework. Theories of Deontology and Utilitarianism 1) Value of an act is found within the act. 2) The value of an act is found in the outcome. Four ideas 1600-1700: Bacon…..A new science Newton…Reductionism a new approach Kant…….The whole is more than the sum of the parts Bentham….Charity- science serves the needs of men.
 Value of an act is found within the act. 2) The value of an act is found in the outcome. Four ideas : Bacon…..A new science Newton…Reductionism a new approach Kant…….The whole is more than the sum of the parts Bentham….Charity- science serves the needs of men..")
8
Uncertainty paradox of Good Science in Public Health Science- Assume something is not true until proven at a level of statistical certainty. –Preferred action is to collect more data Public Health- Assume something may be true based on suggestive but statistically inconclusive evidence – Preferred action is to intervene to prevent potential health effect.

9
Result of application of Good Science is loss of time, lives and treasure Smoking Dioxin Asbestos Chordane Mercury Particulate Asthma at the end of the 20 th century

10
Health events that occur to students and teachers in schools Accidents Colds, flu and headaches Asthmatic attacks/ treatment Others Could any of these be environmental?

11
Health events are rarely linked with environmental exposures Most health events have multiple causes Only a small part of the group responds The exposures are not known sufficiently Investigations are complex and data is sparse The cause of the effect is other than environmental but there may be an environmental role

12
But there are environmentally induced diseases and responses Some are related to molds and other factors in buildings Some have been found to be related to 6 to 12 pollutants found in outside air Two agents, Ozone and PM, are linked to short term asthmatic and cardiac responses How do we respond to these agents ?

13
It is necessary to understand the following The Health Effects that are related to air quality Pollutant sources Movement of air into and within the school Ways to reduce the potential for exposures

14
Bad Air Quality Ozone Particulate Matter Nitrogen Dioxide Sulfur Dioxide Hazardous Air Pollutants (Toxins) Lead Carbon Monoxide
 Lead Carbon Monoxide")
15
Ozone Adverse effects following low-concentration exposure: –chest pains, –coughing, –nausea, –throat irritation, and –congestion. It also can worsen bronchitis, heart disease, emphysema, and asthma, and reduce lung capacity.

16
Studies conducted in the northeastern United States and Canada that show that ozone air pollution may be associated with 10-20 percent of all of the summertime respiratory-related hospital admissions. US Environmental Protection Agency, Criteria Document in support of proposed 8-hour ozone standard

17
Particulate Matter Premature death; Respiratory related hospital admissions and emergency room visits; Aggravated asthma; Acute respiratory symptoms; Chronic bronchitis; Decreased lung function; and Work and school absences.

18
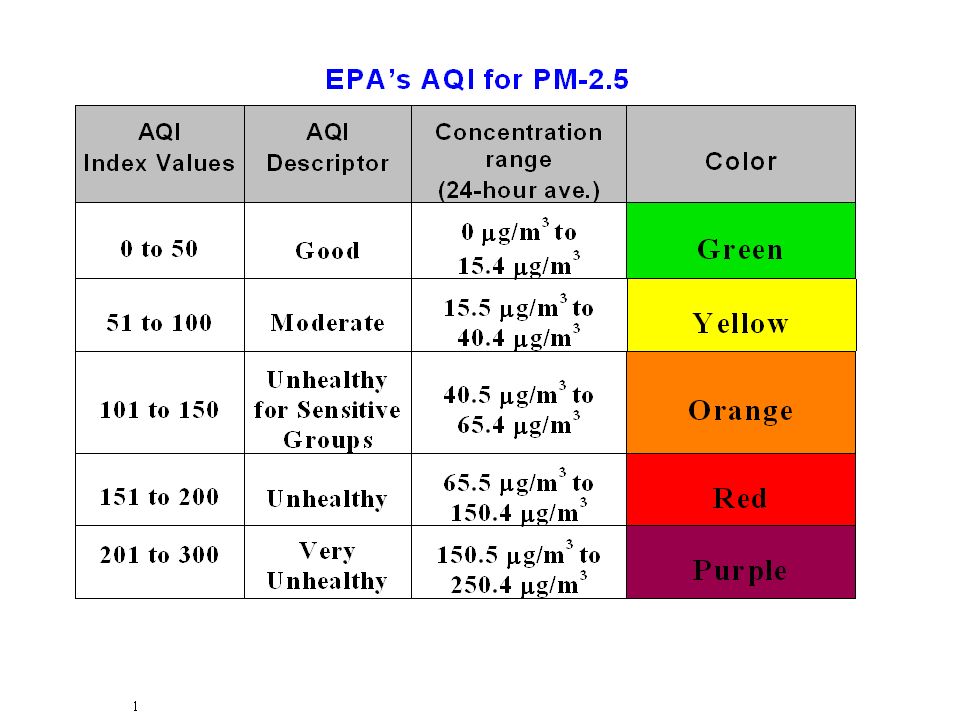
Particulate Matter EPA has revised the primary (health-based) PM standards by adding a new annual PM 2.5 standard set at 15 micrograms per cubic meter (µg/m 3 ) and a new 24-hour PM 2.5 standard set at 65 µg/m 3. EPA is retaining the current annual PM 10 standard of 50 µg/m 3 and adjusting the PM 10 24-hour standard of 150 µg/m 3 by changing the form of the standard.

20
What does this mean? Air exposures induce plausible health risks from short term elevation during regulatory attainment of clean air standards. Science should be brought to the legal decision making. Investigation of the quantitative health risk from localized short term air exposures is needed.

21
Question: How to use existing information to assess environmental exposures? Attainment model approach Evoked response model approach Statistical analyses –Expected spatial distributions –Expected temporal distributions –S plus approach –Cluster analysis –Edge theory analysis

22
As part of the process to determine whether an area meets the EPA particulate matter standard, this 3-month long series of hourly observations would be collapsed to a single value… 9.2 ug/m 3 … Totally obscuring any structure or other content within the data set (Carmine Dibattista, CT DEP).
.")
24
PM 2.5 New Haven, Hartford and Waterbury (ug/m3)
")
25
Fine particles, or haze, restrict our ability to see long distances Hartford Oct. 8, 2002 4 p.m. EDT Unadjusted Hourly conc. of fine particles – 4 g/m 3 Hartford Oct. 2, 2002 4 p.m. EDT Unadjusted Hourly conc. of fine particles – 24 g/m 3

26
33 Air Toxics in Connecticut

27
Consider the different sources of toxics in outdoor air separately Transport from other regions –Fossil fuel and ozone Transport from the within the region –Utilities, fossil fuel and transportation Local sources such traffic and area sources –Transportation, off road commercial Immediate sources near the buildings –Vehicles diesel, pesticides and construction

28
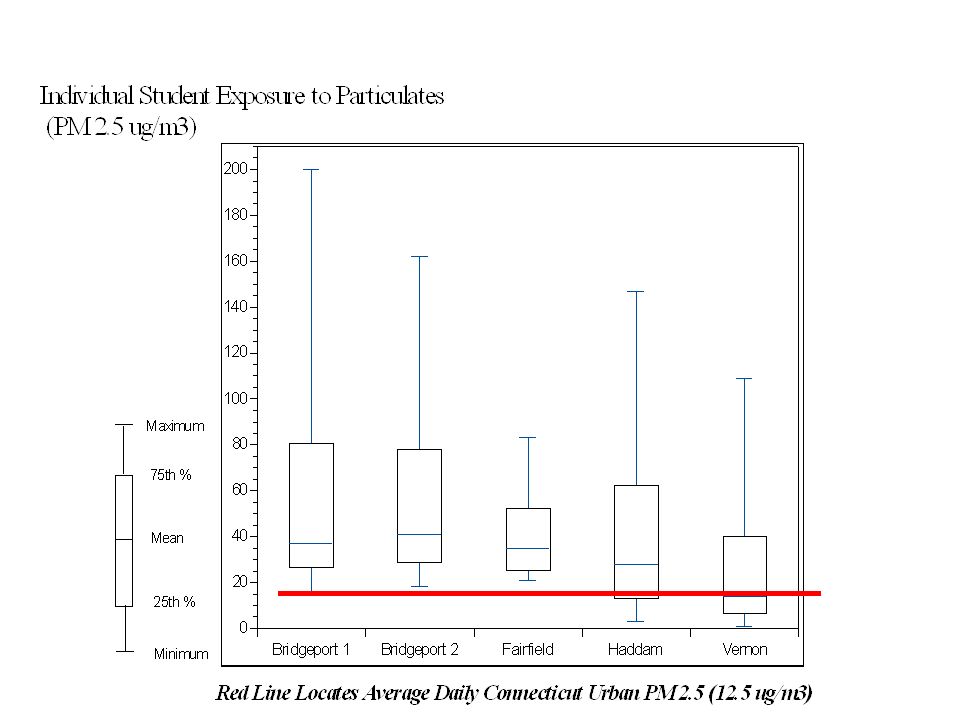
School child exposure, continuous nephelometer 15 minute averages

29
School child exposure, continuous nephelometer

30
School Child Exposure Continuous Nephelometer

32
Comparing ambient pm with School and Buses

33
Compare Bus to School and Ambient monitor for PM.

34
Difference in amount of exposure between times of day

35
Actual inhaled dose varies between day, time of day, activity and location for child

36
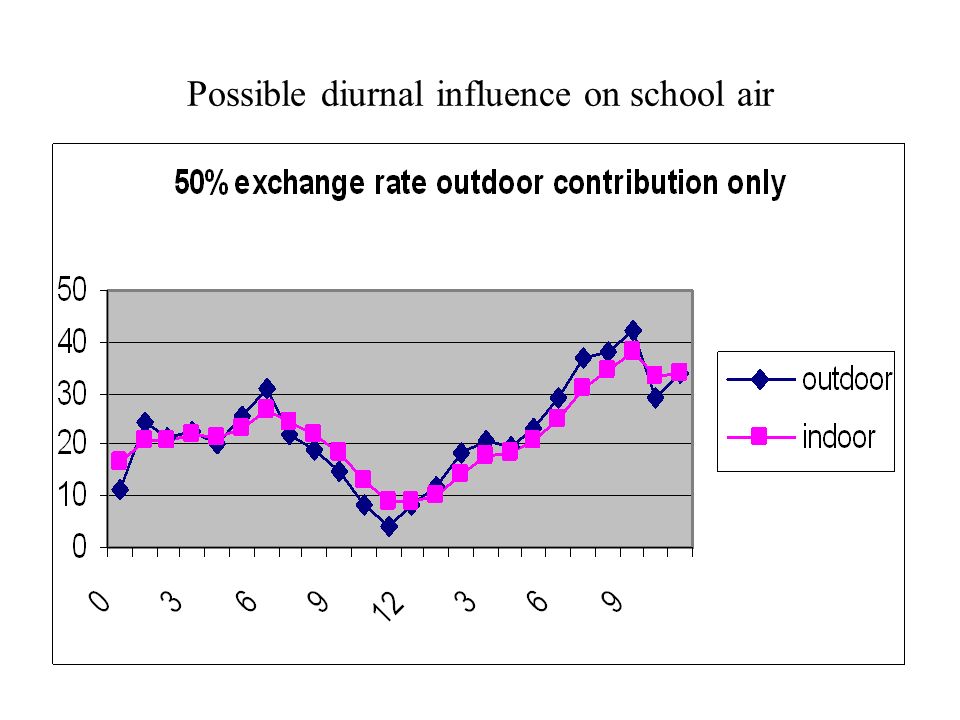
One half the volume in each hour One half the volume out each hour School Buildings have memories of outside exposures A 400 ppm diesel particulate emission from a bus that idles for one hour next to the school exposes the students for over 3 hours

37
Possible diurnal influence on school air

39
Analyzing fine PM data by comparing 3-hr exposure distributions to daily and annual averages reveals significant underestimation of potential health risk. Comparison of PM 2.5 24-hr avg and 3-hr max avg for New Haven CT site, 2001

40
Effect of morning decrease in local wind- speed and mixing volume during sun rise

42
Local air quality events that are seen inside the school Buses idling Morning traffic Commercial vehicles Construction Sun rising and sun setting Nocturnal Jet Sun rising and sun setting Changes in the weather Pesticide applications

43
Information from existing data Vt. monitoring data shows 11 compounds drive most of risk. Using CEP and NATA, EPA characterized types of risk and sources at county levels. Multi-city studies determine level of health risks from PM and ozone nationally. Levy shows local and regional risk from two power plants.

44
Fine Particulates PM 2.5 Spatial Distribution in NE Current monitoring network analyses average away PM 2.5 variability. Are spatial and temporal factors (local sources, unique terrain, meteorology) influencing concentrations and creating PM gradients? If so, micro-scale exposure assessments must be refined. May reveal downward bias of health effects estimates: are missing populations at risk?
 influencing concentrations and creating PM gradients. If so, micro-scale exposure assessments must be refined. May reveal downward bias of health effects estimates: are missing populations at risk .")
45
Lessons learned or hints Short term local exposures are disproportionate, 5 to 15% of days in NE. Sources of variability are: –Location –Season –Time of day –Sources –Meteorology, weather patterns in NE

46
Six ways to reduce the potential for exposures Identify sources near the building Restrict emissions during periods of poor air mixing Reduce idling of engines during the 3 hours prior to student occupancy of building Increase make up air during clean periods Prevent stagnation of air within the school Adjust student activities

47
Conclusions A more robust reporting statistic is needed in addition to attainment levels. The weather variable is discontinuous existing in 4 forms in the NE. National analyses do not characterized NE risk. Averaging time is critical for understanding health risk Health outcome should drive the risk analysis

Similar presentations


















. Can be “good” up.>")



