Download presentation
Presentation is loading. Please wait.

2
Spore-forming gram-positive bacilli Bacillus (Aerobic) B. antheracis, B.cereus, B. subtilis Clostridum (Anaerobic) C. tetani, C. botulinum, C. perfringens, C. difficile
 C. tetani, C. botulinum, C. perfringens, C. difficile.")
3
Bacillus anthracis

4
Disease Anthrax (common in animal but rare in humans). The anthrax bacillus, Bacillus anthracis, was the first bacterium shown to be the cause of a disease.

5
History (Recent years) 1991 - About 150,000 U.S. troops were vaccinated for anthrax in preparation for Persian Gulf War. 2001 - Letters containing anthrax spores were mailed to many places in the US such as NBC, New York Times, and Media in Miami. 1876 - German bacteriologist Robert Koch confirmed bacterial origin of anthrax. 1945 - In Iran an anthrax outbreak killed more than 1 million sheep.

6
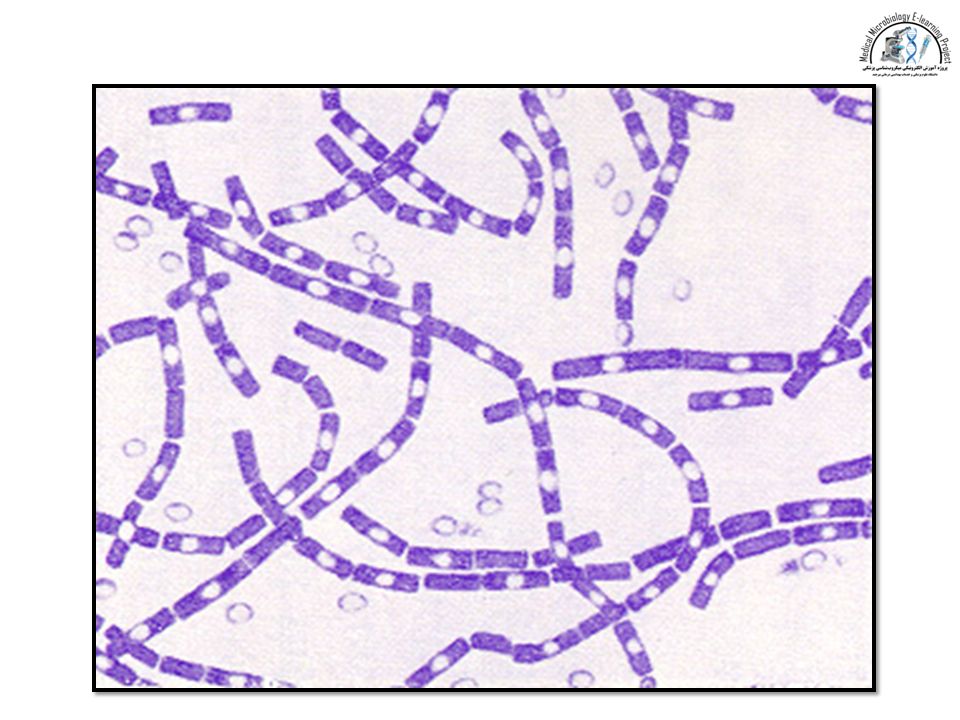
Properties 1 - 1.2µm in width x 3 - 5µm in length Gram + rod Facultative anaerobe A large rod with square ends. Frequently in chains

7
Properties A unique anti-phagocytic capsule is composed of D-glutamate (Glutamyl-polypeptide capsule) Non-motile (other members of the genus are motile. Forms oval, centrally located endospores Head medusa, rough, gray colonies Inhalation Anthrax (2)
.")
8
Gram stain. The cells have characteristic squared ends. The spores are highly refractile to light and resistant to staining. Bacillus cereus

10
Robert Koch's original micrographs of the anthrax bacillus

15
Genetics 1 chromosome 5.2 million bp Ames strain sequenced 2 plasmids px01 184 kbp Exotoxin pX02 95.3 kbp Capsule

16
Anthrax From the Greek word anthrakos for coal Caused by spores Primarily a disease of domesticated & wild animals Herbivores such as sheep, cows, horses, goats Natural reservoir is soil Does not depend on an animal reservoir making it hard to eradicate Cannot be regularly cultivated from soils where there is an absence of endemic anthrax Anthrax zones Soil rich in organic matter (pH < 6.0)
")
17
Transmission May be spread by streams, insects, wild animals, birds, contaminated wastes Animals infected by soilborn spores in food & water or bites from certain insects Humans can be infected when in contact with flesh, bones, hair, & excrement Risk of natural infection Outbreaks occur in endemic areas after outbreaks in livestock

18
Transmission Spores persist in soil for years. Infection from animal products (hides, bristles and wool), contact with sick animal. Portals of entry: skin, mucous membranes, and respiratory tract.
, contact with sick animal. Portals of entry: skin, mucous membranes, and respiratory tract..")
20
Three forms of Anthrax Cutaneous anthrax Skin Most common Spores enter to skin through small lesions Inhalation anthrax Spores are inhaled The most lethal type of Anthrax. Gastrointestinal (GI) anthrax Spores are ingested Oral-pharyngeal and abdominal
 anthrax Spores are ingested Oral-pharyngeal and abdominal.")
21
Pathogenesis The infectious dose of B. anthracis in humans: Minimum infection dose of ~ 1,000-8,000 spores LD 50 of 8,000-10,000 spores for inhalation Virulence depends on 2 factors: Capsule (Invasiveness, not protective antigen) Exotoxin
 Exotoxin.")
22
Capsule Sticky, gelatinous polymer pX02 plasmid Made up of D-glutamic acid Non-toxic on its own Only encapsulated B. anthracis is virulent Most important role during establishment of disease Protects against phagocytosis & lysis during vegetative state

23
Exotoxin pX01 plasmid AB model: Binding & Activating 3 components: Protective antigen (PA), edema factor (EF), lethal factor (LF) Make up 50% of proteins in the organism EF: An adenylate cyclase Components are individually non-toxic LF+PA lethal EF+PA edema EF+LF inactive PA+LF+EF edema & necrosis; lethal
, edema factor (EF), lethal factor (LF) Make up 50% of proteins in the organism EF: An adenylate cyclase Components are individually non-toxic LF+PA lethal EF+PA edema EF+LF inactive PA+LF+EF edema & necrosis; lethal")
24
Cutaneous Anthrax 95% of anthrax infections occur when the bacterium enters a cut or scratch on the skin due to handling of contaminated animal products or infected animals. May also be spread by biting insects that have fed on infected hosts. After the spore germinates in skin tissues, toxin production initially results in itchy bump that develops into a vesicle and then painless black ulcer.

25
Cutaneous Anthrax A painless ulcer with black, necrotic eschar. Local edema. usually 1-3 cm in diameter. Incubation period: Usually an immediate response up to 1 day Case fatality after 2 days of infection : Untreated (20%) With antimicrobial therapy (1%)
 With antimicrobial therapy (1%).")
29
Cutaneous Anthrax (3) CDC, Cutaneous Anthrax- Vesicle Development
 CDC, Cutaneous Anthrax- Vesicle Development")
30
Inhalation Anthrax Natural infection is extremely rare Spores need to be less than 5 microns (millions of a meter) to reach the alveolus. Macrophages lyse and destroy some of the spores. Survived spores are transported to lymph nodes.

31
The two lungs are separated by mediastinum: Heart, trachea, esophagus, blood vessels.

32
Inhalation Anthrax (2) Spores germinate and replicate in the lymph nodes. Exotoxins: mediastinal widening and pleural effusions (accumulation of fluid in the pleural space).
..")
33
Inhalation Anthrax (3) Death usually results 2-3 days after the onset of symptoms. Incubation period: 1–7 days Possibly ranging up to 42 days (depending on how many spores were inhaled). Case fatality after 2 days of infection: Untreated (97%) With antimicrobial therapy (75%)
. Case fatality after 2 days of infection: Untreated (97%) With antimicrobial therapy (75%).")
35
Gastrointestinal Anthrax GI anthrax may follow after the consumption of contaminated, poorly cooked meat. There are 2 different forms of GI anthrax: 1) Oral-pharyngeal 2) Abdominal Abdominal anthrax is more common than the oral- pharyngeal form.
 Oral-pharyngeal 2) Abdominal Abdominal anthrax is more common than the oral- pharyngeal form..")
36
GI Anthrax (2) Oral-pharyngeal form - results from the deposition and germination of spores in the upper gastrointestinal tract. Local lumphadenopathy (an infection of the lymph glands and lymph channels), edema, sepsis develop after an oral or esophageal ulcer. Abdominal form - develops from the deposition and germination of spores in the lower gastrointestinal tract, which results in a primary intestinal lesion. Symptoms such as abdominal pain and vomiting appear within a few days after ingestion.
, edema, sepsis develop after an oral or esophageal ulcer. Abdominal form - develops from the deposition and germination of spores in the lower gastrointestinal tract, which results in a primary intestinal lesion. Symptoms such as abdominal pain and vomiting appear within a few days after ingestion..")
37
This picture is 9 days after the onset of symptoms of oral-pharyngeal anthrax, an unusual manifestation of human infection with B. anthracis.

38
GI Infection (3) GI anthrax cases are uncommon. Incubation period: 1-7 days Case fatality at 2 days of infection: Untreated (25-60%) With antimicrobial therapy (undefined) due to the rarity
 With antimicrobial therapy (undefined) due to the rarity.")
39
The symptoms for Inhalation & Gastrointestinal anthrax There are two phases of symptoms. 1) Early phase - Many symptoms can occur within 7 days of infection 2) 2nd phase - Will hit hard, and usually occurs within 2 or 3 days after the early phase.
 Early phase - Many symptoms can occur within 7 days of infection 2) 2nd phase - Will hit hard, and usually occurs within 2 or 3 days after the early phase..")
40
Early Phase Symptoms Fever (temperature > 38 degrees celsius) Chills or night sweats Headache, cough, chest discomfort, sore throat Joint stiffness, joint pain, muscle aches Shortness of breath Enlarged lymph nodes, nausea, loss of appetite, abdominal distress, vomiting, diarrhea Meningitis
 Chills or night sweats Headache, cough, chest discomfort, sore throat Joint stiffness, joint pain, muscle aches Shortness of breath Enlarged lymph nodes, nausea, loss of appetite, abdominal distress, vomiting, diarrhea Meningitis")
41
2nd Phase Symptoms Breathing problems, pneumonia Shock Swollen lymph glands Cyanosis (skin turns blue) Profuse sweating Death
 Profuse sweating Death")
42
Lab. diagnosis Samples: Exudate, Blood, sputum. Direct smear: Large rods in chains. Spores not seen in smears of exudate. Culture and biological/biochemical tests (Sensitivity to penicillin (String of pearls test), Fermentation, gelatin hydrolysis, Motility) No serological tests are useful
, Fermentation, gelatin hydrolysis, Motility) No serological tests are useful.")
43
How is anthrax diagnosed? Gram stain Immunoflourescence staining Culture of B. anthracis from the blood, skin lesions, vesicular fluid, or respiratory secretions X-ray and Computed Tomography (CT) scan Rapid detection methods PCR for detection of nucleic acid ELISA assay for antigen detection
 scan Rapid detection methods PCR for detection of nucleic acid ELISA assay for antigen detection.")
44
Chest X-ray Useful for inhalation and GI anthrax Chest X-rays is advised as an initial method of inhalation anthrax detections. Find a widened mediastinum and pleural effusion. At day 1 At day 3

46
CT scan Useful for inhalation and GI anthrax Chest CT (Right) shows the increase in the size of the pleural effusions (accumulation of fluid in the pleural space).
 shows the increase in the size of the pleural effusions (accumulation of fluid in the pleural space).")
47
PCR Assay Used for the detection of anthrax toxin genes. rpo B gene - used as a specific chromosomal marker for RT-PCR detection. Provides 100% sensitivity and specificity

48
Distinguishing inhalation Anthrax from cold or influenza Anthrax, cold, and influenza patients have similar symptoms at early phase but Anthrax: No runny nose Breathing problems and more vomiting High white blood cell counts and no increase in the number of lymphocytes Inhalation anthrax has abnormality in X-ray or CT scan

49
Prevention Preventing soil contamination Sterilizing dead animals and animal products Protecting persons at risk of exposure with special clothes Vaccination with cell-free vaccine (PA) for persons at high risk and animals
 for persons at high risk and animals")
50
Who gets it? People working directly with it in the lab People working with imported animal hides or furs in areas where standards are insufficient to prevent exposure People handling potentially infected animal products in high-incidence areas Military personnel deployed to areas with high risk for exposure

51
Treatment Penicillin (Before 2001, 1st line of treatment was penicillin G but Stopped for fear of genetically engineered resistant strains) Doxycycline Ciprofloxacin (from fluoroquinolones)
 Doxycycline Ciprofloxacin (from fluoroquinolones)")
52
Weaponization & Bacillus Anthracis: Why is this Agent Considered to be the Department of Defense’s Number - One/Two Biological Threat?

53
Why are Biological Agents Attractive Weapons? (2) Silent, Unnoticeable Attacks Bombs & bullets are loud and there effects often dramatic and widely evident - not the case with BW BW can be tasteless, odorless, colorless and unnoticeable Allows for more facile attacks on large populations People could be inflicted and not immediately realize it - time lag
 Silent, Unnoticeable Attacks Bombs & bullets are loud and there effects often dramatic and widely evident - not the case with BW BW can be tasteless, odorless, colorless and unnoticeable Allows for more facile attacks on large populations People could be inflicted and not immediately realize it - time lag.")
54
Specific Benefits of Using Anthrax as a Biological Weapon Short Incubation Period (Relative to Most Other BW) Lag-time between attack and the first symptoms is only 1-6 days Prediction of intended effect is much more facile to estimate In contrast, bacterial agent brucellosis has an incubation of 5-60 days UV Resistant One of only two bacterial agents that is considered resistant to sunlight (the other being Coxiella)
 Lag-time between attack and the first symptoms is only 1-6 days Prediction of intended effect is much more facile to estimate In contrast, bacterial agent brucellosis has an incubation of 5-60 days UV Resistant One of only two bacterial agents that is considered resistant to sunlight (the other being Coxiella)")
55
How to Aerosolize?

56
Protection Against Anthrax Pre/Post Exposure Antibiotic Treatment Decontamination of Exposed Areas Using liquid chlorine dioxide or some other disinfectant Use of Protective Clothing & Equipment Gas masks provide good protection against 1-5 m particles Protective suits can be worn to easily eliminate cutaneous threat

57
Bacillus cereus Motile No capsule Saprophyte

58
Laboratory differentiation of Bacillus anthracis & B. cereus (phenethyl alcohol)
")
59
Bacillus cereus Disease Food poisoning Rare infections: Meningitis, Osteomyelitis, … Transmission Spores on grains survive during steaming and rapid frying. Spore germinated when rice is reheated. Portal of entry is the gastrointestinal tract.

60
Pathogenesis B. cereus produces 2 enterotoxins. Clinical findings 1.Emetic syndrome A short incubation period (4 hours) with nausea and vomiting similar to staphylococcal food poisoning. 2.Diarrheal syndrome Involves a long incubation period (18 hours) with diarrhea and resembles clostridial gastroenteritis.
 with nausea and vomiting similar to staphylococcal food poisoning. 2.Diarrheal syndrome Involves a long incubation period (18 hours) with diarrhea and resembles clostridial gastroenteritis..")
61
Lab. diagnosis Not usually doneTreatment No antibiotic is given. Only symptomatic treatmentPrevention Grains (specially rice) should not be reheated
 should not be reheated.")
Similar presentations












 USN Preventive Medicine Resident Johns Hopkins Bloomberg School of Public Health.>")







 Bacillus anthracis Early Symptoms/Signs Fever, Malaise, Fatigue, Chills, Myalgia Cough Delayed.>")

 Liz Schwabel Wildlife Diseases.>")

 Most are saprophytic contaminants or normal flora Bacillus.>")





>")