Download presentation
Presentation is loading. Please wait.

1
Weight Management: Overweight, Obesity, and Underweight Chapter 9

3
Overweight and Obesity Major health problem in the U.S. 66% of Adults 33% of Children Growing concern worldwide Prevalence especially high among women, poor, blacks, and Hispanics BMI of 25 or greater Epidemic is worldwide Not merely among industrialized countries

4
Overweight and Obesity BMI > 25

5
1993: Most states had prevalence rates less than 15 percent, with a couple reporting rates less than 10 percent; no state had prevalence rates greater than or equal to 20 percent. <10% 10%–14% 15%–19% Key: No Data 20%–24% 25%–29% ≥ 30% BMI > 25

6
<10% 10%–14% 15%–19% Key: 20%–24% 25%–29% ≥ 30% No Data 1998: Most states had prevalence rates less than 20 percent, with none reporting rates less than 10 percent; seven states had prevalence rates greater than or equal to 20 percent. BMI > 25

7
<10% 10%–14% 15%–19% Key: 20%–24% 25%–29% ≥ 30% No Data 2003: More than half the states had prevalence rates greater than 20 percent, with four states reporting prevalence rates greater than or equal to 25 percent. BMI > 25

8
<10% 10%–14% 15%–19% Key: 20%–24% 25%–29% ≥ 30% No Data 2008: Only one state had prevalence rates less than 20 percent; more than half the states had prevalence rates greater than 25 percent, with six states reporting prevalence rates greater than or equal to 30 percent. BMI > 25

9
Fat Cell Development Energy in exceeds energy out Body fat stored in cells of adipose tissue Number and size of fat cells Late childhood/early puberty fat cell numbers increase Fat deposited in organs- inflammation, insulin resistance Energy out exceeds energy in Fat cell size decreases; no change in number

10
Energy in > Energy out

11
During growth, fat cells increase in number. When energy intake exceeds expenditure, fat cells increase in size. When fat cells have enlarged and energy intake continues to exceed energy expenditure, fat cells increase in number again. With fat loss, the size of the fat cells shrinks but not the number. Stepped Art Fat Cell Development

12
Fat Cell Metabolism Lipoprotein lipase (LPL) stores triglycerides LPL activity in obese > than lean people Men- abdomen Women- breasts, hips, thighs Hormone-sensitive lipase (HSL) releases and breaks down triglycerides Weight regain: After wt. loss, LPL production increases. Fat oxidation is less efficient than fat storage.

13
Causes of Overweight & Obesity – Genetics & Epigenetics Causative role of genetics Genetic influences do seem to be involved Genetics may determine predisposition to obesity Genes interact with: Diet and physical activity Satiety and energy balance Human genome

14
Causes of Overweight & Obesity – Genetics & Epigenetics Obesity gene Codes for the protein leptin Acts as a hormone in hypothalamus Promotes negative energy balance Suppresses appetite Increases energy expenditure Locations of leptin secretion

15
With leptin treatment, this mouse lost a significant amount of weight but still weighs almost one and a half times as much as a normal mouse. Without leptin, this mouse weighs almost three times as much as a normal mouse.

16
Causes of Overweight & Obesity – Genetics & Epigenetics Obesity gene that codes for leptin- protein that suppresses appetite Genetic deficiency of leptin or genetic mutation- rare in obese people Leptin resistance Leptin rises with BMI, declines with dieting Roles in the body Energy regulation Immune system, RBC’s, female fat reserves

17
Causes of Overweight & Obesity – Genetics & Epigenetics Adiponectin Secreted by adipose tissue Inverse correlation with body fat Inhibits insulin resistance, inflammation, CHD Ghrelin Acts in hypothalamus, secreted by stomach Promotes positive energy balance Inverse correlation with body weight

18
Causes of Overweight & Obesity – Genetics & Epigenetics PYY GI cells secrete in proportion to kcalories consumed Signals satiety and decreases food intake Ideal diet Maintain satiating hormones-leptin, PYY, CCK Minimize appetite stimulating hormone ghrelin Low in fat and rich in fiber

19
Proteins Regulating Appetite and Energy Proteins Regulating Appetite and Energy

20
Causes of Overweight & Obesity – Genetics & Epigenetics Uncoupling proteins Proteins involved in energy metabolism Two types of fat White adipose tissue Brown adipose tissue Uncoupling proteins found in both types of fat Influence basal metabolic rate (BMR)
")
21
Causes of Overweight & Obesity – Environment Encountered daily circumstances Interaction between environment and genetics Overeating Present and past eating and activity patterns influence current body weight Availability Serving sizes Restaurant food

22
Selecting grapes with their high water content instead of raisins increases the volume and cuts the energy intake in half. Even at the same weight and similar serving sizes, the fiber-rich broccoli delivers twice the fiber of the potatoes for about one-fourth the energy. By selecting the water- packed tuna (on the right) instead of the oil- packed tuna (on the left), a person can enjoy the same amount for fewer kcalories.
 instead of the oil- packed tuna (on the left), a person can enjoy the same amount for fewer kcalories..")
24
Causes of Overweight & Obesity – Environment Physical inactivity Life requires little exertion Modern technology Inactivity contributes to weight gain and poor health Sedentary activities and weight gain DRI for prevention of weight gain 60 minutes of moderate activity every day

26
Problems of Overweight and Obesity – Health Risks Three indicators BMI Waist circumference Disease risk profile Factors taken into account Beneficial weight loss Health status Motivation

27
Problems of Overweight and Obesity – Health Risks Overweight but in good health motivation for weight loss Obese or overweight with risk factors Two or more risk factors Obese or overweight with life-threatening condition Recommendation to lose weight

28
Problems of Overweight and Obesity – Perceptions & Prejudices Most obese people do not successfully lose weight and maintain the loss Social consequences Jobs, school, and in social situations Psychological problems Embarrassment Other feelings

29
Fig. 9-6, p. 285

30
Problems of Overweight and Obesity – Weight Cycling

31
Problems of Overweight and Obesity – Popular Interventions Diet books and weight-loss programs Limited success with weight loss maintenance Fad diets- cabbage soup, shakes only Weight-loss products Meal replacements Herbal products No regulations for dietary supplements Liposuction

32
OTC

33
Drug Treatments for Obesity Strategies for weight reduction depend on: Degree of obesity Risk of disease Use drugs as part of long-term comprehensive weight-loss programs Assist with modest weight loss Four drugs approved by FDA for obesity

34
Drug Treatments for Obesity Sibutramine Suppresses appetite Side effects- dry mouth, rapid heart rate, etc Warning from FDA Orlistat Inhibits pancreatic lipase activity in GI tract Blocks dietary fat digestion and absorption Side effects- gas, frequent BM’s, decreased absorption of fat-sol. vitamins

35
Drug Treatments for Obesity Phentermine and diethylpropion Enhance release of neurotransmitter norepinephrine Mood high, appetite low Side effects- hyperactivity, insomnia Off-label use, “Stacking” Sudafed (pseudoephedrine) Claritin Benadryl
 Claritin Benadryl")
36
Diet Pills for sale online http://www.webmd.com/diet/guide/herbal- remedies http://www.webmd.com/diet/guide/herbal- remedies http://www.thedietadvisors.com/adipozin.ht ml http://www.thedietadvisors.com/adipozin.ht ml http://www.weightlossdietpills.com/?gclid=C JSlwpaCs6cCFQcBbAodkThW_w http://www.weightlossdietpills.com/?gclid=C JSlwpaCs6cCFQcBbAodkThW_w

37
How Appetite Suppressants Cause Weight Loss They are STIMULANTS (caffeine, ephedra, phentermine, chemicals that act like cocaine) Appetite suppressants promote weight loss by tricking the body into believing that it is not hungry or that stomach is full. They decrease appetite by increasing serotonin or catecholamine -- two brain chemicals that affect mood and appetite.

38
Prescription Weight Loss Drugs/Surgery Indications An option for the following individuals: People with a body mass index(BMI) of 30 and above with no obesity-related conditions. A person with a BMI of 27 and above with obesity-related conditions, such as diabetes or high blood pressure. http://www.webmd.com/diet/weight-loss- surgery/news/20110217/fda-oks-lap-band- surgery-for-more-patients http://www.webmd.com/diet/weight-loss- surgery/news/20110217/fda-oks-lap-band- surgery-for-more-patients

39
Surgical Treatments for Obesity http://www.lapband.com/en/home/ http://www.lapband.com/en/home/ http://www.webmd.com/diet/weight-loss- surgery/news/20110217/fda-oks-lap-band- surgery-for-more-patients http://www.webmd.com/diet/weight-loss- surgery/news/20110217/fda-oks-lap-band- surgery-for-more-patients Clinically severe obesity 200,000 surgeries performed each year Reduces food capacity of stomach Reduce production of ghrelin Health-related benefits Long-term safety and effectiveness

40
Surgical Treatments for Obesity

41
Esophagus Surgical staples Small stomach pouch Stomach Esophagus Duodenum Gastric band Jejunum StomachPort Large intestine In gastric bypass, the surgeon constructs a small stomach pouch and creates an outlet directly to the small intestine, bypassing most of the stomach, the entire duodenum, and some of the jejunum. (Dark areas highlight the flow of food through the GI tract; pale areas indicate bypassed sections.) In gastric banding, the surgeon uses a gastric band to reduce the opening from the esophagus to the stomach. The size of the opening can be adjusted by inflating or deflating the band by way of a port placed in the abdomen just beneath the skin. Small stomach pouch
 In gastric banding, the surgeon uses a gastric band to reduce the opening from the esophagus to the stomach. The size of the opening can be adjusted by inflating or deflating the band by way of a port placed in the abdomen just beneath the skin. Small stomach pouch.")
42
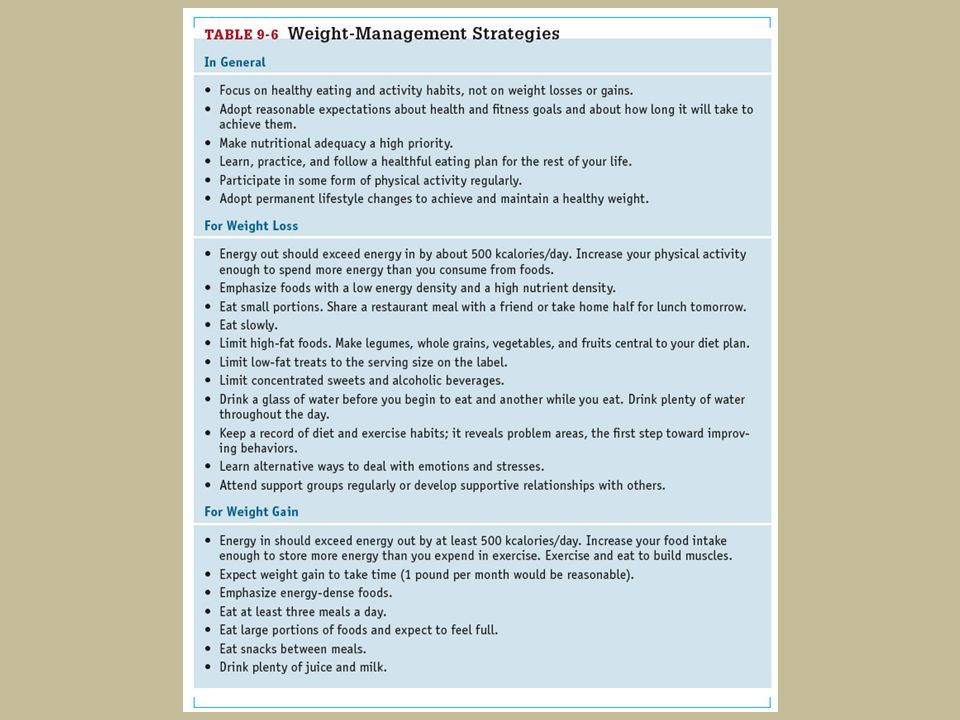
Weight Loss Strategies Successful strategies Find individual rate of change Moderate losses Reasonable short-term / long-term goal weight Reasonable rate of weight loss Benefits of modest weight loss Incorporate healthy eating and exercise

43
Weight Loss Strategies

44
Weight Loss Strategies – Eating Plans Be realistic about energy intake Must provide less energy than is needed Avoid restrictive eating Avoid rapid weight loss Goal: nutritional adequacy without excess Deficit of 500 to 1000 kcalories per day Breakfast frequency Inversely related to obesity

45
Weight Loss Strategies Eating Plans Nutritional adequacy minimum ~1200 kcal/d Eat small portions Eat less food at each meal Feel satisfied, not stuffed Structured meal replacement plans Lower energy density Mind control http://www.webmd.com/diet/default.htm http://www.webmd.com/diet/default.htm

46
Weight Loss Strategies – Eating Plans

47
Remember water Assistance with weight management Focus on fiber Low in energy and high in nutrients Require effort to eat Speed of food consumption Choose fats sensibly Energy density and satiation

48
Food Choices Slideshow http://www.webmd.com/diet/slideshow-fat- fighting-foods http://www.webmd.com/diet/slideshow-fat- fighting-foods

50
Weight Loss Strategies – Eating Plans Volumetrics Select carbohydrates carefully Artificial sweeteners Impact on energy intake Watch for empty/hidden kcalories Fat, sugar, and alcohol

51
Weight Loss Strategies Physical Activity Necessary for weight management Moderate physical activity plus activities of daily life Combination of diet and physical activity Lose more fat Retain more muscle Regain less weight Reduction of abdominal fat

52
Weight Loss Strategies Physical Activity kCalorie expenditure Body weight, intensity, and duration Greater the energy deficit, greater the fat loss Discretionary kcalorie allowance (reward) Metabolism Speeds up with activity Immediate and long-term benefits
 Metabolism Speeds up with activity Immediate and long-term benefits")
53
Weight Loss Strategies – Physical Activity

54
Energy allowance to maintain weight Discretionary kcalorie allowance Energy intake to meet nutrient needs Sedentary personActive person kCalories 2500 2000 1500 1000 500 0

55
Weight Loss Strategies Physical Activity Body composition Fat decreases, esp. abdominal fat Lean body mass increases Strength-training exercises Appetite control Delayed appetite from released stored fuel Exercise curbs appetite from boredom, anxiety, depression

56
Weight Loss Strategies Physical Activity Psychological benefits Self-esteem Choosing activities Ones you enjoy & are willing to do regularly Convenience Energy-expending daily activities Spot reducing vs. strength training

57
Weight Loss Strategies– Environmental Influences Factors surrounding eating experience and the food itself Atmosphere Pleasant and comfortable equals more food Accessibility Less effort needed to obtain food, more food eaten

58
Weight Loss Strategies – Environmental Influences Socializing Duration of meal Visual cues Distraction Distractions Initiating eating Interfering with internal controls Extending duration of eating

59
Weight Loss Strategies – Environmental Influences Presence Sight, smell, or thought of food can prompt eating Multiple choice Large assortments of foods increase consumption Package and portion sizes Serving containers

62
Weight Loss Strategies – Behavior & Attitude Behavior modification Positive, matter-of-fact attitude Become aware of behaviors Keep record Change behaviors Set small, specific goals Practice, make new habits Reward

63
Eating not for Hunger See Emotional Eating Handouts Internet full of tips

64
Weight Loss Strategies – Behavior & Attitude Cognitive skills Problem solving Cognitive restructuring Replace negative thoughts Personal attitude Understand personal relationship with food Sound emotional health Support groups- WW, TOPS, OA

65
Weight Loss Strategies – Weight Maintenance Successful weight loss Plateau Appropriate goal at this point Prevalence of successful weight loss Difficult to determine Weight loss Without formal program Maintained for at least a year

66
Weight Loss Strategies – Weight Maintenance Components of successful weight loss Vigorous exercise regimens Careful eating patterns Frequent self-monitoring Changes in metabolism Takes more to prevent weight regain than to prevent weight gain

67
Preventing Weight Gain/Regain Strategies are similar to losing weight Read labels Watch portion size Change your grocery list Eat out less Ask yourself, “Am I hungry?” Exercise daily: Walk/bike more. Drive less. Plant a garden.

68
Public Health Programs Possibly change food environment through public health law Stretch beyond individual Social networks Community institutions Government policies

69
Public Health Programs

70
Underweight Affects no more than 5% of U.S. adults Weight gain is a matter of health Individual matter Weight gain may be difficult Physical conditioning combined with high energy intakes

71
Problems of Underweight Demand for energy contributes to underweight Physical activity Growth and development Difficult to gain weight Adaptive thermogenesis Learn new habits and like new foods Underweight vs. anorexia nervosa

72
Weight-Gain Strategies Key diet planning strategies Adequacy and balance Energy-dense foods Regular meals daily Large portions Extra snacks Juice and milk Exercise

73
Highlight 9 The Latest and Greatest Weight- Loss Diet – Again

74
Fad Diets Outrageous claims No requirements to prove the claims Do not have to support with credible research Distorted research Numerous fad diet plans

76
Fad Diets’ Appeal Market for weight-loss products is huge Greatest appeal Tend to ignore dietary recommendations Sophisticated and often erroneous explanations Too much rat data Tend to work for short time Fail to produce long-lasting results

77
“Don’t Count Calories?!” Claim to disregard kcalories Designed to have low energy intake Tend to lack variety Monotonous Often recommend dietary supplement Follow a plan Most fad diets cannot support optimal health over time

78
Dieting vs. Living Healthy Fad diet “magical powers” Tipping the energy balance equation to greater energy expenditure Weight loss Long-term lifestyle changes Healthy plan Flexibility and variety

Similar presentations