Download presentation
Presentation is loading. Please wait.

1
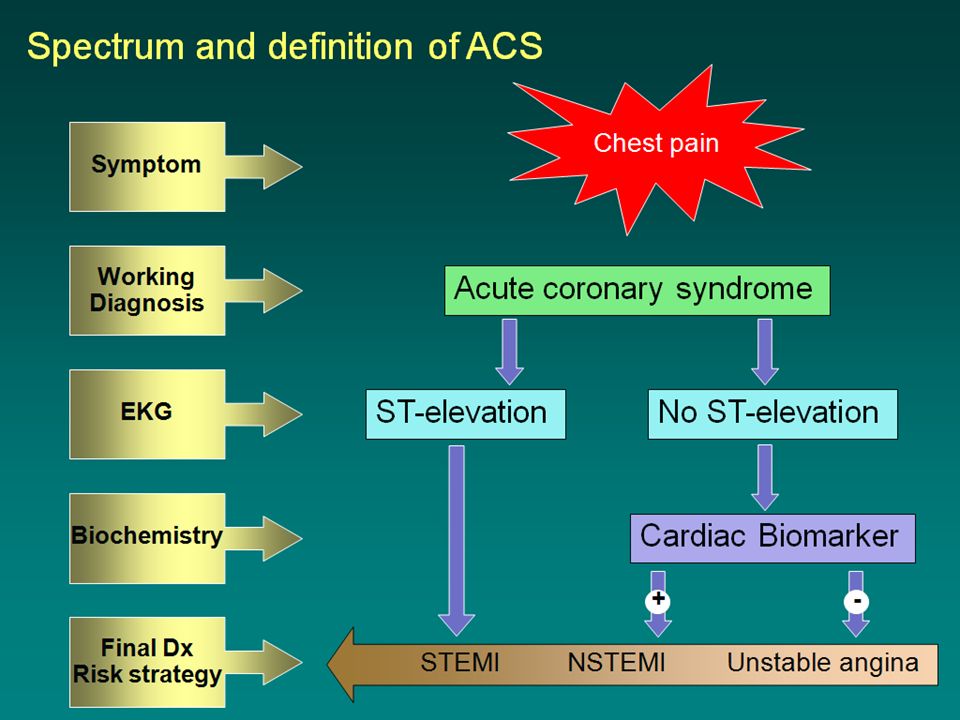
Acute STEMI: current approach

7
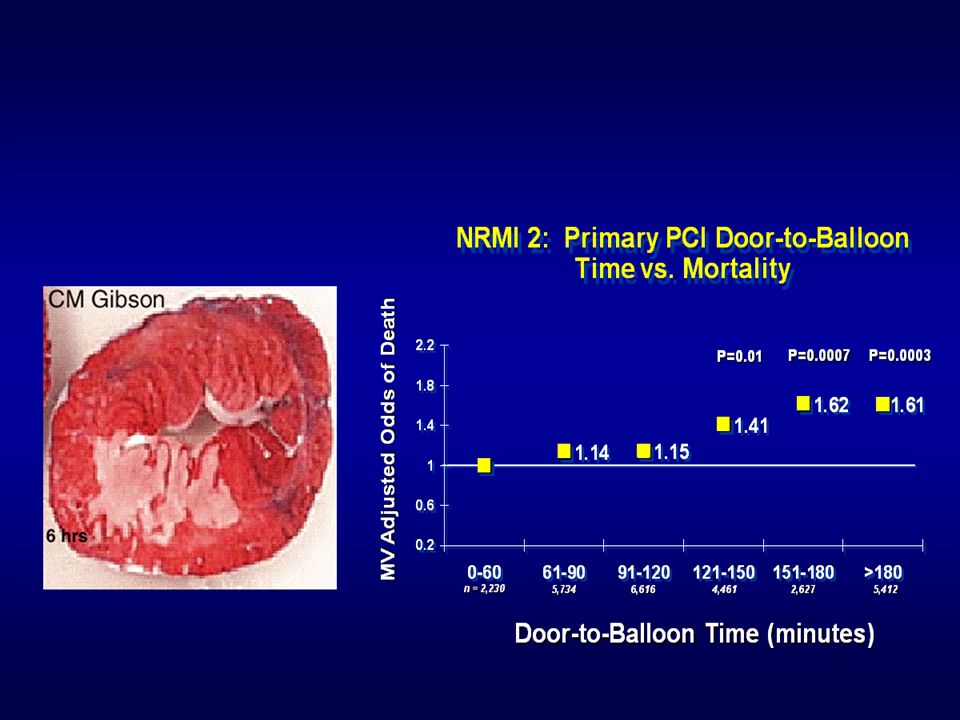
NSTEACS vs. STEACS Non occluding culprit lesion in 60-85 % Autolysis
Recurrent ischemia/MI No time dependent muscle lose Grayish-white (platelet-rich) vs. reddish (fibrin- rich) No role of fibrinolysis in STEACS (TIMI IIIB: ↑MI,↑trend of bleeding)
 vs. reddish (fibrin- rich) No role of fibrinolysis in STEACS (TIMI IIIB: ↑MI,↑trend of bleeding)")
10
ED Evaluation of Patients With STEMI
Differential Diagnosis of STEMI: Life-Threatening Aortic dissection Pulmonary embolus Perforating ulcer Tension pneumothorax Boerhaave syndrome (esophageal rupture with mediastinitis)
")
12
Cardiac Unit, Chest Disease Institute,
“ACS in the year 2011” Boonjong Saejueng, M.D., Cardiac Unit, Chest Disease Institute, Nonthaburi, Thailand

17
Management of STEMI

30
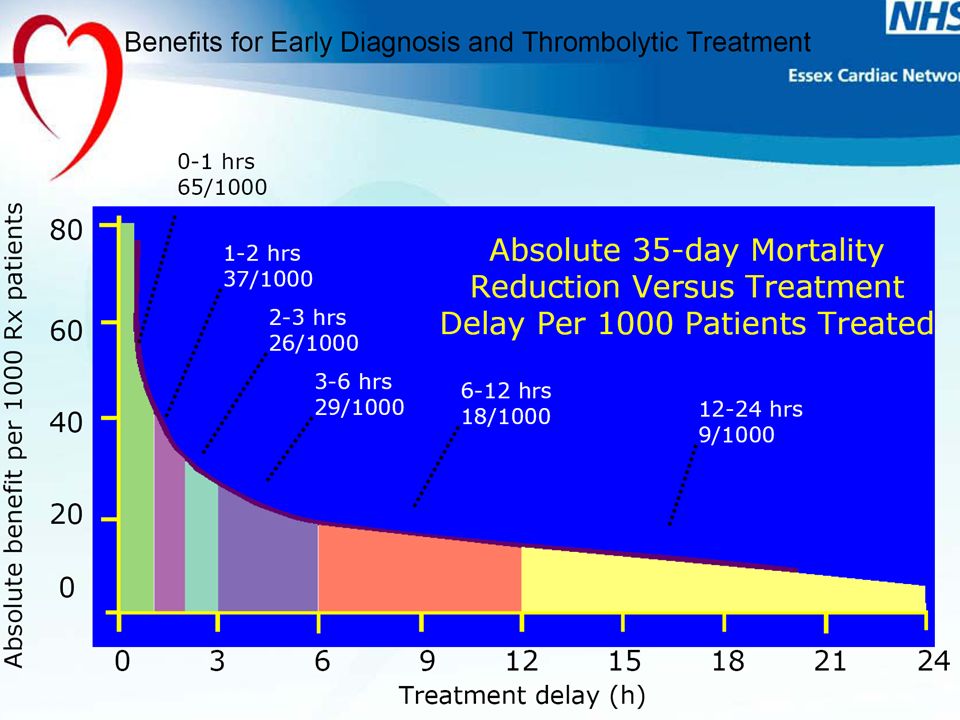
“Thrombolytic Therapy ”

31
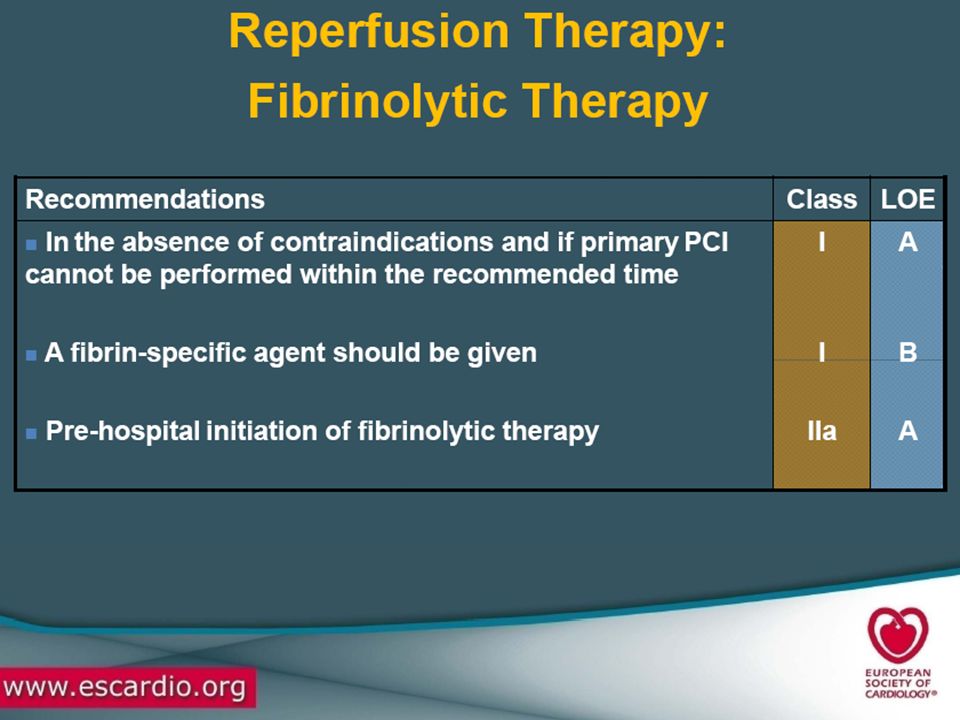
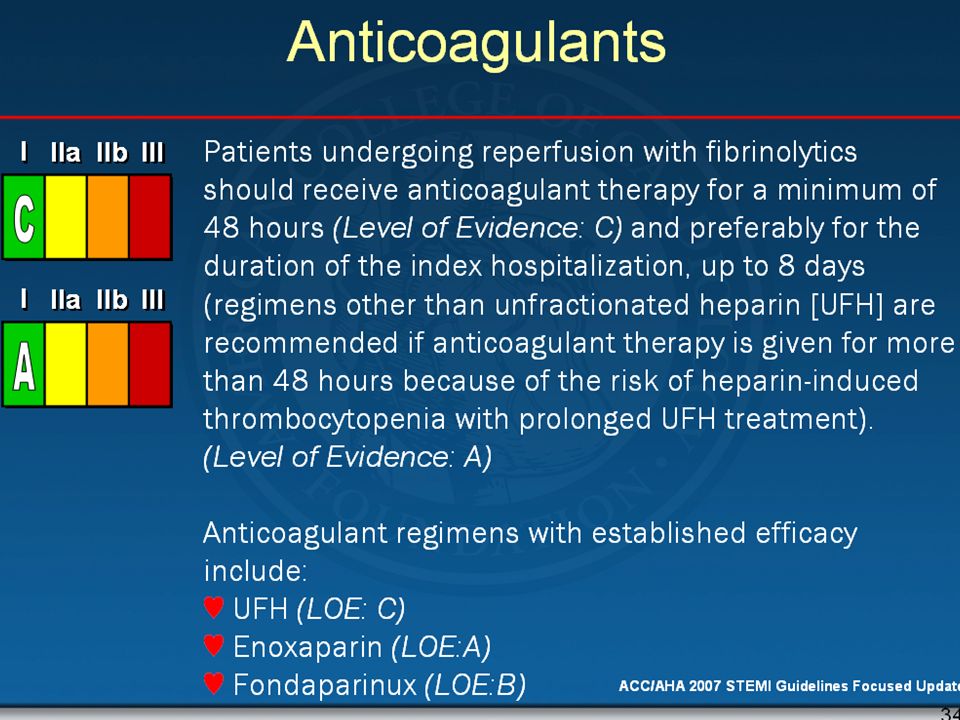
Fibrinolysis In the absence of contraindications, fibrinolytic therapy should be administered to STEMI patients with symptom onset within the prior 12 hours. In the absence of contraindications, fibrinolytic therapy should be administered to STEMI patients with symptom onset within the prior 12 hours and new or presumably new left bundle branch block (LBBB).
.")
36
“Antiplatelets”

38
Aspirin Aspirin should be chewed by patients who have not taken aspirin before presentation with STEMI. The initial dose should be 162 mg (Level of Evidence: A) to 325 mg (Level of Evidence: C) Although some trials have used enteric-coated aspirin for initial dosing, more rapid buccal absorption occurs with non–enteric-coated formulations.
 to 325 mg (Level of Evidence: C) Although some trials have used enteric-coated aspirin for initial dosing, more rapid buccal absorption occurs with non–enteric-coated formulations.")
44
Death/non-fatal MI at day 30 for the major subgroups
All interaction tests p = NS p < 0.5 1 2 Enoxaparin better UFH better Sex Male Female Age (years) < 75 75 Infarct location Anterior Other Diabetes No diabetes Diabetes Prior MI No prior MI Prior MI Fibrinolytic Streptokinase Fibrin specific Time-to-treatment < Median Median OVERALL N = 20,479 Reduction in risk (%) 18 16 20 6 11 23 17 21 13 12 The beneficial effect of enoxaparin on the primary endpoint was consistent across key pre-specified major subgroups including sex, age (< 75 years), infarct location, diabetes, history of myocardial infarction, type of fibrinolytic drug prescribed for the index event, and the time from the onset of symptoms to administration of the study drug. The p values for all interaction tests were not statistically significant. NS = not significant. Adapted with permission from Antman EM, et al. N Engl J Med. 2006;354:
 < 75. 75. Infarct location Anterior. Other. Diabetes No diabetes. Diabetes. Prior MI No prior MI. Prior MI. Fibrinolytic Streptokinase. Fibrin specific. Time-to-treatment < Median. Median. OVERALL N = 20,479. Reduction in risk (%) The beneficial effect of enoxaparin on the primary endpoint was consistent across key pre-specified major subgroups including sex, age (< 75 years), infarct location, diabetes, history of myocardial infarction, type of fibrinolytic drug prescribed for the index event, and the time from the onset of symptoms to administration of the study drug. The p values for all interaction tests were not statistically significant. NS = not significant. Adapted with permission from Antman EM, et al. N Engl J Med. 2006;354:")
45
Cumulative incidence of individual elements of the primary endpoints, death (left) and non-fatal myocardial infarction (right), in patients randomized to the enoxaparin vs. the unfractionated heparin strategy. Cumulative incidence of individual elements of the primary endpoints, death (left) and non-fatal myocardial infarction (right), in patients randomized to the enoxaparin vs. the unfractionated heparin strategy. The P-values were determined using the log-rank test. HR, hazard ratio. Morrow D A et al. Eur Heart J 2010;31: Published on behalf of the European Society of Cardiology. All rights reserved. © The Author For permissions please
 and non-fatal myocardial infarction (right), in patients randomized to the enoxaparin vs. the unfractionated heparin strategy. The P-values were determined using the log-rank test. HR, hazard ratio. Morrow D A et al. Eur Heart J 2010;31: Published on behalf of the European Society of Cardiology. All rights reserved. © The Author For permissions please")
46
Relative hazard rates and absolute event rates for the primary endpoint at 1 year in various subgroups. Relative hazard rates and absolute event rates for the primary endpoint at 1 year in various subgroups. The primary endpoint was the composite of death from any cause or non-fatal recurrent myocardial infarction. The overall treatment effect of the enoxaparin strategy when compared with unfractionated heparin is shown by the diamond (whose left and right edges represent the 95% confidence interval). For each subgroup, the square represents the point estimate of the treatment effect and the horizontal lines represent the 95% confidence intervals. Fibrin-specific fibrinolytic agents included alteplase, tenecteplase, and reteplase. Time to treatment indicates the time from the onset of symptoms to the administration of study drug (median, 3.2 h). P-values for testing for interaction were as follows: sex (P = 0.24), age (P = 0.32), infarct location (P = 0.57), diabetes mellitus (P = 0.32), prior myocardial infarction (P = 0.38), fibrinolytic (P = 0.95), and time to treatment (P = 0.02). Morrow D A et al. Eur Heart J 2010;31: Published on behalf of the European Society of Cardiology. All rights reserved. © The Author For permissions please
. For each subgroup, the square represents the point estimate of the treatment effect and the horizontal lines represent the 95% confidence intervals. Fibrin-specific fibrinolytic agents included alteplase, tenecteplase, and reteplase. Time to treatment indicates the time from the onset of symptoms to the administration of study drug (median, 3.2 h). P-values for testing for interaction were as follows: sex (P = 0.24), age (P = 0.32), infarct location (P = 0.57), diabetes mellitus (P = 0.32), prior myocardial infarction (P = 0.38), fibrinolytic (P = 0.95), and time to treatment (P = 0.02). Morrow D A et al. Eur Heart J 2010;31: Published on behalf of the European Society of Cardiology. All rights reserved. © The Author For permissions please")
53
Nitroglycerin Patients with ongoing ischemic discomfort should receive sublingual NTG (0.4 mg) every 5 minutes for a total of 3 doses, after which an assessment should be made about the need for intravenous NTG. Intravenous NTG is indicated for relief of ongoing ischemic discomfort that responds to nitrate therapy, control of hypertension, or management of pulmonary congestion.
 every 5 minutes for a total of 3 doses, after which an assessment should be made about the need for intravenous NTG. Intravenous NTG is indicated for relief of ongoing ischemic discomfort that responds to nitrate therapy, control of hypertension, or management of pulmonary congestion.")
54
Nitroglycerin Nitrates should not be administered to patients with:
Nitrates should not be administered to patients who have received a phosphodiesterase inhibitor for erectile dysfunction within the last 24 hours (48 hours for tadalafil). systolic pressure < 90 mm Hg or ≥ to 30 mm Hg below baseline severe bradycardia (< 50 bpm) tachycardia (> 100 bpm) or suspected RV infarction.
. systolic pressure < 90 mm Hg or ≥ to 30 mm Hg below baseline. severe bradycardia (< 50 bpm) tachycardia (> 100 bpm) or. suspected RV infarction.")
56
Practical demonstration of the ST segment resolution score (STR) in a patient treated by fibrinolysis for an acute anterior myocardial infarction. Practical demonstration of the ST segment resolution score (STR) in a patient treated by fibrinolysis for an acute anterior myocardial infarction. (A) ECG on admission. The maximum ST segment elevation is observed in lead V2 (8 mm). (B) ECG performed 90 min after fibrinolysis. Now the maximum ST segment elevation is only 3 mm, implying an STR above 50%. Eeckhout E Heart 2007;93: ©2007 by BMJ Publishing Group Ltd and British Cardiovascular Society
 in a patient treated by fibrinolysis for an acute anterior myocardial infarction. (A) ECG on admission. The maximum ST segment elevation is observed in lead V2 (8 mm). (B) ECG performed 90 min after fibrinolysis. Now the maximum ST segment elevation is only 3 mm, implying an STR above 50%. Eeckhout E Heart 2007;93: ©2007 by BMJ Publishing Group Ltd and British Cardiovascular Society.")
58
Wijeysundera, H. C. et al. J Am Coll Cardiol 2007;49:422-430
Efficacy End Points for Repeat Fibrinolytic Therapy Versus Conservative Therapy Wijeysundera, H. C. et al. J Am Coll Cardiol 2007;49: Copyright ©2007 American College of Cardiology Foundation. Restrictions may apply.

59
Wijeysundera, H. C. et al. J Am Coll Cardiol 2007;49:422-430
Safety End Points for Repeat Fibrinolytic Therapy Versus Conservative Therapy Wijeysundera, H. C. et al. J Am Coll Cardiol 2007;49: Copyright ©2007 American College of Cardiology Foundation. Restrictions may apply.

62
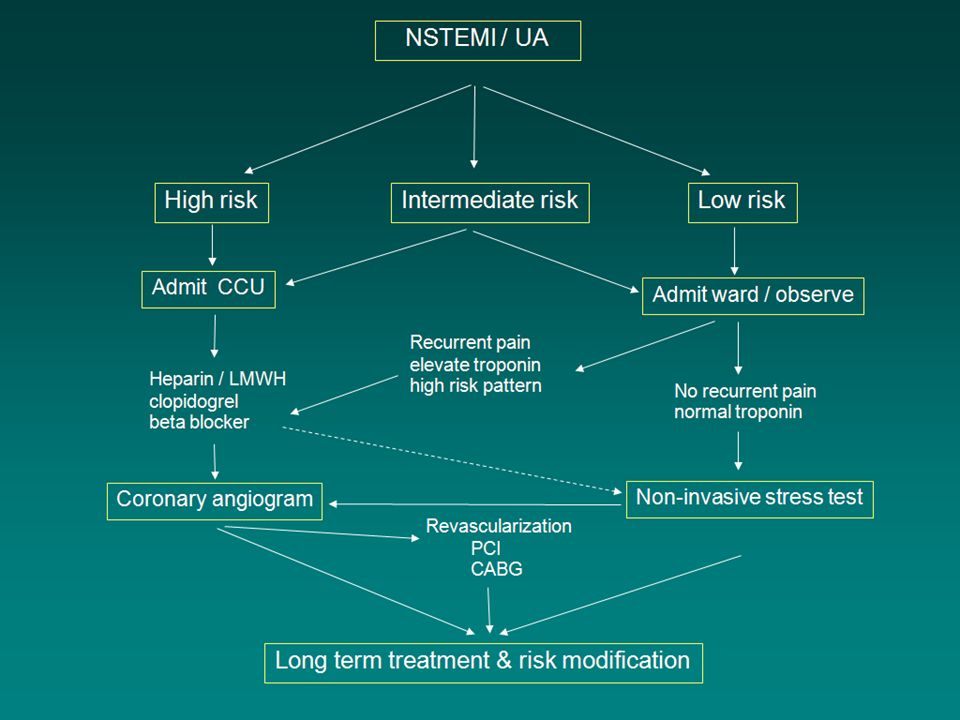
Non-ST-elevation acute coronary syndromes (NSTEACS)
Unstable angina (UA) Non-ST-elevation myocardial infraction (NSTEMI)
 Non-ST-elevation myocardial infraction (NSTEMI)")
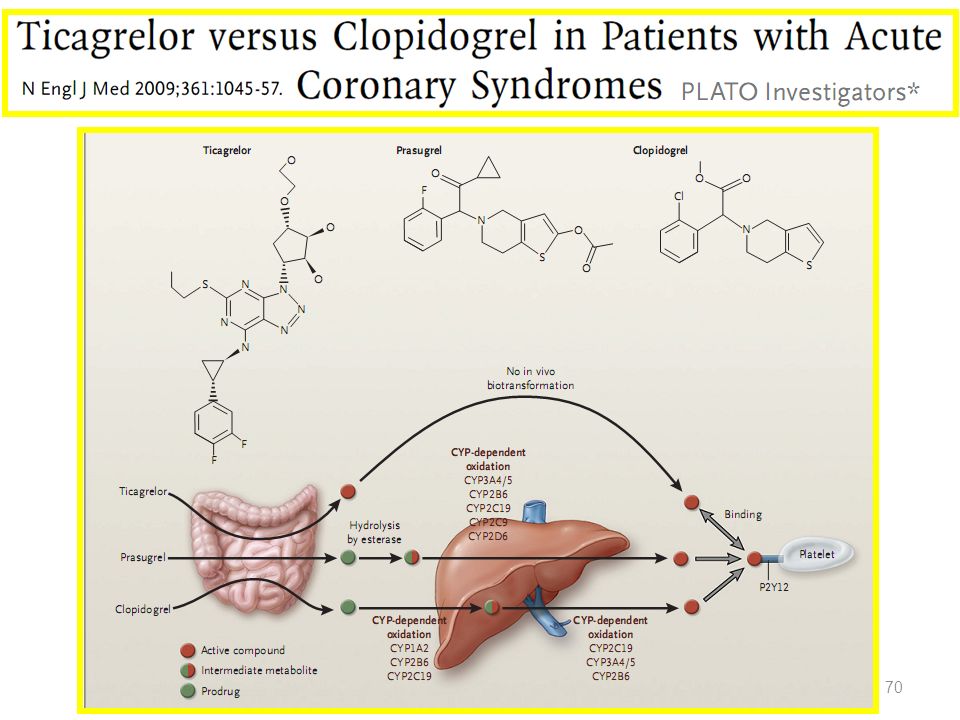
72
Cyclo-pentyl 72

99
PPIs and Antiplatelet Therapy
IIa IIb III PPI should be used in patients with history of prior GI who require DAPT. PPI use is reasonable in patients with increased risk of gastrointestinal bleeding (advanced age, concomitant use of warfarin, steroids, nonsteroidal anti-inflammatory drugs, H pylori infection, etc.) who require DAPT. Routine use of a PPI is not recommended for patients at low risk of gastrointestinal bleeding, who have much less potential to benefit from prophylactic therapy. I IIa IIb III I IIa IIb III No Benefit 99
 who require DAPT. Routine use of a PPI is not recommended for patients at low risk of gastrointestinal bleeding, who have much less potential to benefit from prophylactic therapy. I. IIa. IIb. III. I. IIa. IIb. III. No Benefit. 99.")
Similar presentations

























































 Trial Comparison of the safety and efficacy of unfractionated heparin versus enoxaparin in combination.>")







. ACS Pathophysiology is that of a ruptured or eroded atheromatous plaque. Pathophysiology is that of a ruptured or eroded.>")







 Trial Paul W. Armstrong, WEST Steering Committee Published in The European Heart Journal.>")


 Trial ASSENT- 4 PCI Trial Presented.>")