Download presentation
Presentation is loading. Please wait.

1
Jaundice Dr. Gehan Mohamed Dr. Abdelaty Shawky

2
Learning objectives Understand mechanism of Bilirubin formation and how its increase can lead to jaundice. Discuss Pathophysiologic classification of Jaundice and clinical characteristics of each type.

3
Jaundice (icterus) It is a yellowish pigmentation of the skin, the sclera, and other mucous membranes . Jaundice is not a disease but it is a sign of other diseases.

5
* Causes of Jaundice: Caused by hyperbilirubinemia (increased levels of bilirubin in the blood). This hyperbilirubinemia subsequently causes increased levels of bilirubin in the extracellular fluid. A concentration higher than 1.8 mg/dL leads to jaundice.
. This hyperbilirubinemia subsequently causes increased levels of bilirubin in the extracellular fluid. A concentration higher than 1.8 mg/dL leads to jaundice.")
6
Bilirubin formation RBCs Senecent RBCs Bilirubin Biliverdin heme
120ds Bilirubin RBCs Senecent RBCs Iron hemoglobin Globin Bilirubin Biliverdin heme Hepatic Hemoproteins Premature destruction of newly formed RBCs 1-5% Chiefly 70+% 20%

7
Bilirubin Metabolism After destruction of red blood cells hemoglobin(HB) will be released. Then hemoglobin will be splitted into heme and globin. Then heme is changed into biliverdin then to bilirubin. But bilirubin is water insoluble so can not excreted directly into urine to eliminate it . To overcome this problem this bilirubin must be carried by plasma proteins such as albumin to inside liver . Inside hepatocytes the unconjugated bilirubin undergo conjugation by glucoronic acid and form the conjugated bilirubin which is water soluble.

8
This conjugated bilirubin is excreted from the liver into the biliary and cystic ducts as part of bile. Intestinal bacteria convert the bilirubin into urobilinogen. From here the urobilinogen can take two pathways: a. It can either be further converted into stercobilinogen, which is then oxidized to stercobilin and passed out in the feces. b. or it can be reabsorbed by the intestinal cells, transported in the blood to the kidneys, and passed out in the urine as the oxidised product urobilin. Stercobilin and urobilin are the products responsible for the coloration of feces and urine, respectively.

10
Types of bilirubin Unconjugated bilirubin(UCB):because of its lipid solubility and not water soluble, it is not excreted in urine. Conjugated bilirubin (CB): is water soluble, so it is filtered at the glomerulus and appears in the urine.
: is water soluble, so it is filtered at the glomerulus and appears in the urine.")
11
Physiologic Neonatal jaundice
it is often seen in infants around the second day after birth, lasting until day 8 in normal births, or to around day 14 in premature births . the jaundice is presumably a consequence of metabolic and physiological adjustments after birth. it is usually harmless. Serum bilirubin normally drops to a low level without any intervention required. exposing the baby to intensive phototherapy. Bilirubin count is lowered through bowel movements and urination so regular and proper feedings are especially important

12
Pathologic jaundice

13
* Pathophysiologic classification of Jaundice:
1. Pathologic neonatal Jaundice. 2. Hemolytic Jaundice. 3. Obstructive Jaundice (Cholestasis). 4. Hepatic Jaundice.
. 4. Hepatic Jaundice.")
14
1. Pathologic Neonatal jaundice
In cases where bilirubin rises higher and so jaundice persist for more than 3 weeks after birth. this neonatal hyperbilirubinemia May be due to congenital absence for the enzymes required for bilirubin conjugation inside liver. Most dangerous complication is brain-damage due to deposition of bilirubin,a condition known as kernicterus leading to significant lifelong disability.

15
2. Hemolytic Jaundice. Overproduction of Unconjugated Bilirubin can result from Excess Hemolysis e.g. in sickle cell anaemia, spherocytosis, thalassemia, malaria, autoimmune disorders… Overproduction of heme may overload the liver with excess unconjugated Bilirubin.

16
* Lab investigations of hemolytic jaundice:
Increase Unconjugated bilirubin. urobilinogen in feces and urine hemoglobinuria (in acute intravascular hemolysis) Reticulocyte counts
 Reticulocyte counts.")
17
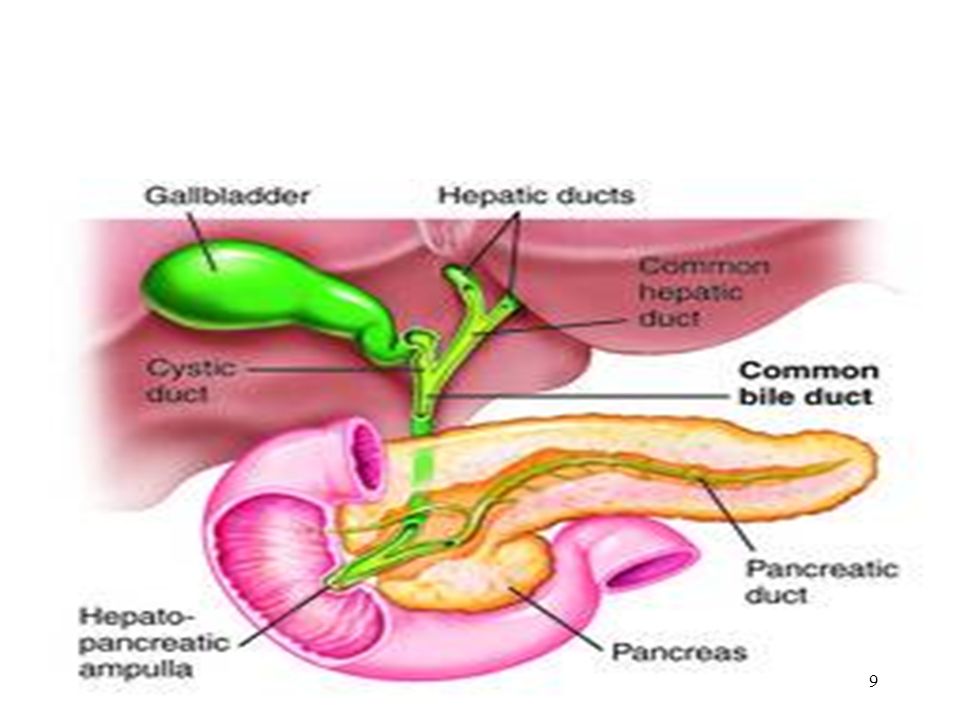
3. Obstructive Jaundice - It is due to extra hepatic obstruction of bile ducts so conjugated bilirubin can not reach intestine. * Causes of obstruction of bile duct: 1. Gall bladder Stones. 2. Fibrous Stricture of the biliary ducts following Inflammatory lesions. 3. Tumors of Ampulla of Vater can compress bile duct from outside.

18
* Clinical picture of obstructive jaundice:
Yellow color of skin, mucous membranes. Severe itching or "pruritus" because of the deposition of bile salts in skin.

19
* Lab investigations of Obstructive Jaundice:
Serum Bilirubin Reduced of absent Fecal urobilinogen Reduced or absent stercobilinogen. bilirubinuria (conjugated type)
")
20
4. Hepatic Jaundice Due to a disease affecting hepatic tissue either congenital or acquired leading to hepatocellular damage e.g. Hepatitis, Cirrhosis, tumors…

21
* Lab investigations of hepatic jaundice:
liver function tests are abnormal both Conjugated Bilirubin and Unconjugated Bilirubin.

22
Thanks

Similar presentations



>")

CM Clinical Chemistry>")






 LIVER FUNCTION AND THE BILIARY TRACT LECTURE FOUR Dr. Essam H. Aljiffri.>")
 LIVER FUNCTION AND THE BILIARY TRACT LECTURE THREE Dr. Essam H. Aljiffri.>")






