Download presentation
Presentation is loading. Please wait.

1
The International Psycho-Oncology Society (IPOS)
Jimmie C. Holland, M.D. Wayne E. Chapman Chair in Psychiatric Oncology Memorial Sloan-Kettering Cancer Center New York, New York 7th World Congress 2004*

3
IPOS: Founded 1984 To improve the “human” side of cancer care on a global basis

4
IPOS: 1984 Foster international communication
Educate professionals in psychosocial care across countries Advocate for making psychosocial an integral part of total cancer care Examine social, cultural factors that impact quality of life and care

5
An International Survey of Physician Attitudes and Practice in Regard to Revealing the Diagnosis of Cancer Jimmie C. Holland, M.D., Natalie Geary, B.A., Anthony Marchini, B.A., and Susan Tross, Ph.D. Psychiatry Service Memorial Sloan-Kettering Cancer Center New York, New York, 10021 Cancer Investigation, 5(2), (1987)
, (1987)")
6
Oncologists Estimated Percentage of Physicians in Their Country Who Disclose Cancer Diagnosis
N = 90 oncologists; 20 countries Tell to the Patient: LOW% HIGH% Africa Austria France Denmark Hungary Finland Iran Netherlands Panama New Zealand Portugal Norway Spain Switzerland Sweden Tell to the Family: High % estimated by majority of physicians

7
IPOS: 2005 Conducted 7 World Congresses 2006, Venice
Education Conducted 7 World Congresses , Venice > 25 national psycho-oncology societies International journal, 1992 Psycho-Oncology Text books in English, Spanish, Italian, and Japanese

8
IPOS: 2005 Education 2004 Website: www.ipos-society.org
Core curriculum online – FREE 4 lectures, with European School of Oncology in Italian German French Hungarian Spanish English

9
IPOS: 2005 Requested to become an NGO of World Health Organization
Rationale: to add a psychological, social and behavorial dimension to WHO national cancer control programs

10
WHO Priority Action Plan for National Cancer Control Programs
Resources A B C Low Medium High Prevention Early diagnosis Screening/therapy Pain/palliative care PSYCHOSOCIAL

11
WHO Cancer Prevention Program
Depends on changes in life style and exposures: must alter BEHAVIOR Psychological and social factors are critical considerations in prevention education which must be culture and language-sensitive Behavioral scientists needed (Tobacco Cessation)
")
12
WHO Cancer Control Program Early Diagnosis
Fatalistic attitudes, fear of stigma of cancer, and ignorance are problems, especially in developing countries Public education requires attention to psychological, social, cultural, and behavioral factors

13
WHO Cancer Control Screening
Participation in screening require attention to local social attitudes, beliefs, trust in procedures/staff, and awareness of cultural factors Requires knowledge of community, beliefs, and fears

14
WHO Priorities for National Cancer Control Programs
Pain/Palliative Care

15
In Palliative Care Pain is often the primary focus
Psychological issues are often not identified and treated as an equally important aspect of end-of-life care Need for more participation of psycho- oncologists in end-of-life for clinical and research collaboration

16
IPOS Goals in Palliative Care
Encourage recognition, diagnosis and treatment of psychosocial and psychiatric problems Develop standards and clinical practice guidelines for psychological care

17
National Programs Standards and Guidelines
Australia United Kingdom Canada United States

18
US Example: 1999 A Multidisciplinary Panel (NCCN)
Chose “DISTRESS” as an encompassing word to cover psychosocial/ psychiatric and spiritual A rapid one-item screening question Standards care and Clinical Practice Guidelines for mental health, social work, clergy

19
DISTRESS CONTINUUM Normal Distress Fears Worries Sadness
Severe Distress Depression, Anxiety Family Spiritual

20
STANDARDS OF CARE FOR MANAGEMENT OF DISTRESS - 1
Distress should be recognized, monitored, documented and treated promptly at all stages of disease All patients should be screened for distress at their initial visit and as clinically indicated Screening should identify the level and nature of the distress Distress should be assessed and managed by evidence or consensus-based clinical practice guidelines Adapted, NCCN

21
BRIEF SCREENING TOOL AND PROBLEM LIST
During the past week, how distressed have you been? Please indicate your level of distress on the thermometer and check the causes of your distress. Practical problems __ Housing __ Insurance __ Work/school __ Transportation __ Child care Family problems __ Partner __ Children Emotional problems __ Worry __ Sadness __ Depression __ Nervousness Spiritual/religious concerns __ Relating to God __ Loss of faith __ Other problems Physical problems __ Pain __ Nausea __ Fatigue __ Sleep __ Getting around __ Bathing/dressing __ Breathing __ Mouth sores __ Eating __ Indigestion __ Constipation/diarrhea __ Bowel changes __ Changes in urination __ Fevers __ Skin dry/itchy __ Nose dry/congested __ Tingling in hands/feet __ Feeling swollen __ Sexual problems Extreme Distress No Distress BRIEF SCREENING TOOL AND PROBLEM LIST

23
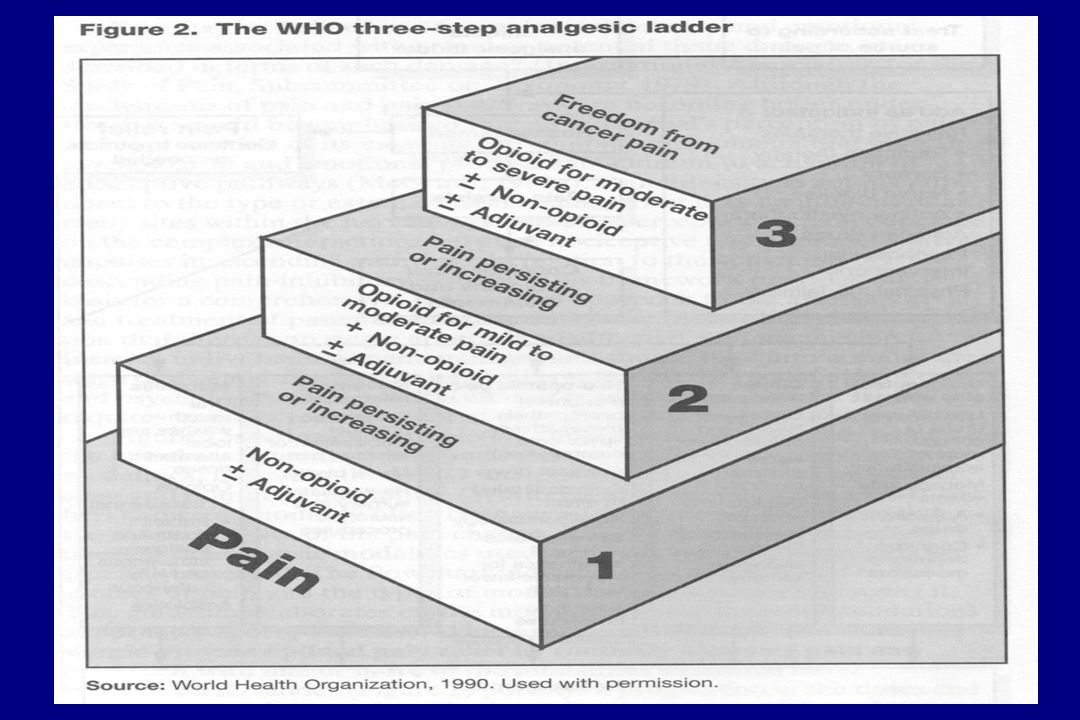
DISTRESS LADDER: MANAGEMENT BY STANDARDS & PRACTICE GUIDELINES
≥ 5 DISTRESS Scale (0–10) < 5 Adapted from WHO Analgesic Ladder
 < 5. Adapted from WHO Analgesic Ladder.")
24
Canada June, 2004 The National Cancer Council
Distress added as the 6th vital sign (temperature, pulse, respiration, blood pressure, pain, distress) To be asked about routinely at patient visits
 To be asked about routinely at patient visits.")
25
Major Barriers in Every Country
Poor to absent funding Absence of oversight and accountability (changing in Australia, Canada, UK) Awareness of the importance to patients and families (especially in palliative care) Mehnert and Koch, 2003
 Awareness of the importance to patients and families (especially in palliative care) Mehnert and Koch,")
26
Action Item - 1 IPOS, with WHO, seeks to bring the psychosocial domain into global cancer control programs IPOS advocates for national standards and clinical practice guidelines

27
Action Item - 2 IPOS provides oversight of global efforts
Collate international data for cross- cultural studies Promotes multidisciplinary multi-national research

28
Action Item - 3 Establish WHO-supported international standards and guidelines For use by national societies to impact policies on service delivery To provide professional training standards To influence national funding priorities To impact governmental agencies via WHO, UICC, IARC To foster research for evidence-based care

29
“What we value can be seen in what we measure.”
Dr. Robert McMurtry “Public Policy, Human Consequences: The Gap Between Biomedicine and Psychosocial Reality” Canada Oncology Exchange, 2003

30
PAIN DISTRESS

31
8th WORLD CONGRESS PSYCHO-ONCOLOGY
"Multidisciplinary Psychosocial Oncology: Dialogue and Interaction" October 2006 Palazzo del Cinema Venice, Italy Details will continue to be posted on the conference website at

Similar presentations

 Ms. Noeleen Heyzer Under Secretary-General and Executive Secretary.>")


















>")