Download presentation
Presentation is loading. Please wait.

1
Oncological Emergencies
Dr. Gary Harding MD, FRCPC Medical Oncology Fellow CancerCare Manitoba

2
CASE 1…

3
Mr. SV ID: 65 year old male with PMHx of CAD and emphysema
EC: present to clinic with one week history of increasing SOB HPI: 3 month history of weight loss, decreased appetite, a change in his chronic cough, and intermittent hemoptysis

4
On Physical Examination
Inspection:

5
Respiratory Examination
Stridor Dullness to percussion on right lower lung fields Increased tactile fremitus to right lower lung fields Decreased A/E to right lower lung fields

6
Chest X-Ray…

7
right pleural effusion

8
Thoracentesis Exudate Gram stain AFB stain Cytology Negative
non-small cell lung cancer Large cell type

9
T1-weighted axial MRI demonstrating paratracheal soft tissue mass that invades into the SVC

10
Superior Vena Cava Syndrome

11
Definition Obstruction of blood flow in the superior vena cava results in signs and symptoms of SVC syndrome

13
Etiology Caused by either invasion or external compression of the SVC by contiguous pathologic process Right lung pathology, lymph nodes, other mediastinal structures, or thrombosis

14
Etiology Before antibiotics the most common causes were from complications of untreated infection Syphilitic thoracic aneurysms fibrosing mediastinitis Malignancy is presently the most common cause

15
Symptoms and Signs As the obstruction develops venous collaterals are formed Symptom onset depends on speed of SVC obstruction onset Malignant disease can arise in weeks to months Not enough time to develop collaterals Fibrosing mediastinitis can take years to have symptoms

16
Symptoms and Signs Central venous pressures remain high even in collaterals High pressures cause the characteristic clinical picture Shortness of breath is the most common symptom1 1. Parish, JM, Marschke, RF Jr, Dines, DE, Lee, RE. Etiologic considerations in superior vena cava syndrome. Mayo Clin Proc 1981; 56:407.

17
Signs and Symptoms Facial swelling or head fullness Cough Arm edema
exacerbated by bending forward or lying down Cough Arm edema Cyanosis

18
Facial swelling associated with SVC Syndrome in a patient with malignancy

19
Physical Findings Venous distension Pemberton’s Sign Facial Edema neck
chest wall Pemberton’s Sign Facial Edema

20
Patient who presented with progressively enlarging veins over the anterior chest wall. A diagnosis of a right-sided superior sulcus (Pancoast) tumor compressing the SVC was made.
 tumor compressing the SVC was made..")
21
Etiology: Malignancy Lung cancer is the most common2
Lymphoma is second most common together represent 94% of cases 2. Escalante, CP. Causes and management of superior vena cava syndrome. Oncology (Huntingt) 1993; 7:61.
 1993; 7:61.")
22
NSCLC 2-4% of bronchogenic cancer patients develop SVC syndrome3
extrinsic compression or direct invasion primary tumor or by enlarging mediastinal nodes 3. Armstrong, BA, Perez, CA, Simpson, JR, Hederman, MA. Role of irradiation in the management of superior vena cava syndrome. Int J Radiat Oncol Biol Phys 1987; 13:531.

23
Small Cell Lung Cancer Greatest risk 20% will develop SVC obstruction3
more common because SCLC tends to occur centrally in contrast to other types

24
Lymphoma 2-4% of patients predominantly non-Hodgkin’s lymphoma4
Hodgkin’s rarely causes SVC syndrome 4. Perez-Soler, R, McLaughlin, P, Velasquez, WS, et al. Clinical features and results of management of superior vena cava syndrome secondary to lymphoma. J Clin Oncol 1984; 2:260.

25
Lymphoma Extrinsic compression caused by enlarging lymph nodes
subtypes of large B cell can be intravascular and cause occlusion (angiotropic) diffuse large cell and lymphoblastic are most commonly associated with SVC syndrome
 diffuse large cell and lymphoblastic are most commonly associated with SVC syndrome.")
26
Other cancers Thymoma primary mediastinal germ cell neoplasm
solid tumors with mediastinal nodal metastases breast cancer most common type

27
Other causes Post radiation local vascular fibrosis can also be considered in oncology patients Thoracic radiation treatment may predate syndrome by many years

28
Other causes Thrombosis Indwelling central venous catheters
Subcutaneous tunneled catheters have fewer thrombotic and infectious complications Can also cause pulmonary embolism5 5. Sivaram, CA, Craven, P, Chandrasekaran, K. Transesophageal echocardiography during removal of central venous catheter associated with thrombus in superior vena cava. Am J Card Imaging 1996; 10:266.

29
Diagnosis Timely identification of the cause is essential
Radiographic studies are useful Up to 60% of patients with SVC syndrome related to neoplasm do not have a known diagnosis of cancer6 Need a tissue biopsy for histologic studies 6. Schraufnagel, DE, Hill, R, Leech, JA, Pare, JA. Superior vena caval obstruction. Is it a medical emergency?. Am J Med 1981; 70:1169.

30
Radiographic Studies Most patients have an abnormal chest x-ray at presentation Most common findings are Mediastinal widening Pleural effusion

31
CT Chest Preferred choice IV contrast defines the level of obstruction
Maps out collateral pathways Can identify underlying cause of obstruction

32
Venography Bilateral upper arm venograpy
superior to CT to define site of obstruction Does not define cause unless thrombosis is solely responsible

33
Helical CT With bilateral upper arm IV contrast injection
Best visualization of level of obstruction and cause

34
MRI Can be useful in patients with IV contrast allergies

35
T1-weighted axial MRI demonstrating the primary tumor and the paratracheal soft tissue mass that invades into the SVC

36
Same patient’s MRI with different technique to further define the intramural mass

37
Histologic Diagnosis Essential Guides treatment
Aids in defining prognosis

38
Histologic Diagnosis Sputum cytology, pleural fluid cytology, biopsy of enlarged peripheral nodes Bone marrow biopsy for NHL Bronchoscopy, mediastinoscopy, or thoracotomy are more invasive but sometimes necessary

39
Treatment of Oncologic Causes

40
Treatment Aimed at underlying cause
Evolution of thought has occurred in recent years

41
Historically SVC syndrome was considered a potentially life-threatening emergency
Standard of care was immediate radiotherapy Zap now Ask questions later The emergent approach is not appropriate for most patients

42
Newer strategies

43
Emergent to Urgent Symptomatic obstruction is usually a prolonged process Most patients are not in immediate danger at presentation Most have time for a full diagnostic work up

44
Emergent to Urgent Prebiopsy radiation can obscure the diagnosis
Current strategies aim at accurate diagnosis of underlying etiology before therapy

45
Exception to new rule Stridor True medical emergency
Central airway obstruction or laryngeal edema True medical emergency Immediate action needed Possible intubation and ICU admission Immediate therapy to target obstruction needed

46
Linked to tumor histology and stage at presentation
Prognosis… Linked to tumor histology and stage at presentation

47
Treatment Sensitive Tumors
NHLs, germ cells, and limited-stage small cell lung cancers usually respond to chemotherapy and or radiation Can achieve long term remission with tumor specific directed therapy Symptomatic improvement usually takes 1-2 weeks after start of therapy

48
Note: Corticosteroids
Controversial issue with regards to treatment benefit at presentation

49
Non-small cell lung cancer
SVC obstruction is a strong predictor of poor prognosis Median survival around 5 months7 Choice of therapy considers likelihood of response to each modality 7. Martins, SJ, Pereira, JR. Clinical factors and prognosis in non-small cell lung cancer. Am J Clin Oncol 1999; 22:453.

50
Non-small cell lung cancer
Goal usually directed to palliation rather than long term remission Palliative radiation and chemotherapy can be used

51
Intraluminal Stents Endovascular placement under fluoroscopy
Patients who have recurrent disease in previously irradiated fields Tumors refractory chemotherapy Patient too ill to tolerate radiation or chemotherapy

52
Intraluminal Stents Some data suggests benefit from immediate stent placement in NSCLC at presentation8 Tends to provide more rapid relief of symptoms Issue of anticoagulation after is not resolved 8. Rowell, NP, Gleeson, FV. Steroids, radiotherapy, chemotherapy and stents for superior vena caval obstruction in carcinoma of the bronchus: a systematic review. Clin Oncol (R Coll Radiol) 2002; 14:338.
 2002; 14:338.")
53
CASE 2…

54
Mr. EC ID: 56 year old man with history of HTN and osteoarthrtis
EC: presents to family doctor with one month history of back pain that is not responding to Tylenol Pain beginning to wake him at night More pain with recumbancy Some shooting pains down right leg ROS: negative

55
On examination vitals stable, no fever
CVS, Respiratory, GI, GU exams reported as normal Back exam Inspection: normal Palpation: some pain in L1 ROM: normal Some pain in right leg with straight leg raising

56
Investigation in Clinic
Lumbar Spine X-ray Some age related degeneration

57
Diagnosis Sciatica vs. Back strain Treatment: NSAIDS
Few days of bed rest

58
The story continues… Mr. EC’s pain does not resolve
More trials of various forms of pain control fail One month later Mr. EC awakens in the morning and has difficulty supporting his weight Subjective leg muscle weakness Goes to HSC Emergency room

59
In ER Patient has objective leg weakness on physical exam
A very keen medical student does a rectal exam and discovers a large nodular prostate PSA: 45.0 MRI Spine…..

61
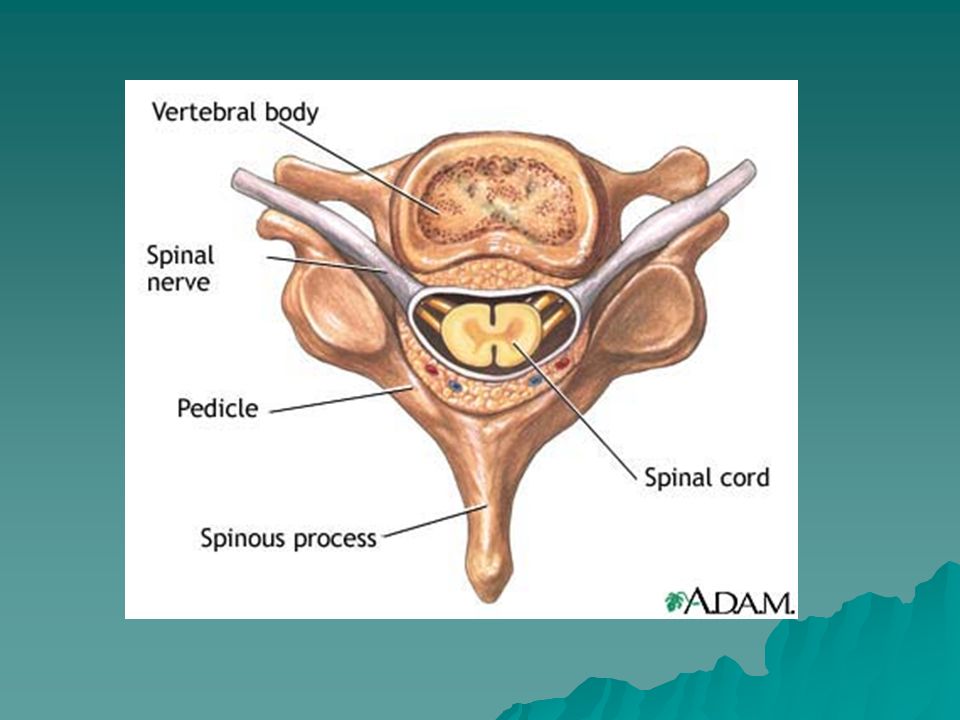
Spinal Cord Compression

62
Malignant Epidural Spinal Cord Compression (ESCC)
Neoplastic invasion of the space between vertebrae and spinal cord (epidural invasion) Usually from bone metastases Compresses thecal sac of spinal cord Frequent complication of malignancy Can cause pain Can cause irreversible loss of neurologic function
 Usually from bone metastases. Compresses thecal sac of spinal cord. Frequent complication of malignancy. Can cause pain. Can cause irreversible loss of neurologic function.")
65
Definition Any radiological indentation of the thecal sac
Tip of the spinal cord lies at the L1 vertebral level Lumbosacral nerve roots form the cauda equina

66
Epidemiology Many cases of unrecognized ESCC
Difficult to define incidence Autopsy review studies suggest around 5% of cancer patients die with ESCC9 9. Barron, KD, Hirano, A, Araki, S, Terry, RD. Experiences with metastatic neoplasms involving the spinal cord. Neurology 1959; 9:91.

67
Causes Metastatic tumor from any primary site
Tumors with predilection to metastasize to spinal column Prostate, breast, and lung carcinoma 15-20% of cases Renal cell, non-Hodgkin’s lymphoma, or myeloma 5-10% of cases

68
Vertebral metastases are more common than ESCC Prostate cancer: 90%
Breast Cancer: 74% Lung Cancer: 45% Lymphoma: 29% Renal cell: 29% GI: 25% 10. Posner, JB. Neurologic Complications of Cancer. FA Davis, Philadelphia, 1995

69
ESCC can be initial presentation of a malignancy
Around 20% of cases In many cases diagnosis is made by biopsy of the spinal lesion

70
Spinal Location10 Thoracic spine: 60% Lumbosacral spine: 30%
Cervical spine: 10% Specific tumor predilection is difficult to define

71
Clinical Features

72
Important to recognize Early recognition leads to better outcomes
Efficacy of treatment depends most on patient’s neurological function at presentation Median time from symptoms to diagnosis is around 2 months11 More than half of patients who present to hospital are non-ambulatory 11. Husband, DJ. Malignant spinal cord compression: Prospective study of delays in referral and treatment. BMJ 1998; 317:18.

73
RED FLAGS…..

74
First Red Flag: Pain Usually first symptom12
80-90% of the time Usually precedes other neurologic symptoms by seven weeks Increases in intensity Severe local back pain Aggravated by recumbency Distension of venous plexus May become radicular 12. Bach, F, Larsen, BH, Rohde, K, et al. Metastatic spinal cord compression. Occurrence, symptoms, clinical presentations and prognosis in 398 patients with spinal cord compression. Acta Neurochir (Wien) 1990; 107:37.
 1990; 107:37.")
75
Second Red Flag: Motor Weakness: 60-85%13 At or above conus medularis
Extensors of the upper extremities Above the thoracic spine Weakness from corticospinal dysfunction Affects flexors in the lower extremities Patients may be hyperreflexic below the lesion and have extensor plantars 13. Greenberg, HS, Kim, JH, Posner, JB. Epidural spinal cord compression from metastatic tumor: Results with a new treatment protocol. Ann Neurol 1980; 8:361.

76
Weakness tends to be symmetrical
Progressive weakness is followed by lost of gait function then paralysis The severity of weakness is greatest with thoracic metastases

77
Third Red Flag: Sensory
Less common than motor findings Still present in majority of cases Ascending numbness and parathesias

78
Fourth Red Flag: Bladder and Bowel Function
Loss is late finding Autonomic neuropathy presents usually as urinary retension Rarely sole finding

79
Radiologic Investigation

80
Diagnosis depends on ability to demonstrate a mass compressing the thecal sac
Plain radiographs are not enough Historically this involved invasive procedures Advent of MRI has allowed non-invasive diagnosis Clinical examination is not reliable in determining level of lesion

81
Entire imaging of spine is ideal
Focused CT imaging can miss clinically unapparent lesions Myelography and MRI are better than plain X-Rays, bone scans and CT for diagnosis

82
Plain Spine Radiographs
Easiest and cheapest Need large bony destruction or vertebral collapse to be diagnostic High false negative rate Not recommended to confirm diagnosis

83
MRI vs. CT Myelography

84
Both image thecal sac and display indentation and encircling
CT myelography involves a lumbar puncture Contraindicated in brain metastases, thrombocytopenia, or coagulopathy Can diagnose leptomeningeal metastases Available in Winnipeg in middle of the night

85
MRI Images whole spine High detail Spares lumbar puncture
Patients in pain must lie still

86
Roughly equivalent in terms of sensitivity and specificity
Presently no large comparative studies b/c MRI in the US has become so readily available MRI standard of care in centers that have access

87
Bone Scan More sensitive than plain radiograph
Visualizes entire skeleton Can miss neoplasms that do not have increased blood flow

88
CT Scan alone Does not visualize spinal cord and epidural space clearly

89
Intramedullary Metastases
Less common Often present with hemicord symptoms Unilateral weakness below lesion Contralateral diminution of pain and temperature sensation Can progress to bilateral dysfunction

90
Radiation Myelopathy Can mimic ESCC MR imaging can make distinction

91
MRI of epidural spinal cord compression in a women with past history of breast cancer.

92
Treatment

93
Treatment delays……. 2 month median delay in treatment from onset of back pain11 14 day delay in treatment from onset of neurological symptoms11

94
Why the delay? EDUCATION Patient factors General practitioner factors
Hospital factors EDUCATION

95
Treatment Objectives Pain control Avoidance of complications
Preserve or improve neurological function

96
Pain management Corticosteroids Opiates Decrease edema
Needed to decrease pain for comfort and examination purposes

97
Bed Rest No

98
Anticoagulation Cancer is a hypercoaguable state
High burden of tumor in metastatic disease Possible value in prophylaxis against venous thromboembolism If patient not mobile subcutaneous heparin or compression devices is indicated

99
Prevention of Constipation
Factors Autonomic dysfunction Limited mobility Opiate analgesic Risk of perforation Masked by corticosteroids Bowel regimen needed

100
Corticosteroids

101
Part of standard regimen Limited data on benefit vs. side effects
Many studies suggesting lower doses can be effective No randomized trials

102
Corticosteroid Recommendations
High dose dexamethasone and half dose every three days Pain with minimal neurological dysfunction can have lower dose Small asymptomatic lesions can forgo steroids

103
Radiation Therapy

104
Definitive choice Portal 8 cm wide Centered on spine Extends one to two vertebral bodies above and below the epidural metastasis

105
Relieves pain in most cases
Post-neurological function usually determines response Response most associated with tumor type and radiosensitivity; eg. lymphoma Dosing 20 to 40 Gy in 5 to 20 fractions Popular 30 Gy in 10 fractions

106
Surgery Changing role Historically posterior vertebral decompression was done No survival benefit with or without radiation15 15. Findlay, GF. Adverse effects of the management of malignant spinal cord compression. J Neurol Neurosurg Psychiatry 1984; 47:761.

107
Better techniques today allow aggressive approach
Gross spinal tumor resection with vertebral reconstruction now possible Experienced surgeon required

108
Improvement in surgery+rads
Recent controlled trial comparing aggressive surgery followed by radiation vs. radiation alone16 Improvement in surgery+rads Days remained ambulatory (126 vs. 35) Percent that regained ambulation after therapy (56% vs. 19%) Days remained continent (142 vs. 12) Less steroid dose, less narcotics Trend to increase survival 16. Patchell, R, Tibbs, PA, Regine, WF, et al. A randomized trial of direct decompressive surgical resection in the treatment of spinal cord compression caused by metastasis (abstract). proc Am Soc Clin Oncol 2003; 22:1.
 Percent that regained ambulation after therapy (56% vs. 19%) Days remained continent (142 vs. 12) Less steroid dose, less narcotics. Trend to increase survival. 16. Patchell, R, Tibbs, PA, Regine, WF, et al. A randomized trial of direct decompressive surgical resection in the treatment of spinal cord compression caused by metastasis (abstract). proc Am Soc Clin Oncol 2003; 22:1.")
109
Chemotherapy Can be successful in chemosensitive tumors
Hodgkin’s lymphoma Non-Hodgkin’s lymphoma Neuroblastoma Germ cell Breast cancer (hormonal manipulation) Prostate cancer (hormonal manipulation)
 Prostate cancer (hormonal manipulation)")
110
Bisphosphonates Recommended
Decrease pathologic fractures in bony disease Multiple myeloma Breast cancer

111
Prognosis Median survival with ESCC is 6 months14
Ambulatory patients with radiosensitive tumors have the best prognosis 14. Sorensen, PS, Borgesen, SE, Rohde, K, et al. Metastatic epidural spinal cord compression. Results of treatment and survival. Cancer 1990; 65:1502.

112
Treatment Delay Education EXPERIENCE

113
Case 3: Mrs. HC ID: 75 year old female living alone with no significant past medical history EC: brought to ER by paramedics after neighbor called b/c she was found in her apartment unresponsive No collateral history

114
Examination Fluctuating level of consciousness Vitals normal, no fever
Dehydrated Coarse upper airway sounds No other pertinent findings

115
Investigations CBC normal Mildly elevated BUN and Cr Normal LFTs
Standard electrolytes normal

116
Concern of pneumonia Chest x-ray ordered……

117
Multiple Pulmonary Metastasis

118
Calcium checked 4.5

119
Hypercalcemia

120
Symptoms Usually nonspecific
Many times patients present with very high calcium level Most research done in hyperparathyroidism

121
Gastrointestinal Constipation is most common15 Anorexia
Exacerbated or confused with narcotic effects Related to autonomic dysfunction Anorexia Vague abdominal pain Rarely can lead to pancreatitis 15. Heath, H 3d. Clinical spectrum of primary hyperparathyroidism: Evolution with changes in medical practice and technology. J Bone Miner Res 1991; 6(Suppl 2):S63.
:S63.")
122
Renal Dysfunction Nephrolithiasis Nephrogenic diabetes insipidus
More common in hyperparathyroidism Nephrogenic diabetes insipidus Defect in concentrating ability Polyuria and polydipsia Chronic renal failure Longstanding high calcium Calcifcation, degeneration, and necrosis of tubules

123
Neuropsychiatirc Anxiety Depression Cognitive dysfunction Delerium
Psychosis Hallucinations Somnolence Coma

124
Cardiovascular Short QT interval Supraventricualr arrhythmias
Ventricular arrhythmias

125
Physical Findings Usually not specific
Dehydration secondary to diuresis caused by the hypercalcemia Corneal deposition of calcium “band keratopathy” on slit lamp exam

126
Epidemiology Occurs in about 10 to 20% of patients with cancer
Both solid tumors and leukemias Most common Breast Lung Multiple myeloma

127
Pathogenesis

128
Three mechanisms Osteolytic metastases with local cytokine release
Tumor secretion of parathyroid hormone-related protein (PTHrP) Tumor production of calcitriol
 Tumor production of calcitriol.")
129
Osteolytic Metastases

130
Non-small cell lung cancer Cytokines released
Breast cancer Non-small cell lung cancer Cytokines released Tumor necrosis factor Interleukin-1 Stimulate osteoclast precursor differentiation into mature osteoclasts Leading to more bone breakdown and release of calcium

131
PTH-Related Protein Most common in patients with non-metastatic tumors
Called humoral hypercalcemia of malignancy Secretion of PTH itself is a rare event PTHrP binds to same receptor as PTH and stimulates adeynylate cyclase activity Increased bone resorption Increases kidney calcium reabsorption and phosphate excretion

132
Calcitriol Hodgkin’s disease (mechanism in majority)
Non-Hodgkin’s (mechanism in 1/3) Usually responds to glucocorticoid therapy
 Usually responds to glucocorticoid therapy.")
133
Diagnosis

134
Clinical symptomology with
History of cancer Risk factors for cancer Suppressed PTH Some centers can test for PTHrP to confirm Dx of humoral hypercalcemia High PTHrP may predict response to pamidronate16 Less of a response 16. Gurney, H, Grill, V, Martin, TJ. Parathyroid hormonerelated protein and response to pamidronate in tumourinduced hypercalcemia. Lancet 1993; 341:1611.

135
Malignancy must be ruled out in patients that present with a very high calcium and no other obvious cause

136
Treatment

137
Aims Lower serum calcium concentration Treat complications if present
Treat underlying disease

138
Volume Large volume of normal Saline administration
Expands intravascular volume Increases calcium excretion Inhibition of proximal tubule and loop reabosrption Reduces passive reabsorption of calicum Follow fluid status b/c of danger of fluid overload

139
Inhibition of Bone Resorption
Three therapies Calcitonin Bisphosphonates Gallium nitrate Historical therapy Antitumor antibiotic plicamycin (mithramycin) Multiple serious side effects No longer manufactured
 Multiple serious side effects. No longer manufactured.")
140
Calcitonin Salmon calcitonin Increases renal excretion of calcium
Decreases bone reabsorption by interfering with osteoclast maturation Weak agent Works the fastest

141
Bisphosphonates Adsorb to the surface of bone hyroxyapatite
Interfere with osteoclast activity Cytotoxic to osteoclasts Inhibit calcium release from bone Three commonly used Pamidronate Zoledronic acid Etidronate (1st generation, weaker)
")
142
Bisphosphonates More potent than calcitonin
Maxium effect occurs in 2 to 4 days Trend to use of IV zoledronic acid in the acute situation Both are can be renal toxic More potent than pamidronate Administered over a shorter period of time (15 minutes vs. 2 hours)
")
143
Prophylactic Bisphosphonates
Pamidronate use in patients with known lytic lesions17 Less episodes of hypercalcemia Less pathologic fractures Less pain Less spinal cord compression Less need for radiation or surgery 17. Hortobagyi, GN, Theriault, RL, Porter, L, et al for the Protocol 19 Aredia Breast Cancer Study Group. Efficacy of pamidronate in reducing skeletal complications in patients with breast cancer and lytic bone metastases. N Engl J Med 1996; 335:1785.

144
Newly discovered side effect…
Osteonecrosis of the jaw Recent case reports of jaw bone necrosis in patients on pamidronate EDUCATION needed

145
Gallium Nitrate Effective More potential for nephrotoxicity
Rarely used

146
Dialysis Last resort Dialysis fluid with little or no calcium is effective Useful when patients can’t tolerate large volume resuscitation If calcium needs to be correct emergently

147
Recommendations in symptomatic situation
Volume expansion Salmon calcitonin IV zoledronic acid or pamidronate Close follow up of calcium level and symptoms

148
Transitions in Treatment

149
Chemotherapy Two roles Direct treatment of cancer
Palliation of symptoms

150
Palliative Chemotherapy
Goal is not cure Goals Control of tumor Preservation of function Help tumor symptoms Pain Dsypnea Pruritis Poor appetite Weight loss

151
Fine Balance Chemotherapy can be very toxic
Ratio: benefit vs. toxicity Host factors and tumor factors Delicate balance in palliative situation Want medications that affect tumor but do not heavily affect host

152
Psychology of Cancer Psychological evolution during cancer treatment
Many people have fought very hard with their disease Chemotherapy for “relief” not “cure” can be difficult concept for patients ART of medicine

153
Evolution Chemotherapeutic protocols that have less side effects
molecular targeted therapies Attack tumor specifically Less effect on host

154
Breast cancer Colon Cancer Prostate cancer Lung cancer

155
Breast Cancer Aromatase inhibitors for ER positive tumors
Anastrozole, Letrozole, Exemestane Trastuzumab (Herceptin) Humanized monoclonal antibody targeting Her-2/neu protein on breast cancer cells Inhibits growth factor signal transduction Tolerated quite well
 Humanized monoclonal antibody targeting Her-2/neu protein on breast cancer cells. Inhibits growth factor signal transduction. Tolerated quite well.")
156
Colon Cancer Capecitabine (Xeloda)
Oral drug that is transformed into 5-FU with three enzymatic reactions Final enzyme is at higher levels in tumor cells Contributes to drug’s less toxic side effect profile Less stomatitis, less myelosupression

157
Targeted GI Therapies Bevacizumab Cetuximab
Monoclonal antibody to vascular endotheial growth factor receptor Some cardiac toxicity Cetuximab Monoclonal antibody to human epidermal growth factor receptor Skin toxicity

158
Prostate Cancer LHRH analogues Leuprolide (Lupron) Goserelin (Zoladex)
Stop testosterone production with limited side effects

159
Lung Cancer In stage IV disease patients who receive Cisplatin based doublet chemotherapy live longer and feel better than best supportive care Hard to balance side effects

160
Gefitinib (Iressa) Targets epidermal growth factor receptor (tyrosine kinase small molecule inhibitor) May have a role in the palliation of advanced non small cell lung cancer patients

161
Palliative Care Debate
Do not accept any patient on “active” therapy This needs to be further elucidated Patients being palliated with chemotherapy or targeted therapies still have other palliative care issues and needs Should a patient still on Xeloda for breast or colon cancer not be admitted to St. Boniface 8A?

162
Thank you

163
Any questions?

Similar presentations






















 Monday – Friday 8am – 4pm Bleep: 946 T: 020 8401 3000 x5726 F: 020 8401 3513 Dr Nicola Beech Dr Jillian Noble Dr Susannah.>")