Download presentation
Presentation is loading. Please wait.

3
Development-Knowledge Transfer Survey results over time: Recognition of CCGC name was 49-50% in 2002 moving up to 74% by 2003 Ranking of most useful guidelines: 2002: Diabetes, Depression, Asthma 2003: Colorectal, Pediatric Immunizations, Diabetes 2009 (May): Asthma, Gestational Diabetes, SBIRT Sustained interest in having CCGC continue to: –Develop guidelines –Convene stakeholders –Help practices prepare for systems change
: Asthma, Gestational Diabetes, SBIRT Sustained interest in having CCGC continue to: –Develop guidelines –Convene stakeholders –Help practices prepare for systems change")
4
EVALUATE

5
Guideline Uptake Survey published in Critical Pathways in Cardiology (June, 2008) Guideline use before and after dissemination: rates varied between 42.9% and 51.2%
 Guideline use before and after dissemination: rates varied between 42.9% and 51.2%")
6
Implementation-systems integration Rapid Improvement Activity (RIA) Fit Now Results: By 12 months participants had lost, on average 11.3 pounds when compared to baseline weight (p<.01, 95% CI: 4.3;18.4 pounds) which corresponds to a 5.6% loss of original body weight. Changes between 6 and 12 months were not significant.

7
TOTAL ENROLLMENT REFERRALS CURRENT ENROLLMENT REFERRALSCounty 21 Adams 6737 Garfield 00 Lincoln 00 Larimer 3016 Alamosa 3523 Alamosa 84 Summit 41 Weld 1410 Kiowa 00 Baca Fit Now Colorado RIA Sites by County: Referrals/Enrollment 92 Patients enrolled

10
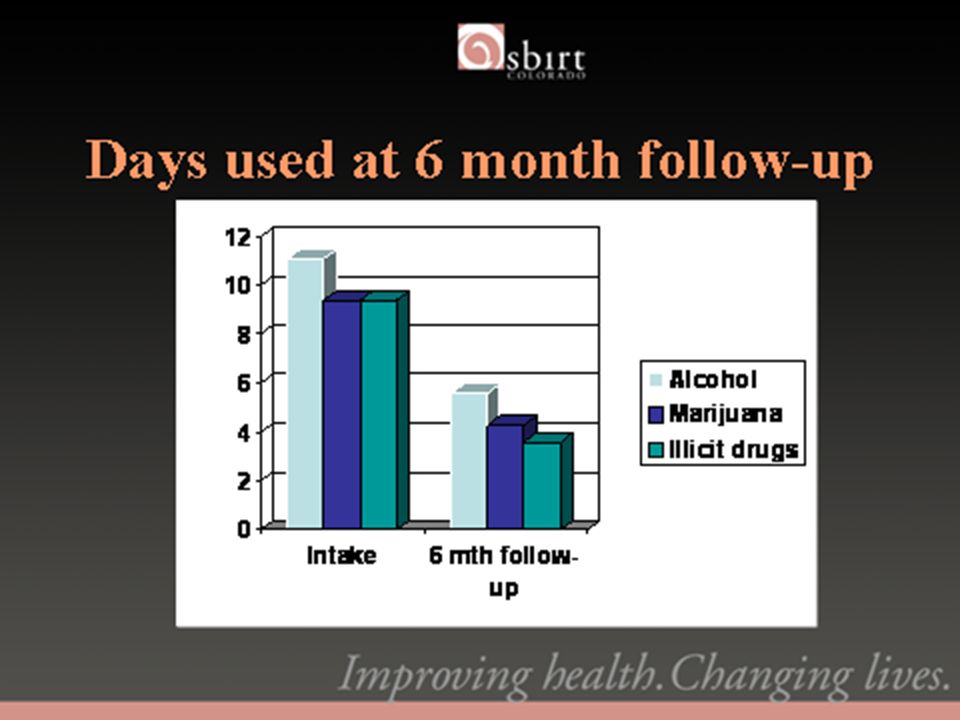
SBIRT Colorado Progress to Date 46,598 patients screened 54% of patients scored in low or no risk category 29% scored at risk for tobacco only 12% scored in moderate risk category (BI) 2% scored in high moderate risk category (BT) 3% scored in high risk category (RT)
 2% scored in high moderate risk category (BT) 3% scored in high risk category (RT)")
12
Pneumococcal Immunization Rates

15
CCGC Tobacco Program June 9, 2009

16
Co-Directors: Alison Long, MPH Michele Patarino, MBA, MSHA Project Managers: Debbie Dion Emily Gingerich CCGC Tobacco Team

17
Tobacco Program Overview

19
Show Me The Data InterventionParticipationQuitLineSelf Report Chart Audit/ registry or EMR Additional data CME X TRIA XXX TRIA with IPIP XXXX Mini-grants XXXX Grants xxXXX

20
Tobacco Program Provider Participation 6 www.coloradoguidelines.org/tobacco

21
Grants to Healthcare Organizations

22
MedSouth 8 www.coloradoguidelines.org/tobacco

23
Grants to Healthcare Organizations InterventionParticipationQuitLineSelf Report Chart Audit/ registry or EMR Additional data CME X TRIA XXX TRIA with IPIP XXXX Mini-grants XXXX Grants xxXXX

24
Tobacco Rapid Improvement Activity (TRIA)
")
25
TRIAs Examples of Practice Changes Following the TRIA WHATWHOHOW ASK about tobacco status Intake nurse or MAIntake form – add Do you use tobacco? Add Tobacco Use tab in EMR Amend vital sign stamp to include smoking status ADVISE to quit RN, NP, PA, MDProvider is prompted to advise patient to quit b/c of chart documentation or b/c QL fax form is on chart REFER for help RN, NP, PA, MD or staff cessation specialist QuitLine referral materials (brochures, fax forms, prescription pads) are available in exam rooms
 are available in exam rooms.")
26
Tobacco Rapid Improvement Activity (TRIA) InterventionParticipationQuitLineSelf Report Chart Audit/ registry or EMR Additional data CME X TRIA XXX TRIA with IPIP XXXX Mini-grants XXXX Grants xxXXX
 InterventionParticipationQuitLineSelf Report Chart Audit/ registry or EMR Additional data CME X TRIA XXX TRIA with IPIP XXXX Mini-grants XXXX Grants xxXXX")
27
TRIA Results 15 www.coloradoguidelines.org/tobacco

28
IPIP Tobacco Measures

29
Additional Data Source: Colorado QuitLine 1-800-Quit-Now

30
RIA Flyers

31
Questions? VISIT: www.coloradoguidelines.org/tobacco Email: tobaccoinfo@coloradoguidelines.org CALL: 720/297-1681 www.coloradoguidelines.org/tobacco tobaccoinfo@coloradoguidelines.org

32
Boulder, Colorado http://sprucestreetinternalmedicine.com

33
Hillary Browne, MD, FACP Colorado Practice Coaches: Debbie Barnett & Deb Maltby Improving Diabetes Care Start date: January 2007 Number of diabetes patients in the registry: ~250

34
Description of Practice Boulder, Colorado 3500-4000 active patients, 5% Medicare 3.5 full time equivalent providers Aim: to provide excellent, comprehensive diabetes care; NCQA certification Staff: Manager, Phone receptionist, 2 front office, 4 MAs, 4 file clerks, part time dietician. Quality improvement team: 1 front office, 1 back office (MA), office manager, 2 providers, QI coach
, office manager, 2 providers, QI coach.")
35
Data collection Reach My Doctor (RMD): portal with diabetes and asthma registries Special features we use: –Care plan/flow sheet –labs automatically populate flow sheets –email reminders –labs can be emailed with our comments –patients can view their care plans
: portal with diabetes and asthma registries Special features we use: –Care plan/flow sheet –labs automatically populate flow sheets – reminders –labs can be ed with our comments –patients can view their care plans")
36
Planned care at Spruce Street … how it works Registry Protocols –Patient makes appointment and DM goes on the schedule –File clerk pulls the chart (red dot) and prints the flow sheet –MA notes that patient has DM and removes patients shoes –If annual sensory exam is due, she performs and documents the exam –Visit with provider focuses on flow sheet, which is given to patient at the end of the appointment –Self-management goals and reminder
 and prints the flow sheet –MA notes that patient has DM and removes patients shoes –If annual sensory exam is due, she performs and documents the exam –Visit with provider focuses on flow sheet, which is given to patient at the end of the appointment –Self-management goals and reminder")
38
Retinal Exams 6/07 to 5/086/08 to 5/09

39
Adopting a clinical protocol: overcoming provider insulin resistance! Registry enabled us to clearly identify patients with hgb AICs > 9 Leading to a conscious decision to relearn insulin regimens to achieve better glycemic control MAs now trained to teach patients to administer insulin and monitor blood sugars

40
Spruce Street Internal Medicine A1c > 9 6/07 to 5/08 5/08 to 4/09

41
Spruce Street Internal Medicine A1c < 7 6/07 to 5/08 5/08 to 4/09

42
Spruce Street Internal Medicine BP < 130/80 6/07 to 5/08 5/08 to 4/09

43
Spruce Street Internal Medicine BP < 140/90 6/07 to 5/08 5/08 to 4/09

44
Spruce Street Internal Medicine LDL < 100 6/07 to 5/085/08 to 4/09

45
Spruce Street Internal Medicine Kidney Assessment 6/07 to 5/08 6/07 to 5/08 6/08 to 5/09

46
Spruce Street Internal Medicine Flu Vaccine 6/07 to 5/08 6/08 to 5/09

47
Spruce Street Internal Medicine Foot Exams 6/07 to 5/086/08 to 5/09

48
Sustainable improvement Routine protocols with immediate correction if not followed Staff feels responsible and integral to successful patient outcomes Patients develop stronger connections with ancillary staff Ultimate outcome is improved satisfaction for patients and staff

49
Next steps Focus on high-risk patients (hgbAiC > 9) Challenge ourselves to attain goals on individual diabetes measures. Asthma registry initiated Move forward with plan include COPD and heart/stroke Coordinate timely office follow up after hospitalization to prevent readmission.

50
Thank you To all of our providers and staff for their exceptional performance And to Allyson Gottsman, Associate Director, and Marjie Grazi Harbrecht, MD, Medical/Executive Director of the Colorado Clinical Guidelines Collaborative

51
LDL in control Chet Cedars Lone Tree Family Practice

52
Two physicians and two nurse practitioners One physician spends ½ time in clinical work and ½ time in practice management. One nurse practitioner spends ½ time clinical work and ½ time as Care Manager. (three FTE) Use Allscripts/Misys EMR with imbedded orders in Preventive Health Module based on sex, age and diagnosis. Query Reports to pull patient lists based on Dx and other clinical data.
 Use Allscripts/Misys EMR with imbedded orders in Preventive Health Module based on sex, age and diagnosis. Query Reports to pull patient lists based on Dx and other clinical data..")
53
Patients with 1 LDL in last 12 months

54
LDL < 100

55
System that Underpins Performance LDL at Target LDL measured appropriate intervals Intervention s when not at target Sustaining activities when at target Appropriate follow up Improvements can be applied at any point to make the system perform better

56
To improve timely LDL measurements: Print list of patients with LDL >100 – Mailing labels for outreach Last LDL date and value available at time of service Informal provider consensus regarding how often to measure assists with consistent messaging to patients

57
Interventions to Help Patients Achieve LDL Target Lab values auto imported to diabetes tab, including LDL Informal consensus among providers regarding management Aggressive follow up Print out of trends from PHP registry Guidelines and targets shared with patients Provider directed self management strategy Some assistance with DAPs for Rx as needed

58
Sustaining Activities when at Target Periodic re-measurement Reinforcement of care plan Positive reinforcement with trending graphs

59
Appropriate Follow Up Aggressive follow up encouraged Patients engaged in progress toward goal Patients recognize ongoing follow up essential for optimal outcomes

60
Still working on… Strategy to get patients in based on last date of LDL More data points auto populated for diabetes care parameters Continuing process to eliminate double data entry Documentation of self management goals

61
Improving Performance in Practice - Evaluation Data June, 2009 Perry Dickinson

62
Elements Registry data – performance measures Assessment of Diabetes Management (clinician survey) Patient data from trial practices Qualitative data from practice interviews Chart audit data for trial practices – coming soon In slides: ** means p<.01, * means p<.05, + means nearing significance
 Patient data from trial practices Qualitative data from practice interviews Chart audit data for trial practices – coming soon In slides: ** means p<.01, * means p<.05, + means nearing significance")
63
Diabetes Process Measures

64
Diabetes Outcome Measures

65
Asthma Measures

66
Patient Measures Only those 11 practices involved in the randomized clinical trial Patients recruited from a list of diabetic patients provided by practice Same patients at baseline, 9, 18 months 244 patients at baseline, 235 at 9 months 18 month f/u data soon! Patient self report regarding various aspects of their diabetes care

67
Checked in Past 12 Months

68
Overall Diabetes Process of Care Process – A1c, urinary protein, cholesterol, eye exam, foot exam done over past year SMS – Self- Management Support - Dietary counseling, goal setting, home glucose monitoring dealt with over past year Total = checks + PSMS

69
Clinician Survey Assessment of Clinician Diabetes Management (ACDM) – designed to measure the level of implementation of elements of the Chronic Care Model 42 practices; 181 clinicians at baseline, 80 post-intervention
 – designed to measure the level of implementation of elements of the Chronic Care Model 42 practices; 181 clinicians at baseline, 80 post-intervention")
70
ACDM

71
Qualitative Data Interviews of key informants (lead physician, practice manager, key staff) from 8 IPIP practices regarding issues around their diabetes improvement efforts through IPIP All practices had engaged to the point of reporting measures Qualitative interviews of the trial practices are in progress
 from 8 IPIP practices regarding issues around their diabetes improvement efforts through IPIP All practices had engaged to the point of reporting measures Qualitative interviews of the trial practices are in progress")
72
Practices Interviewed Six from Denver metropolitan area, one from Pueblo, and one from Colorado Springs Ranged from three to seven clinicians, Three belonged to an IPA in the Denver area, two to other IPAs, and three were independent Primarily family medicine, with one internal medicine

73
Clinical Changes Practices all implemented mechanisms to identify and track their patients with diabetes Most used flow sheets to assist with data management and point of care decision support – key in organizing care Virtually all developed a distinguished diabetic visit- helped focus visit activities Most expanded MAs activities, including screening questions, assessment and performance of needed labs or services Many developed patient recall systems to bring patients in when visits and services were due.

74
Barriers The major barrier was time Substantial financial costs – mostly personnel Insufficient staff It is hard to have more than one person in the practice trained and up to speed on doing this, and they tend to be upwardly mobile. Staff and clinician turnover an issue Problems getting information from consultants

75
IT Barriers Duplication of effort in data entry a huge issue, especially in practices with EHR Lack of ability to enter data once and have it show up in the appropriate places for administrative, clinical, and quality data reporting and use Often easier for practices without an EHR to implement a registry Practices with paper charts - charts not always available, time spent tracking them down.

76
Benefits Improved quality of care Power of having better data for managing patients. Possibility of financial benefit through bonuses, pay- for-performance, higher coding, group visits, and bringing patients in for services Improved organization and efficiency of work flow Improved morale for clinicians Greatly improved staff satisfaction Staff more engaged and invested in the practice -felt like they were more an important part of patient care

77
Colorado April 2008 v March 2009

78
Measures reported – March 2008 Measures reported – April 2009

Similar presentations







 Pilot population.>")


















