Download presentation
Presentation is loading. Please wait.

2
Common Anorectal Diseases
Lecturer: Professor Saleh M. AlSalamah FRCS Professor of Surgery & Consultant General and Laparoscopic Surgeon College of Medicine, King Saud University, Riyadh, KSA.

3
References Clinical Surgery by Michael M. Henry
Bailey and Love’s Short Practice of Surgery Essential of General Surgery by Peter F. Lawrence

4
Objectives At the end of this presentation students will be able to:
Understand the surgical anatomy of the anal canal. Classification, pathogenesis and management of hemorrhoids. Pathogenesis, presentation and management of anal fissure. Presentation. Classification and management of perianal abscess. Classification and management of anal fistula. Pathogenesis, presentation and management of anal carcinoma.

5
Anorectal Diseases Overview Surgical Anatomy Examination of the Anus
Common Anal Conditions

6
Overview Anal and perianal disorders makeup about 20% of all outpatient Surgical referrals. These conditions are extremely distressing and embarrassing patient often put up with symptoms for long time, before seeking medical care.

7
Common symptoms Anal bleeding Anal pain and discomfort
Perianal itching and irritation Something coming down perianal discharge

8
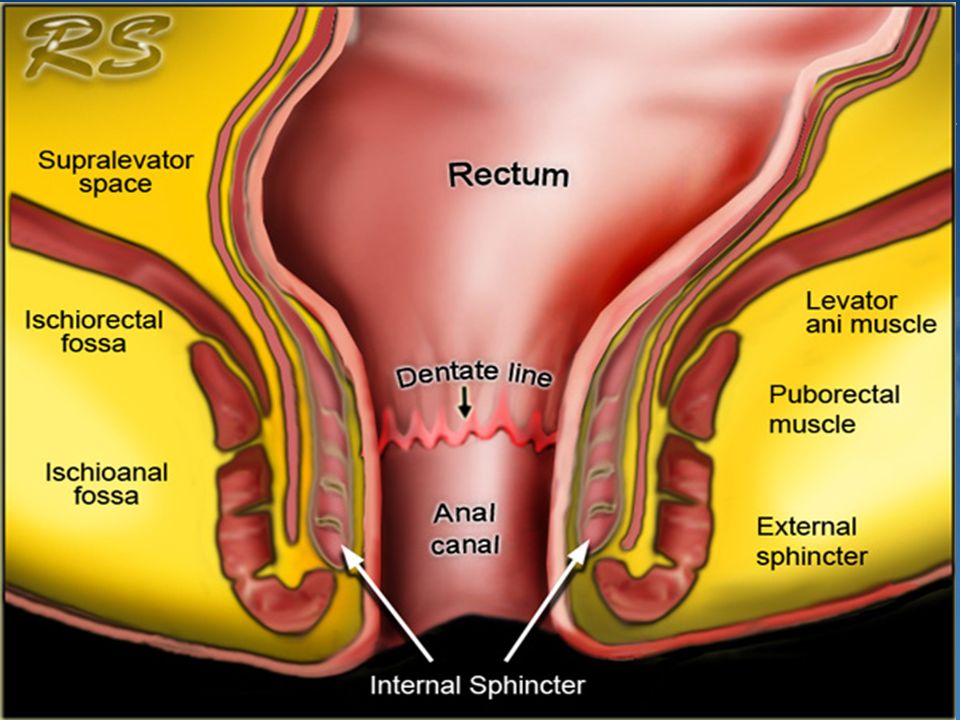
Surgical Anatomy The anal canal 1.5” (4 cm) long and is directed downward and backward from the rectum to end at the anal orifice. The mid of anal canal represents the junction between endoderm and ectoderm

11
Surgical Anatomy The lower ½ is lined by squamous epithelium and the upper ½ by columnar epithelium so carcinoma of the upper ½ is adenocarcinoma. Where as that arising from the lower part is squamous tumour.

13
Surgical Anatomy The blood supply of upper ½ of the anal canal is from the superior rectal vessels. Where as that of the lower ½ is supply of the surrounding anal skin the inferior rectal vessels which derives from the internal pudendal ultimately from the internal iliac vessels.

15
Surgical Anatomy The lymphatic above the mucocutaneous junction drain along the superior rectal vessels to the lumbar lymph nodes, where as below this line drainage is to the inguinal lymph nodes.

16
Surgical Anatomy The nerve supply to the upper ½ via autonomic plexus and the lower ½ is supplied by the somatic inferior rectal nerves terminal branch of the pudendal nerve. So the lower ½ is sensitive to the prick needle.

17
Anal Sphincter The internal anal sphincter of in voluntary muscle, which is the continuation of the circular muscles of the rectum. The external sphincter of the voluntary muscles, which surrounds the internal sphincter and comprises 3 parts (formerly) subcutaneous the lower most portion of the external sphincter superficial part deep part
 subcutaneous the lower most portion of the external sphincter. superficial part. deep part.")
19
Common Anal Conditions
Haemorrhoids Pruritus ani Perianal abscess Anal fissure Anal fistula Rectal prolapse Anal in continence Non malignant strictures Anal neoplasms

22
Examination of Anus This requires careful attention to circumstances (couch, light, gloves). The Sims (left lateral position) is satisfactory. The examination proceed by; inspection digital examination with index finger proctoscopy sigmoidoscopy
. The Sims (left lateral position) is satisfactory. The examination proceed by; inspection. digital examination with index finger. proctoscopy. sigmoidoscopy.")
24
Hemorrhoids Piles may be internal or external according to whether they are internal or external to anal orifice. The internal Haemorrhoids: They are dilation of the superior haemorrhoidal veins above the denate line each pile consists of mass of dilated vein, artery, some connective tissue and mucosal investment.

27
Hemorrhoids The location of piles, right anterior, right posterior and left lateral situated respectively 11, 7, 3 o’clock with patient in the lithotomy position, these are give daughter piles.

29
Etiology Primary Causes:
Hereditary factors e.g, structural weakness of the vein. Anatomical factors. Partial congestion. Chronic constipation. Sphincteric relaxation.

30
Etiology Secondary Causes: venous obstruction straining on micturation
pregnancy venous obstruction straining on micturation venous congestion carcinoma of the rectum

31
Clinical features Bleeding at defecation Prolapse
Discharge with pruritus ani Pain Thrombosed piles

32
Assessment and Diagnosis
Careful history Abdominal Examination Anorectal Examination Investigation e.g., proctoscopy

33
Complications Profuse haemorrhage Acute thrombosis

35
Treatment

36
Treatment Injection treatment Barron’s rubber banding Cryosurgery
Gabriel syringe is filled with sclerosant 5% phenol with almond oil Barron’s rubber banding Cryosurgery Co2 Laser Lord’s manual dilation

39
Hemorrhoidectomy

40
Stapled Hemorrhoidectomy

42
External Hemorrhoids Perianal Hematoma
Due to rupture of dilated anal vein as result of sever straining. Sudden onset of painful lump at the anus. Swelling tense & tender, bluish in colour covered with smooth shining skin.

43
External Hemorrhoids

44
Treatment Evacuation if the patient come within 48hours
If patient come late conservative treatment. If untreated the haematoma undergoes: resolution ulceration suppuration to forms in abscess fibrosis which give rise to skin tag.

45
Perianal Abscess The infection usually starts in one of the crypts of Morgagni and extends along the related anal gland to the intersphincteric plane where it forms as abscess. Soon it tracks in various directions to produce different types of abscesses .

46
Types of Abscess Perianal abscess (60%) Ischiorectal abscess (30%)
Sub mucous abscess (5%) Pelvirectal abscess
 Pelvirectal abscess.")
48
Perianal Abscess Patient with recurrent anorectal abscess always consider associated underlying diseases such as Crohn’s, UC, rectal cancer and active TB.

49
Perianal Abscess Symptoms Signs Treatment Acute pain High fever
Swelling Tenderness with induration Treatment Incision and drainage and covered by antibiotics.

50
Perianal Abscess

51
Fistula in ano Defined as track lined by granulation tissues, which connects deeply in the anal canal or rectum and superficially on the skin around the anus. It usually result from an anorectal abscess.

52
Fistula in ano Anal fistulas have well recognized association with crohn’s disease, UC, TB, colloid carcinoma of the rectum and lympho granuloma venercum.

54
Types of Anal Fistulas According to whether their natural opening is below or above the anorectal ring Low level e.g., subcutaneous, low anal, sub mucous. High level – open into anal canal at or above the anorectal ring e.g., high anal, pelvirectal

55
Park’s Classification
Inter sphincteric (70%) low level anal fistula Trans-sphincteric (25%) high level anal fistula Supra sphincteric fistulae (4%). Extra sphincteric (1%) rare type include the tract passes outside all sphincter muscles to open in the rectum.
 low level anal fistula. Trans-sphincteric (25%) high level anal fistula. Supra sphincteric fistulae (4%). Extra sphincteric (1%) rare type include the tract passes outside all sphincter muscles to open in the rectum.")
57
Good Sall's Rule Fistulas with external opening in relation to the anterior ½ of the anus tend to be direct type.

58
Clinical features Persistent discharge which irritates the skin and causes discomfort at the anus may be associated with pain. External opening may be seen with palpation the tracks is often palpable as cord.

59
Investigations Proctoscopy Radiology Biopsy

60
Surgery Fistulectomy

61
Always sent track for biopsy.

62
Seton placement

63
Anal Fissure Defined as longitudinal tear in the mucosa and skin of the anal canal. Commonly posterior midline more common in female than male.

64
Anal Fissure Lateral fissures are so rare there presence suggest specific lesions such as, Crohn’s disease, UC, TB or malignancy.

65
Etiology Tearing of the anal lining by over distension of the anal canal during passage of large scybalous mass (stool). Tearing of anal valve or fibrous polyps. Laceration of the anal canal by sharp FB. Excessive straining during child birth.

67
Anal Fissure The acute anal fissure if not treated becomes chronic anal fissures. As result secondary pathological changes may occurs: Chronicity A “sentinel” pile Hypertrophied anal papilla Contracture of the anus Suppuration

69
Clinical Features Pain during and after defecation. Constipation
Bleeding Discharge

70
Findings Fissure or ulcer distal to dentate line. Sentinel Tag
Hypertrophied papilla. Spasms of the internal sphincter

71
Treatment Conservative Treatment Stool softeners (laxative)
Sitz baths (10 – 15 mins.) Ointments & Suppository
 Ointments & Suppository.")
72
Treatment Surgical Treatment Dilation under anaesthesia (Anal Stretch)
Fissurectomy and dorsal sphincterotomy Lateral internal sphincterotomy

73
Anorectal Tumours Benign tumours Epithelial Tumours Anal warts (virus)
Juvenile polyp Adenomatous polyps Villous papilloma Familial polyposis Pseudo polyps Endometrioma

75
Anorectal Tumours Connective Tissue Tumours Fibrous polyp Lipoma Myoma
Haemangioma Benign Lymphoma

76
Malignant Tumours of the Anal Canal
The lesion is usually squamous cell carcinoma. Rarely adenocarcinoma, malignant melanoma or basal cell carcinoma.

77
Squamous cell carcinoma
5% of all anorectal malignancies. Arising from the stratified squamous epithelium of the lower ½ of the anal canal. It is disease of elderly. Squamous cell carcinoma more common in males. The aetiology of anal carcinoma unknown but chronic irritation or infection may be predisposing factors.

79
Clinical Features Localized ulcer or raised growth with irregular ulcerated surface. History of bleeding. History of pain with discomfort. Tenesmus with incontinence. Discharge.

80
Examination On palpation squamous carcinoma feels hard and woody due to invasion of perianal tissues. P/R examination may prove impossible because of stenosis or discomfort. Inguinal LN are examined carefully as they receive lymph from the lower anal canal and perianal region and may be the site of metastasis.

81
Treatment Above the pectinate line Abdomino perineal excision
Below the pertinate line local excision. If inguinal LN metastasis present should be removed by block dissection.

82
Treatment Late cases Palliative colostomy. Radiotherapy.

83
Rare Malignant Anal Tumours
Adenocarcinoma Basal cell carcinoma Malignant melanoma

84
Benign strictures Stricture of the anus and rectum may be: Congenital
Postoperative Inflammatory

85
Clinical features Progressive difficulty in defecation
In cases of inflammatory strictures Bleeding Discharge Tenesmus Late cases subacute intestinal obstruction

86
Diagnosis Rectal examination reveals the location type and degree of the stenosis. Proctoscopy Biopsy

87
Treatment Dilation Superficial external proctotomy

88
Thanks

Similar presentations