Download presentation
Presentation is loading. Please wait.

1
Brian S. Parsley, MD 2 nd Vice President AAHKS Clinical Associate Professor Baylor College of Medicine Houston, Texas

2
2 nd VP for AAHKS Orthopaedic Surgeon in Private Practice Strong Patient Advocate

3
The PATIENT We Want to Get It Right Outline the Rules and We Will Follow Them! We Want to Maintain Access to Care for Our Patients. We are in this Together!

4
Medicare receives over 1.2 Billion claims per year. This equates to: 4.6 million claims per work day, or 575,000 claims per hour 9,580 claims per minute 160 claims per second

5
MAC: Medicare Administrative Contractor. US is split into ten regions for purposes of Medicare claims administration. MACs are private companies that serve as contractors performing claims administration for Medicare. Each MAC has some level of latitude in the interpretation and application of the rules based on regional determinations. CERT: Comprehensive Error Rate Testing. CERT audit program is designed to monitor the performance of MACs and to ensure that they are administering claims properly. CERT audits result in annual reports of the rate of improper payments made to hospitals. A high error rate for a particular procedure on the Part A hospital side may lead to increased scrutiny of Part B physician claims.

6
RAC: Recovery Audit Contractor. A RAC is an independent medical collection agency that works for Medicare to review overpayments and underpayments to providers. RACs are paid 9-12.5% contingency fees for the overpayments they recover. RACs have the ability to analyze claims with payment dates reaching as far back as October 1, 2007. LCD: Local Coverage Determination. MACs define LCDs for different procedures. The LCD tells you what Medicare will cover in its MAC jurisdiction. For example, they define what constitutes medical necessity for a specific procedure, and no procedure will be covered if it is not found to be medically necessary. Failure to follow the requirements of an LCD will result in an overpayment, which could be sought after an audit and refunded to CMS.

8
MACs have always had the authority to audit claims in order to reduce their CERT error rates. In late 2011, at least three MACs initiated audits that targeted specific orthopaedic procedures with high error rates in their jurisdictions. MAC Audits have looked at documentation requirements of non-surgical interventions prior to total joint replacement. MAC has launched a prepayment audit program affecting orthopaedic codes, including those for total joint replacements in Florida. if problems are found with the Part A claims, then payment will be denied, and the MAC may then perform a post-payment audit of the Part B physician services claims related to the problematic Part A claims and deny payment.

10
Goals set by President Obama: To reduce the Medicare FFS improper payment rate from 12.4% to 8.5% by Nov 2011 and 6.2% by Nov 2012. Identifying past improper payments through data analysis. (Audits) Correcting past and improper payments through post pay review. (Audits) Preventing future improper payments through provider education.
 Correcting past and improper payments through post pay review. (Audits) Preventing future improper payments through provider education..")
12
Is it fraud? (Intentional falsification or deceit to obtain payment) Is it abuse? (CMS: when doctors or suppliers do not follow good medical practices that can result in unnecessary costs to Medicare) Is it a pattern of disregard for regulations? OR Is it hospitals and physicians providing appropriate care to their patients but unable to comply with a myriad of confusing, vague technical Medicare documentation and billing rules despite their good intentions? How does CMS tell the difference? How do providers protect themselves?
 Is it a pattern of disregard for regulations. OR Is it hospitals and physicians providing appropriate care to their patients but unable to comply with a myriad of confusing, vague technical Medicare documentation and billing rules despite their good intentions. How does CMS tell the difference. How do providers protect themselves .")
13
ALL FRAUDULENT CLAIMS ARE IMPROPER PAYMENTS BUT ALL IMPROPER PAYMENTS ARE NOT FRAUDULENT CLAIMS!!!!! MOST ARE DUE TO IMPROPER DOCUMENTATION!

14
Improper payments: est. 3% to 10% of total healthcare expenditures nationally. Improper Payment Elimination and Recovery Act 2010 (IPERA) - Signed by President Obama on 7/20/2010 FY 2010: Feds recovered more than $4 billion thru these enforcement efforts. $2.5 billion represented recoveries under the False Claims Act, the largest amount in the history of the DOJ. Affordable Care Act (ACA) provides tools for enhanced fraud prevention and prosecution.
 - Signed by President Obama on 7/20/2010 FY 2010: Feds recovered more than $4 billion thru these enforcement efforts. $2.5 billion represented recoveries under the False Claims Act, the largest amount in the history of the DOJ. Affordable Care Act (ACA) provides tools for enhanced fraud prevention and prosecution..")
15
Repository of all Medicare claims All Medicare auditors have access to Medicare Data Warehouse Data mining at will for Parts A, B, C, D Auditors input results of reviews Red flag suspicious activities also alerts other auditors Public disclosure required by ACA ( the public will know that you or your hospital has been audited).
.")
16
The Cops PERM: Payment Error Rate Measurement Program (Medicaid and CHIP) MAC: Medicare Administrative Contractor (pays bills) CERT: Comprehensive Error Rate Testing (MAC payment errors) RAC: Recovery Audit Contractor (independent contractors) ZPIC: Zone Program Integrity Contractor (fraud) OIG: Office of the Inspector General (fraud) Medicaid RAC: Implementation January 2012 Cross referrals: Auditors talk to each other. Auditors required to refer suspicious activities for fraud investigations

17
Sixth National Medicare RAC Summit, November 8, 2011 Lessons for Providers from the First Year of ZPIC Audits Steve Lokensgard, Faegre & Benson LLP

19
The MAC pays all Medicare providers except for DME – allows claims matching. MACs Role in audit process Performs provider education Adjusts payments after CERT, RAC (and other audit) review Beginning Jan. 1, 2012 – Sends Demand Letter –Applies recoupments and corrects underpayments –Limited information on Demand Letter Supplies information to Data Warehouse Notifies RAC when account receivable is created –N432 remittance notice sent to hospital
 review Beginning Jan. 1, 2012 – Sends Demand Letter –Applies recoupments and corrects underpayments –Limited information on Demand Letter Supplies information to Data Warehouse Notifies RAC when account receivable is created –N432 remittance notice sent to hospital.")
20
Reviews conducted by clinicians (nurses, physical therapists, etc) and certified coders Pre pay review: Claims that are found to be improper are denied and no payment issued. Post pay claims that are found to be improper –overpayment is recouped –underpayment is paid back Suspected fraud: Referral for investigation

21
CERT evaluates MACs payment error rate Claims are randomly selected Post payment only CERT auditor reviews medical records Reviews conducted by at least one nurse Claims paid incorrectly are scored as errors No documentation error: Failure to submit record Insufficient documentation Lack of medical necessity Incorrect coding Other errors (duplicate payments / no benefit category / other billing errors)
")
22
Computes and reports error rates. Nationally By Contractor By Service By Provider Type CMS and contractors analyze MAC error rate data and develop Error Rate Reduction Plans Payments adjustments by CERT are referred to MAC Payment adjustments are made by MAC Appeals go to MAC Provides targets for future RAC issues

23
The RAC Audits have been implemented Recovery Audit Prepayment Review Demonstration Project is on the horizon

24
November 15, 2011: CMS announced a new Recovery Audit Prepayment Review Demonstration Project Auditors review Part A hospital claims after services are provided but before claims are paid to ensure that the provider complied with all Medicare payment rules. The reviews were targeted on seven states with high populations of fraud and error-prone providers (FL, CA, MI, TX, NY, LA, IL) and four states with high claims volumes of short inpatient stays (PA, OH, NC, MO) for a total of 11 states. FLA has been implemented
 and four states with high claims volumes of short inpatient stays (PA, OH, NC, MO) for a total of 11 states. FLA has been implemented.")
25
A meeting was held on Dec 27, 2011 with representatives from AAOS and AAHKS to discuss our concerns with this new initiative. Shortly after the meeting, CMS announced an indefinite delay in the January 2012 implementation, but it is anticipated that this program ultimately will be implemented.

26
You bettcha! It can affect the cost of borrowing It raises the costs to hospital It increases the cost of care Purchase of new equipment Maintenance of facility/ equipment Staffing ratios and salaries to attract good staff Marketing (information in the public domain)
.")
27
No! Physician payments are now coming under review. If the hospital is denied then you will be denied Physicians are now being audited directly

29
Comprehensive Error Rate Testing (CERT) Notice #14632 Followed CERT audit and denial of inpatient hip and knee replacements Affects Part A providers and physicians in Colorado, New Mexico, Oklahoma and Texas The CERT contractor stated that favorable audit findings would have required medical record documentation clearly demonstrating that the patient has end-stage joint disease and should have included evidence of prior failed conservative therapy. CERT Notice 14632

30
Documentation expected (physician, ARNP, RN, PT, OT) Preoperative joint examination findings showing end- stage joint disease requiring joint replacement. Peoperative significant loss of range of motion or joint deformity. Operative findings supporting end-stage joint disease, including bone-on-bone disease. Documentation that patient needed adaptive skills or an assistive device to maintain mobility. Preoperative radiographs showing end-stage joint disease. CERT Notice 14632

31
Including adequate history of the presenting illness in hospital record will improve the likelihood of Medicare payment of the hospital claim. It will also substantiate medical necessity for payment of physician services performed in conjunction with the hospital stay. Please note that statements such as, Failed outpatient therapy, admit for right total knee replacement, are simply not sufficient evidence of medical necessity for the admission or the surgery… Records must demonstrate end-stage joint disease with ongoing symptoms and functional limitation despite maximal appropriate conservative care… CERT Notice 14632

32
Records must demonstrate end-stage joint disease with ongoing symptoms and functional limitation despite maximal appropriate conservative care, and should include the following items from the medical record: Preoperative physician and therapist evaluations and treatment records. Preoperative X-rays showing end-stage joint disease. Operative findings supporting end-stage joint disease, including bone-on-bone disease. Documentation of patients functional limitations or need for adaptive behavior or use of assistive devices (e.g., canes, walkers, wheelchair). CERT Notice 14632
. CERT Notice")
33
CMS Wants to know what YOU are thinking Accurate and complete documentation in the physician records as well as the hospital records is the key A medical evaluation must be performed. The evaluation should include: clear documentation of the patients functional status documentation of the patients mobility and pain. evaluation may be done all or in part by the surgeon. the surgeon must sign off on the report and incorporate it into their records.

34
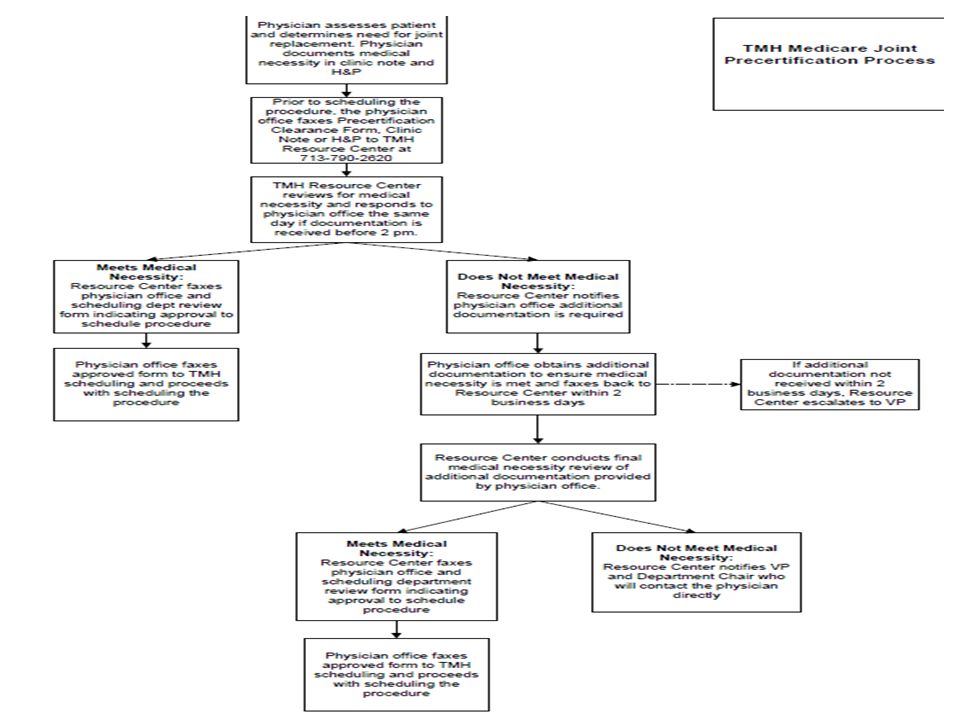
Pre certification and approval of DRG 470 patients prior to posting on surgery schedule Screening for sufficient data to justify surgery This effects both Medicare and commercial insurance patients

37
radiographic supported evidence (X-ray) or MRI supported evidence and pain or functional disability from injury due to trauma or arthritis of the joint and non-surgical medical management must have been tried and failed and such management must be clearly addressed in the pre-procedure medical record non-surgical medical management have been tried for a sufficient period (usually three months) to assess effectiveness. Treatment should include one of more of the following: anti-inflammatory medications analgesics flexibility and muscle strenghtening exercises supervised physicial therapy(DATE OF TREATMENTS???) activity restrictions as is reasonable assistive devices (canes, braces, etc.) weight reduction as appropriate therapeutic injections into the joint as appropriate
 activity restrictions as is reasonable assistive devices (canes, braces, etc.) weight reduction as appropriate therapeutic injections into the joint as appropriate.")
38
Chief Complaint: End stage osteoarthritis, right knee, for knee replacement. History: Patient has had bilateral osteoarthritis, gradually progressive over 10-15 years. Most recent X-ray (7/22/11), right knee shows joint space near obliteration along with marginal osteophytes and subchondral sclerosis. Has been treated as follows: Ibuprofen 400 mg QID since January; PT 3 x week from 3/15/11 to 6/30/11. Patient started using a cane in May. Right knee pain is continuous at level 3/10 with 6/10 on ambulation. Sometimes pain keeps him up at night. No longer able to climb the five steps to his front door. Knee pain and stiffness limit walking to less than 25 yards without resting. Physical Exam: Bilateral knee deformity consistent with severe osteoarthritis. Right knee reduced to less than 90 degrees. Unable to rise from a chair unassisted. Impression: Worsening pain, deteriorating range of motion and significant interference with function. Current therapy ineffective. Total Knee Replacement is only option for pain control and functional restoration. Orders: Admit to inpatient care for right TKR.
, right knee shows joint space near obliteration along with marginal osteophytes and subchondral sclerosis. Has been treated as follows: Ibuprofen 400 mg QID since January; PT 3 x week from 3/15/11 to 6/30/11. Patient started using a cane in May. Right knee pain is continuous at level 3/10 with 6/10 on ambulation. Sometimes pain keeps him up at night. No longer able to climb the five steps to his front door. Knee pain and stiffness limit walking to less than 25 yards without resting. Physical Exam: Bilateral knee deformity consistent with severe osteoarthritis. Right knee reduced to less than 90 degrees. Unable to rise from a chair unassisted. Impression: Worsening pain, deteriorating range of motion and significant interference with function. Current therapy ineffective. Total Knee Replacement is only option for pain control and functional restoration. Orders: Admit to inpatient care for right TKR..")
39
MUST be dictated for transcription within 24 hours Operative findings should support the diagnoses; describe pathology observed in detail. For your and the surgical assistants benefit, describe the need for any surgical assistance. Include type of metal or ceramic surface of prostheses, orthopedic devices, use of cement and rationale for biological products. Include every item used in this description. Describe any complications and how handled intraoperatively.

40
RECOMMEND dictating within 24 hours of discharge for optimal coding. This intended to be more than a recap of the surgery performed. If complication occurs, THEN DOCUMENT IT IN THE D/C OP patients discharged the day of surgery also must have pertinent information filled in the form. If referred for Extended Recovery or Observation, a Discharge Note should be written on a Progress Note form with the correct DATE and TIME to document the proper flow of assessment and care provided during this period.

41
AAOS is working actively with CMS nationally and the Regional MACs to Clarify & modify the documentations requirements To try and delay the enforcement process until our members and our hospitals are better educated on the process and expectations Assisted in the development of a MLN Matters with CMS that was sent to all Medicare providers in Sept Supply YOU the membership with an informational piece and documentation form to utilize Help to develop a draft LCD for Regional MACs to utilize

43
MR should contain enough information to support the determination that the total joint procedure was reasonable and necessary =presence of advanced DJD Currently, audits show medical records commonly lack documentation that justifies the need for payment. Not Fraud and Abuse but lack of Documentation!!

44
Set up templates to ask the questions that you need to include and allow for comment sections so that you can explain yourself Describe the treatment plan with as many dates Add X-ray detail check-offs Instruct your office personnel on the importance

47
Show Me The Money! Thank You

Similar presentations



















>")




>")

