Download presentation
Presentation is loading. Please wait.

1
The Confused Elderly Patient Dr C Kotzé Dept of Psychiatry 2012

2
Acute –Delirium –Disturbance of brain physiology –Short term (weeks) –Secondary cause –“Acute brain failure” Chronic –Dementia –Disturbance of brain anatomy –Long term (years) –Primary or secondary cause Types of confusion
 –Secondary cause – Acute brain failure Chronic –Dementia –Disturbance of brain anatomy –Long term (years) –Primary or secondary cause Types of confusion")
3
Delirium

4
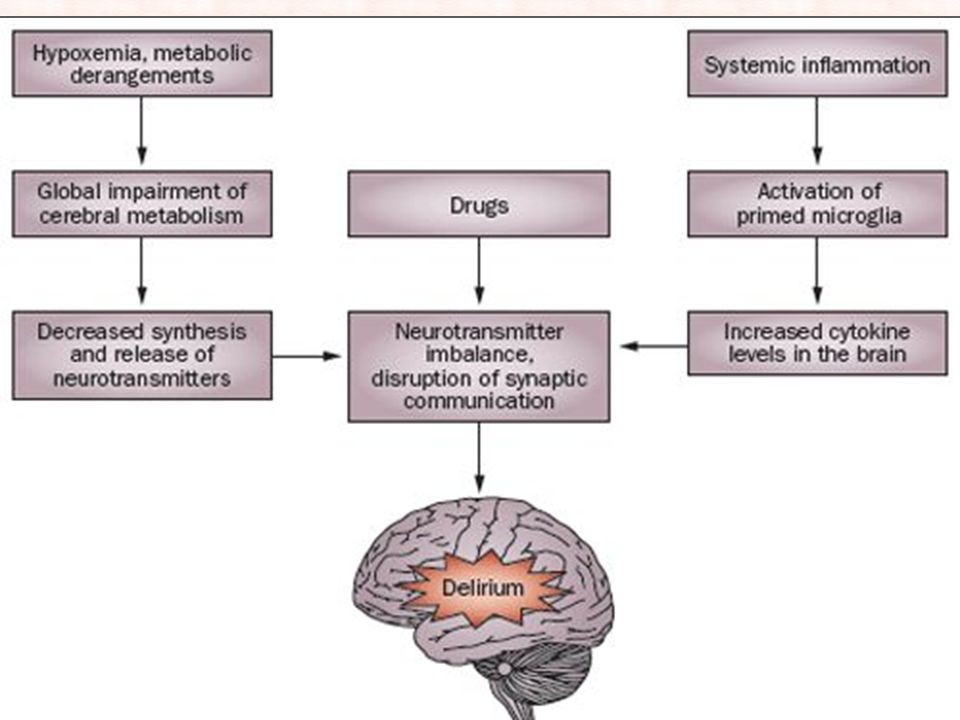
Delirium is a medical emergency Threatens the lives of older people if not recognized and treated It is a sudden change in mental state Fluctuates over 24 hours Alters consciousness Disturbs thinking and attention Results in changed behavior Delirium

5
Acute onset of clouding of consciousness Attention deficit & forgetful Disorientation Perceptual disturbances Hypersensitive to light / sounds Sleep-rhythm disturbance Incoherent speech Changing psychomotor activity Fluctuation of picture Characteristics

6
Infection (chest &UTI) Heart failure Metabolic disturbance Cerebro-vascular disease Drug administration Drug withdrawal (alcohol, BZ Hypothermia Any severe illness Causes
 Heart failure Metabolic disturbance Cerebro-vascular disease Drug administration Drug withdrawal (alcohol, BZ Hypothermia Any severe illness Causes")
8
Medical emergency Make an accurate diagnosis Treat any underlying condition Stop offending drugs Avoid sedation unless absolutely required Familiar medical personnel should deal with the patient Management

9
Aid orientation: get patient up spectacles & hearing aids provide clues to environment (signs etc) Prohibit the use of cot sides Nurse the person low to floor Use a soft night-light Management
 Prohibit the use of cot sides Nurse the person low to floor Use a soft night-light Management")
10
Haloperidol 0,5mg bd If severe restlessness: Lorazepam 2-4mg IMI q6h In substance withdrawal delirium: Withdrawal regime of long acting BZ Pharmacological

11
Dementia

12
Onset

13
Abrupt onset Acute, rarely >1 month Usually reversible Disorientation early Fluctuates hourly Altered & changing level of consciousness Short attention span Variation in sleep cycle Marked psychomotor changes Gradual onset Progress over years Generally irreversible Disorientation later More stable day to day Consciousness not clouded until terminal Normal attention Day-night reversal Psychomotor changes late Delirium vs Dementia

14
Age of onset

15
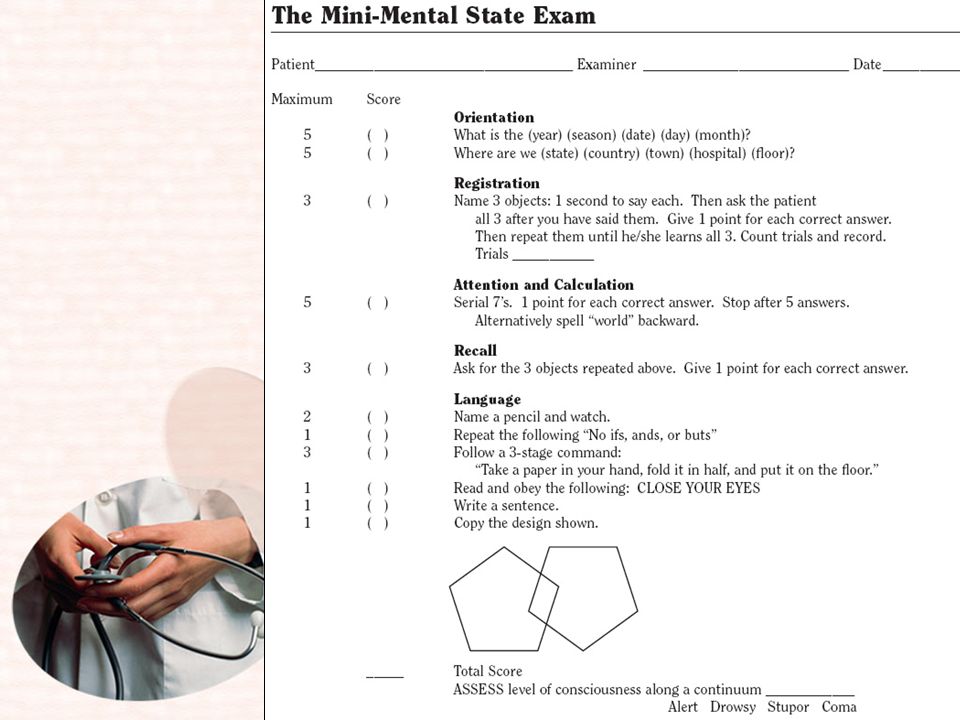
Characteristics Impaired executive function Memory impairment Disturbed judgment Other disturbances of higher cortical functions (aphasia, agnosia, apraxia) Personality change Delirium must be excluded
 Personality change Delirium must be excluded")
16
BPSD

17
Parenchymal disease of CNS AD, PD, Pick’s, Huntington’s, MS Systemic disease Thyroid disease, Hypoglycemia, Hypoxia, Encephalopathy, Multi-infarct dementia Nutritional deficiencies Drugs and toxins Intracranial pathology Infectious Creutzfeld-Jacob, Cryptococ, TB, HIV, Neurosyphilis Causes

19
THINK! From top to bottom Head: CAT/MRI for tumours, infarct, NPH etc Chest: ECG, X-Ray for heart & lungs Abdomen: bloods for liver, kidney, pancreas General: FBC etc for infections, anaemia, deficiency states LP only with high suspicion index Diagnosis

20
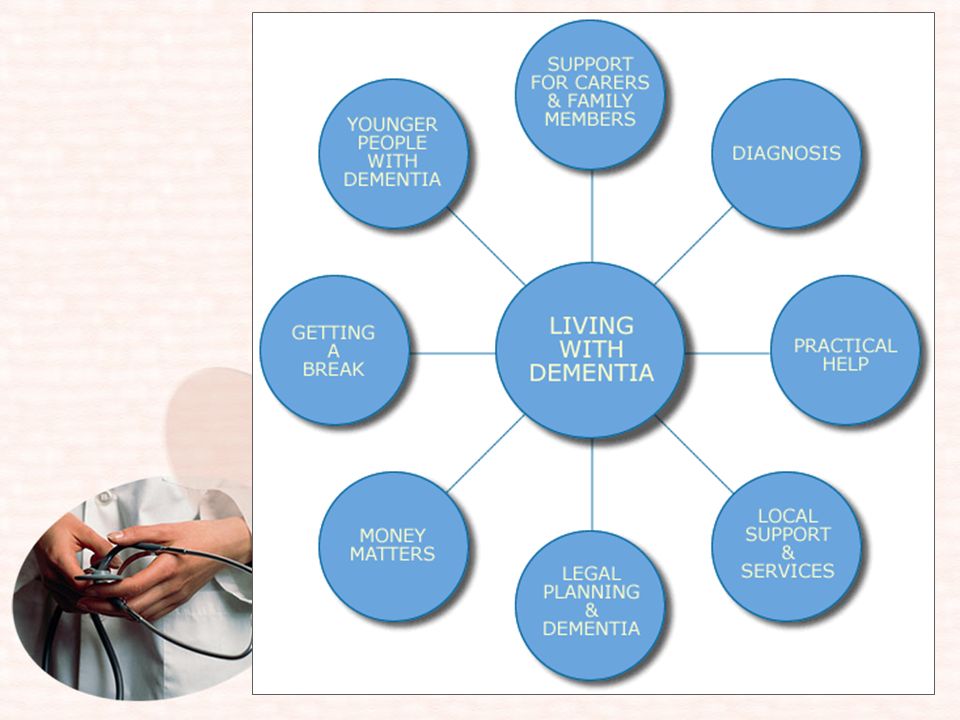
Make an etiological diagnosis Disease specific management Management of behavioral problems Prevent of complications Support of the family Include: Social worker Occupational therapist Physiotherapist Lawyer Nursing personnel Management

22
Non-pharmacological: Mild to moderate dementia: cognitive stimulation Pharmacological: Acetylcholinesterase inhibitors donepesil, galantamine, rivistigmine Memantine (NMDA antagonist) Management: Cognition
 Management: Cognition")
23
Non-pharmacological: Less expensive, no side-effects Identify behavioral problem and what precipitates it Nursing plan to curb the behavior Cognitive & behavioral therapy Interpersonal therapy Reality orientation Exercise and activities Management: BPSD

24
Consider a cholinesterase inhibitor Avoid anticholinergics Antipsychotics for psychosis, aggression, agitation, restlessness Haloperidol( Serenace) 0,5 – 2mg Risperidone(Risperdal) 0,25 –2mg Antidepressants for depression, anxiety, sleep disturbances Anticonvulsants for agitation, aggression, irritability Management: BPSD
 0,5 – 2mg Risperidone(Risperdal) 0,25 –2mg Antidepressants for depression, anxiety, sleep disturbances Anticonvulsants for agitation, aggression, irritability Management: BPSD")
25
Elderly persons often present with confusion, either primarily or when being treated for illness and post operatively NB is to distinguish between: Delirium: medical/neurological emergency: find cause and treat Dementia: must exclude treatable causes early: refer for specialist management initially Context in block SA8

Similar presentations






disorders ► Functional.>")












