Download presentation
Presentation is loading. Please wait.

1
ERT 420 BIOPHARMACEUTICAL ENGINEERING ERT 420 BIOPHARMACEUTICAL ENGINEERING Semester 1 Academic Session 2012/2013 HUZAIRY HASSAN School Of Bioprocess Engineering Universiti Malaysia Perlis

2
DRUG BIOAVAILABILTY & BIOEQUIVALENCE

3
Drug Absorption & Bioavailability Absorption is the rate and extent at which drugs reach the systemic circulation from the site of administration. Distribution of drugs includes all the processes involved from the time when the drugs reaches the circulation to the time when it (or drug metabolite) leaves the body. Metabolism involves all biochemical processes resulted in a chemical change to the drug compound including both the metabolism in the gut wall, the liver, and blood circulation. Excretion is the process in which the drug is eliminated from the systemic circulation into bile, urine, feces, sweat, and air.
 leaves the body. Metabolism involves all biochemical processes resulted in a chemical change to the drug compound including both the metabolism in the gut wall, the liver, and blood circulation. Excretion is the process in which the drug is eliminated from the systemic circulation into bile, urine, feces, sweat, and air..")
4
Bioavailability (BA): rate and extent to which API or active moiety is absorbed from a drug product and becomes available at the site of action. Bioavailablity, F ; F = F a x F g x F h * Fraction of drug absorbed Fraction that escapes metabolism in GI tract Fraction that escapes first pass hepatic metabolism

5
Oral drug absorption process occurs mainly in small intestinal regions, including passive transcellular diffusion, carrier-mediated transport processes, paracellular transport, and endocytosis. In general, Lipophilic compounds- absorbed by passive diffusion Hydrophilic compounds- absorbed through carrier- mediated process Some small hydrophilic compounds – may be transported through paracellular junction

6
Types of Intestinal Membrane Transport IMT includes paracellular and transcellular transports. Passage of solute without passage through the epithelium cells Can be divided into passive diffusion, endocytosis, and carrier-mediated transport.

8
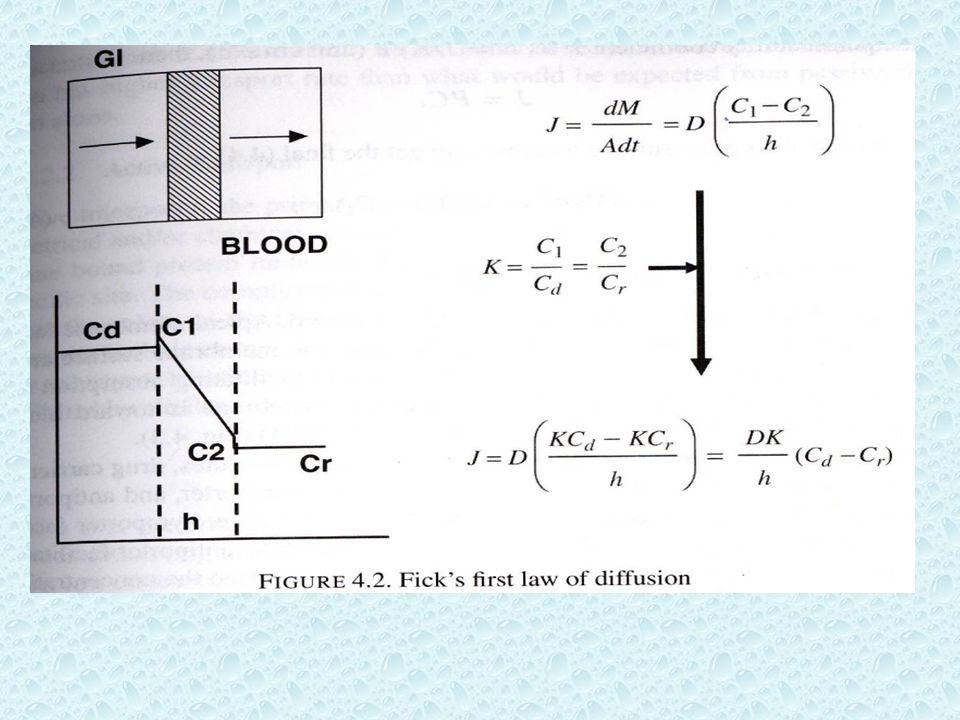
Transcellular Transport 1)Passive Diffusion - hydrophobic molecules can pass through the lipid bilayers by random molecular motions. - mass transfer of molecules depends on the concentration gradient on the 2 sides of membrane. - governed by Fick’s first law of diffusion.

9
J= flux (amount of material flowing through a unit cross section) M = drug mass (g, mol) A = surface area (cm 2 ) t = time (s) D = diffusion coefficient (diffusivity, cm 2 s -1 ) C 1 = drug concentration at membrane wall in intestinal lumen (mol L -1 ) C 2 = drug concentration at membrane wall in blood side (mol L -1 ) h = membrane thickness (cm)
 M = drug mass (g, mol) A = surface area (cm 2 ) t = time (s) D = diffusion coefficient (diffusivity, cm 2 s -1 ) C 1 = drug concentration at membrane wall in intestinal lumen (mol L -1 ) C 2 = drug concentration at membrane wall in blood side (mol L -1 ) h = membrane thickness (cm)")
11
Assumptions: -Steady state flux -The transfer of drugs reaches to steady state very fast -Steady state follows sink conditions: both side of membrane are well stirred and homogeneous. Define partition coefficient, K K = C 1 / C d = C 2 / C r C d : drug concentration in the GI lumen C r : drug concentration in the blood

13
2) Carrier-mediated Transport -Intestinal epithelial cell membranes are highly polarized. -Apical membrane faces the external lumen with many microvilli to increase membrane surface area. -Many membrane transporters are located in this side facilitating absorption for most nutrients and many drugs, while basolateral membrane is toward blood.

14
Carrier-mediated transport Facilitated Diffusion - Involve carrier protein - does not need energy - depends on solutes conc. gradient (similar to passive), but has higher transport rate Active transport - Transported against electrical / chemical conc. gradient. - Involves membrane bound protein molecule that binds reversibly to the solute at specific site - The complex changes in conformation that translocates the solute to the other side of membrane.
, but has higher transport rate Active transport - Transported against electrical / chemical conc. gradient. - Involves membrane bound protein molecule that binds reversibly to the solute at specific site - The complex changes in conformation that translocates the solute to the other side of membrane..")
15
3) Endocytosis -A process in which a substance or compound gain entry into a cell without passing through the lipid cell membrane. -3 types: Pinocytosis, Phagocytosis, and receptor- mediated. -In each types, endocytosis results in formation of intracellular vesicle by which the drug molecules are transported into the cells.

16
Paracellular Transport -Refers to transport solutes in between cells, without passage through the epithelial cells themselves. -Knowing that intercellular junctions between epithelial cells of capillaries are “leaky”, allowing paracellular transport of small molecules. -is passive transport, follows drug concentration gradient, does not require energy.

18
Factors Influence Drug Absorption Drug solubility GI Membrane permeability Dissolution of Solid Dosage Forms **Case Study**

19
1)Membrane permeability -Passive permeability (P) of molecules across a membrane: K: Partition coefficient (measure of substance solubility in lipid) D: Diffusion coefficient (depends on M W or size of molecule) h: thickness of cell membrane Therefore, P is related to membrane and drug properties. For specific drug, the passive membrane permeability should be a constant P m and independent to drug concentration.

20
-Active Permeability for absorption: J max : Maximum drug flux K m : Drug affinity to carrier Active permeability is dependent to drug concentration. Therefore, Total Effective Permeability:

22
2) Solubility - The drug molecules have to be dissolved in the solution for the absorption to occur in intestinal tract. -Low oil/water partition coefficient, K indicates high solubility in water and high K indicates high solubility in lipid. -But, drug with high lipid solubility possesses high membrane permeability. -Ionization: * For weak basic drugs, more unionized form would be predominant in intestine at high pH (5-8) favors absorption. * For weak acid drugs, more ionized form in intestine. * Ionized form is more water soluble than unionized. * Unionized form is easier for absorption by passive diffusion.
 favors absorption. * For weak acid drugs, more ionized form in intestine. * Ionized form is more water soluble than unionized. * Unionized form is easier for absorption by passive diffusion..")
23
3) Dissolution of solid dosage forms -For the drugs in solid dosage form, they must be dissolved in GI tract before absorption can take place. -For drugs with low solubility and high dose, the dissolution will be slow, and the dissolution rate will be rate-limiting step for absorption. -Factors that affect dissolution will control the whole absorption process.

24
BIOEQUIVALENCE Federal regulations (21 CFR, 2006) define Bioequivalence as: The absence of a significant difference in the rate and extent to which the active ingredient or active moiety in pharmaceutical equivalents or pharmaceutical alternatives becomes available at the site of drug action when administered at the same molar dose under similar conditions in an appropriately designed study.
 define Bioequivalence as: The absence of a significant difference in the rate and extent to which the active ingredient or active moiety in pharmaceutical equivalents or pharmaceutical alternatives becomes available at the site of drug action when administered at the same molar dose under similar conditions in an appropriately designed study.")
25
Equivalence: Relationship in terms of bioavailability, therapeutic response, or a set of established standards of one drug product to another. Bioequivalent drug products: describes pharmaceutical equivalent or pharmaceutical alternatives products that display comparable bioavailability when studied under similar experimental conditions. - For systemically absorbed drugs, the test and reference listed drug, RLD (brand-name) shall be considered bioequivalent if: a) the rate & extent of absorption of the test drug do not show significant difference from the rate & extent of absorption of the reference drug when administered at the same molar dose under similar experimental conditions in either single or multiple doses;
 shall be considered bioequivalent if: a) the rate & extent of absorption of the test drug do not show significant difference from the rate & extent of absorption of the reference drug when administered at the same molar dose under similar experimental conditions in either single or multiple doses;.")
26
b) the difference from the reference drug in the rate of drug absorption is intentional, is reflected in its proposed labeling, is not essential to the attainment of effective body drug concentrations on chronic use. Bioequivalent drug products may contain different inactive ingredients, provided the manufacturer identifies the differences and provides information that the differences do not affect the safety or efficacy of the product.

27
Pharmaceutical Alternatives (PA): -Drug products that contain the same therapeutic moiety but as different salts, esters, or complexes. -Ex: tetracycline phosphate or tetracycline hydrochloride equivalent to 250 mg tetracycline base. -Different dosage forms and strength within a product line by a single manufacturer (ex: extended-release dosage form and a standard immediate-release dosage form of the same active ingredient). -* FDA considers a tablet and capsule containing the same active ingredient in the same dosage strength as PA.
. -* FDA considers a tablet and capsule containing the same active ingredient in the same dosage strength as PA..")
28
Pharmaceutical Equivalents (PE): -Drug products in identical dosage forms that contain the same active ingredient (s), i.e., the same salt or ester, same dosage form, use the same route of administration, are identical strength or concentration (ex: chlordiazepoxide hydrochloride, 5-mg capsules), but, may differ in characteristics such as shape, scoring configuration, release mechanism, packaging, excipients ( including color, flavors, preservatives), expiration time, and within certain limit, labeling. When applicable, PE must meet the same content uniformity, disintegration time, and/or dissolution rates.

29
Biopharmaceutical Classification System According to BCS, drug substances are classified as : Class I : High Solubility – High Permeability Class II : Low Solubility – High Permeability Class III: High Solubility – Low Permeability Class IV: Low Solubility – Low Permeability

30
Info

31
THANK YOU

Similar presentations





 drugs to polar metabolites easily excreted in urine. The liver.>")

















