Download presentation
Presentation is loading. Please wait.

1
Avenida Hotel Maputo, Mozambique August 10-12, 2010 The 8th Annual Track 1.0 ART Program Meeting

2
The Latest Treatment Numbers and Transition Highlights Tedd V. Ellerbrock, MD, FACOG Co-Chair, Adult Treatment Technical Workgroup Team Leader, HIV Care and Treatment Global AIDS Program, NCHHSTP U.S. Centers for Disease Control and Prevention

3
Track 1.0 ART Program The Track 1.0 ART Program is funded & administered by the Division of Global HIV/AIDS at CDC and Global AIDS Program at Health Resources and Services Administration (HRSA) Four partners received Track 1.0 ART awards AIDSRelief (Catholic Relief Services Consortium) Elizabeth Glaser Pediatric AIDS Foundation (EGPAF) Harvard School of Public Health (Harvard) Mailman School of Public Health of Columbia University (Columbia) The program was funded in February 2004
 Four partners received Track 1.0 ART awards AIDSRelief (Catholic Relief Services Consortium) Elizabeth Glaser Pediatric AIDS Foundation (EGPAF) Harvard School of Public Health (Harvard) Mailman School of Public Health of Columbia University (Columbia) The program was funded in February 2004")
4
Program Year Annual Funding (millions) No. of Countries No. of Partner Programs No. of Treatment Facilities 1 (2004-05)$921121119 2 (2005-06)$1721324279 3 (2006-07)$2061324478 4 (2007-08)$3201325652 5 (2008-09) $44313251,030 6 (2009-10) $41313251,235 7 (2010-11) $3721325 Track 1.0 ART Program Funding, Countries, Partner Programs, and Facilities, by Program Year Total Funding since February 2004 = US $2 billion
$ ( )$ ( )$ ( )$ ( ) $ ,030 6 ( ) $ ,235 7 ( ) $ Track 1.0 ART Program Funding, Countries, Partner Programs, and Facilities, by Program Year Total Funding since February 2004 = US $2 billion.")
5
Track 1.0 ART Program The Emergency Plan for AIDS Relief Program Totals

6
Countries where Partners have Implemented Track 1.0 ART Programs, as of March 31, 2010 Country by PartnerAIDSRELIEFEGPAFHARVARDCOLUMBIATOTAL Botswana X 1 Cote d’Ivoire X X2 EthiopiaX X2 GuyanaX 1 HaitiX 1 KenyaX X2 MozambiqueX X2 NigeriaX XX3 RwandaX X2 South Africa Program Transitioned X X2 TanzaniaXXXX4 UgandaX 1 ZambiaXX2 TOTAL953 825

7
Number of Track 1.0 Treatment Sites by Country and Partner, as of March 31, 2010 Country by PartnerAIDSRELIEFEGPAFHARVARDCOLUMBIATOTAL Botswana1*1 Cote d’Ivoire12958187 Ethiopia15152 Guyana33 Haiti88 Kenya315182 Mozambique425799 Nigeria34253291 Rwanda164763 South Africa4965114 Tanzania9816542127432 Uganda19 Zambia196584 TOTAL229450684881,235 *Indirect Support

8
Number of Persons Currently on ART by Country and Partner, as of March 31, 2010 Country by PartnerAIDSRELIEFEGPAFHARVARDCOLUMBIATOTAL Botswana 8,498*8,498 Cote d’Ivoire 37,0112,95439,965 Ethiopia 60531,56732,172 Guyana855 Haiti3,140 Kenya39,75713,33553,092 Mozambique 20,15958,35378,512 Nigeria35,41843,65132,884111,953 Rwanda4,09219,40623,498 South Africa97,76355,325153,088 Tanzania31,91033,90333,95018,927118,690 Uganda26,176 Zambia33,00988,480121,489 TOTAL174,962277,31686,099232,751771,128 *Indirect Support

9
Number of Children (<15 years) Currently on ART by Country and Partner, as of March 31, 2010 Country by PartnerAIDSRELIEFEGPAFHARVARDCOLUMBIATOTAL Botswana n/a*0 Cote d’Ivoire 1,6991501,849 Ethiopia1072,7172,824 Guyana60 Haiti217 Kenya4,9751,7526,727 Mozambique 1,6575,4497,106 Nigeria1,9141,9972,0555,966 Rwanda5992,1562,755 South Africa11,3705,23116,601 Tanzania2,4463,0923,1011,51710,156 Uganda2,327 Zambia2,2925,6627,954 TOTAL14,93723,4805,09821,02764,542 *Indirect Support
 Currently on ART by Country and Partner, as of March 31, 2010 Country by PartnerAIDSRELIEFEGPAFHARVARDCOLUMBIATOTAL Botswana n/a*0 Cote d’Ivoire 1, ,849 Ethiopia1072,7172,824 Guyana60 Haiti217 Kenya4,9751,7526,727 Mozambique 1,6575,4497,106 Nigeria1,9141,9972,0555,966 Rwanda5992,1562,755 South Africa11,3705,23116,601 Tanzania2,4463,0923,1011,51710,156 Uganda2,327 Zambia2,2925,6627,954 TOTAL14,93723,4805,09821,02764,542 *Indirect Support")
10
Track 1.0 ART Program As of March 31, 2010: 2,116,203 ever enrolled in palliative care 1,129,590 (53%) currently in palliative care 1,133,027 ever started on ART 771,128 (68%) currently on ART Of those on ART, 64,542 (8%) were children Of adults on ART, 66% were females Of children on ART, 50% were females
 currently in palliative care 1,133,027 ever started on ART 771,128 (68%) currently on ART Of those on ART, 64,542 (8%) were children Of adults on ART, 66% were females Of children on ART, 50% were females")
11
Track 1.0 ART Program As of March 31, 2010: 2,116,203 ever enrolled in palliative care 1,129,590 (53%) currently in palliative care 1,133,027 ever started on ART 771,128 (68%) currently on ART Of those on ART, 64,542 (8%) were children Of adults on ART, 66% were females Of children on ART, 50% were females
 currently in palliative care 1,133,027 ever started on ART 771,128 (68%) currently on ART Of those on ART, 64,542 (8%) were children Of adults on ART, 66% were females Of children on ART, 50% were females")
12
Track 1.0 ART Program As of March 31, 2010: 2,116,203 ever enrolled in palliative care 1,129,590 (53%) currently in palliative care 1,133,027 ever started on ART 771,128 (68%) currently on ART Of those on ART, 64,542 (8%) were children Of adults on ART, 66% were females Of children on ART, 50% were females
 currently in palliative care 1,133,027 ever started on ART 771,128 (68%) currently on ART Of those on ART, 64,542 (8%) were children Of adults on ART, 66% were females Of children on ART, 50% were females")
13
Track 1.0 ART Program As of March 31, 2010: 2,116,203 ever enrolled in palliative care 1,129,590 (53%) currently in palliative care 1,133,027 ever started on ART 771,128 (68%) currently on ART Of those on ART, 64,542 (8%) were children Of adults on ART, 66% were females Of children on ART, 50% were females
 currently in palliative care 1,133,027 ever started on ART 771,128 (68%) currently on ART Of those on ART, 64,542 (8%) were children Of adults on ART, 66% were females Of children on ART, 50% were females")
14
Track 1.0 ART Program As of March 31, 2010: 2,116,203 ever enrolled in palliative care 1,129,590 (53%) currently in palliative care 1,133,027 ever started on ART 771,128 (68%) currently on ART Of those on ART, 64,542 (8%) were children Of adults on ART, 66% were females Of children on ART, 50% were females
 currently in palliative care 1,133,027 ever started on ART 771,128 (68%) currently on ART Of those on ART, 64,542 (8%) were children Of adults on ART, 66% were females Of children on ART, 50% were females")
15
Track 1.0 ART Program As of March 31, 2010: 2,116,203 ever enrolled in palliative care 1,129,590 (53%) currently in palliative care 1,133,027 ever started on ART 771,128 (68%) currently on ART Of those on ART, 64,542 (8%) were children Of adults on ART, 66% were females Of children on ART, 50% were females
 currently in palliative care 1,133,027 ever started on ART 771,128 (68%) currently on ART Of those on ART, 64,542 (8%) were children Of adults on ART, 66% were females Of children on ART, 50% were females")
16
Track 1.0 ART Program As of March 31, 2010: 2,116,203 ever enrolled in palliative care 1,129,590 (53%) currently in palliative care 1,133,027 ever started on ART 771,128 (68%) currently on ART Of those on ART, 64,542 (8%) were children Of adults on ART, 66% were females Of children on ART, 50% were females
 currently in palliative care 1,133,027 ever started on ART 771,128 (68%) currently on ART Of those on ART, 64,542 (8%) were children Of adults on ART, 66% were females Of children on ART, 50% were females")
17
Track 1.0 ART Program As of March 31, 2010: 2,116,203 ever enrolled in palliative care 1,129,590 (53%) currently in palliative care 1,133,027 ever started on ART 771,128 (68%) currently on ART Of those on ART, 64,542 (8%) were children Of adults on ART, 66% were females Of children on ART, 50% were females
 currently in palliative care 1,133,027 ever started on ART 771,128 (68%) currently on ART Of those on ART, 64,542 (8%) were children Of adults on ART, 66% were females Of children on ART, 50% were females")
18
Track 1.0 ART Program The Emergency Plan for AIDS Relief Number of Persons on ART by Partner and Quarter

19
Number of Persons on ART by Partner and Quarter, as of March 31, 2010 AIDSRelief 246,378 Ever Started On ART 71% on ART 10,712 patients/quarter

20
Number of Persons on ART by Partner and Quarter, as of March 31, 2010 EGPAF 18,321 patients/quarter 421,389 Ever Started On ART 66% on ART

21
Number of Persons on ART by Partner and Quarter, as of March 31, 2010 Harvard 66% on ART 5,700 patients/quarter 131,103 Ever Started On ART

22
Number of Persons on ART by Partner and Quarter, as of March 31, 2010 Columbia 70% on ART 14,528 patients/quarter 334,157 Ever Started On ART

23
Number of Persons on ART by Partner and Quarter, as of March 31, 2010 Program Totals 68% on ART 49,262 patients/quarter 1,133,027 Ever Started On ART

24
Track 1.0 ART Program The Emergency Plan for AIDS Relief CDC Transition Approach

25
Our Vision of Track 1.0 ART Program Transition Focus on strengthening the Ministry of Health (MOH), especially Regional and District health systems, to support HIV care and treatment services Build the capacity of local partners and civil society i nstitutions (NGOs and FBOs) to support the MOH in response to HIV/AIDS Strengthen ability of MOH and partners to compete for and manage direct USG and other international funding Gradually transition administrative and clinical responsibilities to the MOH and local partners, while continuing to provide quality care and treatment
, especially Regional and District health systems, to support HIV care and treatment services Build the capacity of local partners and civil society i nstitutions (NGOs and FBOs) to support the MOH in response to HIV/AIDS Strengthen ability of MOH and partners to compete for and manage direct USG and other international funding Gradually transition administrative and clinical responsibilities to the MOH and local partners, while continuing to provide quality care and treatment")
26
Essential Elements of Track 1.0 ART Program Transition Shared vision of what we plan to achieve Leadership of participating parties at all levels Commitment of time and effort, despite competing priorities Collaboration to develop a local strategy and processes that will work Willingness to transcend ownership issues Flexibility to encourage and support in-country perspectives, solutions, and thus ownership

27
How We Need to Work Together to Achieve Transition Track 1.0 ART Program Transition to MOH & Local Partners CDC Head- quarters CDC Country Office Track 1.0 Partner Head- quarters Track 1.0 Country Program Ministry of Health Local Partners ART Treatment Sites

28
Aligning Track 1.0 Transition Plans with In-Country Strategies Harmonize transition plans with Partnership Framework strategies Provide a role for MOH in transition decision-making Integrate transition activities into the processes of in-country CDC and national MOH systems Communicate the vision of the Track 1.0 transition to all levels of the MOH and other local partners Because transition plans were not initially fully aligned with in-country strategies, we found a need to help:

29
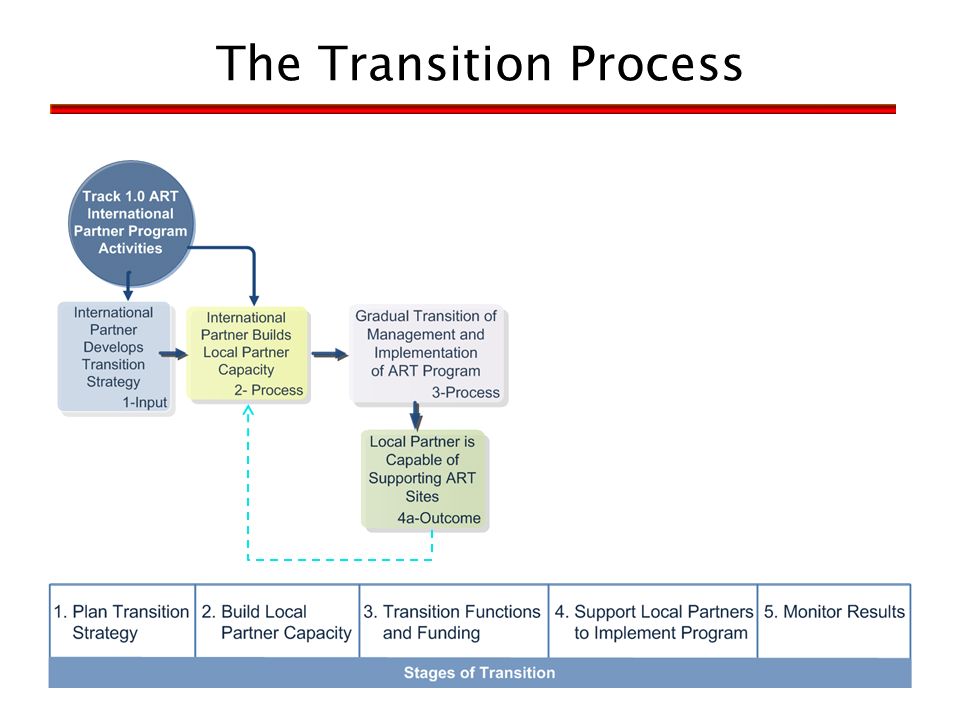
The Transition Process

34
Stages of Track 1.0 ART Program Transition Benchmarks 1Plan Transition Strategy 1.1 International partner (IP) has organizational strategy for transitioning significant portion of Track 1.0 HIV program functions to sustainable local capacity. 1.2 Local partners that can meet OGAC criteria are identified to take over specific program functions. 1.3 MOH and/or potential local partners participate in transition planning decision-making. 1.4 IP submits written transition plan strategy that includes detailed 3-year work plan and measurable benchmarks. 1.5 CDC country team and CDC or HRSA HQ team approves the transition plan and updates. 2Build Local Partner Capacity 2.1 IP has operational plan/approach to develop local partner capacity to provide and manage HIV specific program services. 2.2 IP conducts baseline assessment of local partners’ technical and organizational capacity that includes core competency areas 2.3 Local partner engages with IP in capacity-building work plan that includes human resources and organizational systems development. 2.4 IP validates and documents local partner capacity to begin to manage technical and administrative requirements of specific program areas. 3Supportive Transition of Functions and Funding to Local Partners 3.1 IP begins transition of key program functions and resources to local partner management responsibility through sub-grants and/or transfers to existing local partner USG awards. 3.2 IP transitions increasing amounts of resources and functional responsibilities to local partner through sub-grants or transfers to local partner USG awards during transition period. 3.3 IP continues to provide quality assurance support to local partner programmatic and financial management and implementation during transition period. 3.4 Local partners successfully apply for a USG funding opportunity announcement (FOA) in-country for local partners. 4Implementation by Local Partners 4.1 Local partners successfully manage key program functions as transferred by IP through sub-grants and/or transitions to existing local partner prime awards. 4.2 Local partner maintains and improves organizational capacity in core competency areas. 4.3 Local partner provides effective program service support to ART treatment sites in specific functional area. 4.4 Local partners successfully manage USG funding awards to support care and treatment sites and programs as a USG prime partner. 5Monitor Results 5.1 Program functions and associated funding of Track 1.0 ART program has transitioned to direct implementation and management by local partners as prime USG grantee. 5.2 All ART treatment sites in Track 1.0 program as continue to provide ART treatment services. 5.3 Uninterrupted supply of ARV medicines at site level is assured (in absence of national stock-outs). 5.4 Quality of service core indicators for ART treatment services are monitored through site assessments and supportive supervision on a scheduled basis. 5.5 Treatment sites implement a quality management system to sustain and improve quality of care, 5.6 Key program performance indicators remain level or improve for sites in Track 1.0 program during and after transition to local partners.
 in-country for local partners. 4Implementation by Local Partners 4.1 Local partners successfully manage key program functions as transferred by IP through sub-grants and/or transitions to existing local partner prime awards. 4.2 Local partner maintains and improves organizational capacity in core competency areas. 4.3 Local partner provides effective program service support to ART treatment sites in specific functional area. 4.4 Local partners successfully manage USG funding awards to support care and treatment sites and programs as a USG prime partner. 5Monitor Results 5.1 Program functions and associated funding of Track 1.0 ART program has transitioned to direct implementation and management by local partners as prime USG grantee. 5.2 All ART treatment sites in Track 1.0 program as continue to provide ART treatment services. 5.3 Uninterrupted supply of ARV medicines at site level is assured (in absence of national stock-outs). 5.4 Quality of service core indicators for ART treatment services are monitored through site assessments and supportive supervision on a scheduled basis. 5.5 Treatment sites implement a quality management system to sustain and improve quality of care, 5.6 Key program performance indicators remain level or improve for sites in Track 1.0 program during and after transition to local partners..")
35
Stages of Track 1.0 ART Program Transition Benchmarks 1Plan Transition Strategy 1.1 International partner (IP) has organizational strategy for transitioning significant portion of Track 1.0 HIV program functions to sustainable local capacity. 1.2 Local partners that can meet OGAC criteria are identified to take over specific program functions. 1.3 MOH and/or potential local partners participate in transition planning decision-making. 1.4 IP submits written transition plan strategy that includes detailed 3-year work plan and measurable benchmarks. 1.5 CDC country team and CDC or HRSA HQ team approves the transition plan and updates. 2Build Local Partner Capacity 2.1 IP has operational plan/approach to develop local partner capacity to provide and manage HIV specific program services. 2.2 IP conducts baseline assessment of local partners’ technical and organizational capacity that includes core competency areas 2.3 Local partner engages with IP in capacity-building work plan that includes human resources and organizational systems development. 2.4 IP validates and documents local partner capacity to begin to manage technical and administrative requirements of specific program areas. 3Supportive Transition of Functions and Funding to Local Partners 3.1 IP begins transition of key program functions and resources to local partner management responsibility through sub-grants and/or transfers to existing local partner USG awards. 3.2 IP transitions increasing amounts of resources and functional responsibilities to local partner through sub-grants or transfers to local partner USG awards during transition period. 3.3 IP continues to provide quality assurance support to local partner programmatic and financial management and implementation during transition period. 3.4 Local partners successfully apply for a USG funding opportunity announcement (FOA) in-country for local partners. 4Implementation by Local Partners 4.1 Local partners successfully manage key program functions as transferred by IP through sub-grants and/or transitions to existing local partner prime awards. 4.2 Local partner maintains and improves organizational capacity in core competency areas. 4.3 Local partner provides effective program service support to ART treatment sites in specific functional area. 4.4 Local partners successfully manage USG funding awards to support care and treatment sites and programs as a USG prime partner. 5Monitor Results 5.1 Program functions and associated funding of Track 1.0 ART program has transitioned to direct implementation and management by local partners as prime USG grantee. 5.2 All ART treatment sites in Track 1.0 program as continue to provide ART treatment services. 5.3 Uninterrupted supply of ARV medicines at site level is assured (in absence of national stock-outs). 5.4 Quality of service core indicators for ART treatment services are monitored through site assessments and supportive supervision on a scheduled basis. 5.5 Treatment sites implement a quality management system to sustain and improve quality of care, 5.6 Key program performance indicators remain level or improve for sites in Track 1.0 program during and after transition to local partners.
 in-country for local partners. 4Implementation by Local Partners 4.1 Local partners successfully manage key program functions as transferred by IP through sub-grants and/or transitions to existing local partner prime awards. 4.2 Local partner maintains and improves organizational capacity in core competency areas. 4.3 Local partner provides effective program service support to ART treatment sites in specific functional area. 4.4 Local partners successfully manage USG funding awards to support care and treatment sites and programs as a USG prime partner. 5Monitor Results 5.1 Program functions and associated funding of Track 1.0 ART program has transitioned to direct implementation and management by local partners as prime USG grantee. 5.2 All ART treatment sites in Track 1.0 program as continue to provide ART treatment services. 5.3 Uninterrupted supply of ARV medicines at site level is assured (in absence of national stock-outs). 5.4 Quality of service core indicators for ART treatment services are monitored through site assessments and supportive supervision on a scheduled basis. 5.5 Treatment sites implement a quality management system to sustain and improve quality of care, 5.6 Key program performance indicators remain level or improve for sites in Track 1.0 program during and after transition to local partners..")
36
Organizational domains (All domains apply for potential MOH and local partners that may become USG prime partners.) Technical program domains (Specific domains to be selected/defined according to program area(s) the local partner will implement.) Governance/Leadership Strategic planning & execution Human resource management Performance measurement, analysis and improvement systems/CQI External relationships, networks, and partnerships Financial management Ability to apply for and manage USG grants Strategic resource mobilization (other than USG) Clinical HIV service delivery Routine supervision of HIV services Training (clinical and other in-service) for HIV program/service delivery Clinical mentoring Laboratory services Infrastructure rehabilitation Supply chain support/management Community and patient services Monitoring and evaluation Technical assistance to MOH Core Capacity Domains
 Technical program domains (Specific domains to be selected/defined according to program area(s) the local partner will implement.) Governance/Leadership Strategic planning & execution Human resource management Performance measurement, analysis and improvement systems/CQI External relationships, networks, and partnerships Financial management Ability to apply for and manage USG grants Strategic resource mobilization (other than USG) Clinical HIV service delivery Routine supervision of HIV services Training (clinical and other in-service) for HIV program/service delivery Clinical mentoring Laboratory services Infrastructure rehabilitation Supply chain support/management Community and patient services Monitoring and evaluation Technical assistance to MOH Core Capacity Domains")
37
Strategic Guidance for a Standards-based Approach to National ART Program Supervision to Assure Quality Care and Sustainability of U.S. Government Support to National ART Program This system would implement and/or maintain the following standards: There is a regular schedule of joint (USG-MOH) supportive supervisory site visits There is a reliable results monitoring system for oversight of partners and programs All ART sites have a functional and sustainable patient monitoring system There is a regular schedule and reporting of ART data quality assessment activities All ART sites have QM/PI processes in place
 supportive supervisory site visits There is a reliable results monitoring system for oversight of partners and programs All ART sites have a functional and sustainable patient monitoring system There is a regular schedule and reporting of ART data quality assessment activities All ART sites have QM/PI processes in place.")
38
Track 1.0 ART Program The Emergency Plan for AIDS Relief The Way Forward

39
Early Lessons Learned Transition of program responsibilities to MOH and local partners must be accompanied by new program approaches designed to progressively increase leadership and decision-making roles of MOH and local partners during the transition period Engaging MOH leaders at sub-national levels (e.g., at Regions, Provinces, and Districts) to provide transition leadership and support is essential
 to provide transition leadership and support is essential")
40
Early Lessons Learned We need increased emphasis on measurable benchmarks for USG partners to support increasing health system capacity at district and provincial levels to sustain integrated HIV services Transition can gain momentum by focusing on early wins, transitioning functions that can be readily absorbed by existing systems in the country, if adequate external funding and assistance is provided (e.g., human resources)
")
41
Early Lessons Learned Learning-by-doing is an effective method for strengthening MOH and local partners’ capacity to manage increasing fiscal responsibilities through direct funding of activities The rate of transition to the Ministry of Health and other local partners in resource-limited settings depends upon the capacity of the local entities to absorb the administrative, fiscal, and clinical responsibilities of the programs (i.e., the rate of transition is determined by the local absorptive capacity)
")
42
Early Lessons Learned Learning-by-doing is an effective method for strengthening MOH and local partners’ capacity to manage increasing fiscal responsibilities through direct funding of activities The rate of transition to the Ministry of Health and other local partners in resource-limited settings depends upon the capacity of the local entities to absorb the administrative, fiscal, and clinical responsibilities of the programs (i.e., the rate of transition is determined by the local absorptive capacity)
")
43
What Is Needed to Support Track 1.0 Transition Reasonable timeline to ensure MOH or local partner has capacity to assume transition responsibilities Flexibility to re-program Track 1.0 funds into new awards to be fully operational post-February 2012 Recognition that international partners will be needed for selected activities beyond 2012 in some countries Flexibility to define success as what is reasonable to achieve in a country, given existing limitations Ability to monitor transition of leadership, program functions, responsibilities, performance, and results

44
The Track 1.0 cooperative agreement for the 4 grantees that supports 26 programs in 13 countries will end on February 28, 2012 New funding opportunities will be announced to support continuous HIV care and treatment programs by CDC country teams, and will be in place, prior to February 2012 New funding opportunities will emphasize goals for continuing the transition to sustainability in PEPFAR II, including increased support for Ministries of Health and local partners Track 1.0 Close-Out: February 2012

Similar presentations











 Tool and other Mechanisms to Monitor Transition Status Track 1 Implementers.>")

 Pre-Review Conference Call Competitive Funding Opportunity Announcement: HRSA-15-021 March 25,>")




 Dr. Shirley Lecher, CDC Director Caribbean Regional Office On Behalf of the.>")




 Madhu Deshmukh Director, HIV/AIDS.>")