Download presentation
Presentation is loading. Please wait.

1
Project First Step: Approaches to Co-occurrence of Child Maltreatment & Substance Abuse in New Hampshire 2007 CAPTA State Liaison Meeting Bernie Bluhm, NH DCYF bbluhm@dhhs.state.nh.us

2
Vision Statement We envision a state in which every child lives in a nurturing family and plays and goes to school in communities that are safe and cherish children. Mission Statement We are dedicated to assisting families in the protection, development, permanency, and well-being of their children and the communities in which they live. DCYF Comprehensive Child & Family Services Plan, 2004-2009 NH DHHS, Children, Youth, & Families

3
Key Project Aims Identify & Address Parental Substance Abuse Problems co-occurring with suspected child abuse or neglect. Better Decision-Making about Safety Reduce Substance Abuse Risk Behaviors of Parents Fewer Subsequent Founded Referrals Prevent or Shorten Placement of Children in Foster Care Improve Stability and Adjustment of Children Cost Neutrality/Savings of Project

4
Demonstration Project Design Abuse/Neglect reports to the most populous Co in NH (2 Offices). Substance Abuse IDd as Current Risk Factor LADC services initiated up front close to first face:face CPS contact. Random selection: Control/Exp groups maintained for five yrs.

5
LADC/Counselor Role Engage Client at Time of Assessment of Allegation Immediate Screening & Assessment by LADC Immediate individual treatment for AODA, presenting MH conditions – Joins with domestic violence specialist Immediate and ongoing consultation for CPSW

6
For Families Receiving Services Consultant participates in case planning Keep focus on parent issues Include parenting in treatment goals Aftercare with focus on parenting Support to relative caregivers

7
For people awaiting treatment Individual counseling On-going contact with counselor – Treatment window extended 60 days from CPS assessment or case closure – Treatment provider connections

8
Evaluation Design Experimental Model with True Randomized Design to Standard/Enhanced Services at 2 District Offices Enhanced Group: LADC + CPS Standard Group: Received the usual services provided by NH DCYF UNH-FRL Eval. Team – Conducted confidential interviews with parents in both groups. – Analyzed case records, SACWIS data, LADC records. – Process & Outcomes data Cost Benefit (In terms of IV-E Dollars)
.")
9
Final Evaluation Status Conducted 11/15/99 through 10/15/04 – 437 families were involved in the demonstration 212 baseline interviews (49%) 156 follow-up interviews (74%)
 156 follow-up interviews (74%)")
10
Study Sample Demographics: Primary Caregiver Enhanced Group (n=222): Mean Age: 33 Years % White: 92% Any Employment: 59% Relationship of Alleged Perp. to Child Bio. Mother 69% Mean Family Size Total Adults: 1.83 Total Children: 2.80 Standard Group (n=215): Mean Age: 33 Years % White: 90% Any Employment: 63% Relationship of Alleged Perp. to Child Bio. Mother: 72% Mean Family Size Total Adults: 1.85 Total Children: 2.84
: Mean Age: 33 Years % White: 90% Any Employment: 63% Relationship of Alleged Perp. to Child Bio. Mother: 72% Mean Family Size Total Adults: 1.85 Total Children:")
11
Maltreatment & CPS Factors Enhanced Group (n=222) CPS Factors Prior Referrals * 44% High Risk at Entry 11% Type of Maltreatment Physical Abuse 25% Phys. Abuse & Negl. 13% Neglect: 52% Sexual Abuse: 3% Psychological Abuse: 1% Standard Group (n=215) CPS Factors Prior Referrals 51% High Risk at Entry 14% Type of Maltreatment Physical Abuse: 21% Phys. Abuse & Negl: 9% Neglect: 56% Sexual Abuse: 5% Psychological Abuse: 2%
 CPS Factors Prior Referrals 51% High Risk at Entry 14% Type of Maltreatment Physical Abuse: 21% Phys. Abuse & Negl: 9% Neglect: 56% Sexual Abuse: 5% Psychological Abuse: 2%.")
12
Family Risk Factors Enhanced (n=222) Domestic Violence: 33% Adult Mental Illness: 14% Adult Phys. Disability: 4% Homeless: 17% Incarceration (Case Level): 32% Standard (n=215) Domestic Violence: 33% Adult Mental Illness: 16% Adult Phys. Disability: 7% Homeless: 14% Incarceration (Case Level): 28%
: 32% Standard (n=215) Domestic Violence: 33% Adult Mental Illness: 16% Adult Phys. Disability: 7% Homeless: 14% Incarceration (Case Level): 28%.")
13
Child Risk Factors Enhanced Group (n=222) Mental Illness: 6% Phys. Disability: 3% Learning Disabled 11% Neonatal Addiction: 2% Severe Behavior Prob. 5% JPPO* Involvement at Case Level 26% Standard Group (n=215) Mental Illness: 7% Phys. Disability: 5% Learning Disabled: 13% Neonatal Addiction: 1% Severe Behavior Prob. 9% JPPO* Involvement at Case Level 24% * DHHS Division for Juvenile Justice Services Juvenile Probation & Parole Officers, involved due to child status offenses or delinquency.
 Mental Illness: 7% Phys. Disability: 5% Learning Disabled: 13% Neonatal Addiction: 1% Severe Behavior Prob. 9% JPPO* Involvement at Case Level 24% * DHHS Division for Juvenile Justice Services Juvenile Probation & Parole Officers, involved due to child status offenses or delinquency..")
14
Co-Morbidity in Interview Sample

15
Substance Abuse Factors At initial assessment, 36% demonstrated a high probability of having a substance dependence disorder (via modified SASSI). Strong association with partners substance abuse. – 70% of women reporting heavy alcohol use, reported similar heavy use by partners (p<.01) – Intimate partners drug use is significantly correlated (p<.001) – Heavy drinking women are significantly more likely to have partners who use illicit drugs (p=.06)
 – Intimate partners drug use is significantly correlated (p<.001) – Heavy drinking women are significantly more likely to have partners who use illicit drugs (p=.06).")
16
Victimization & Trauma Hx. Of Adult

17
Domestic Violence identified in Initial CPS Study Referrals Over half (58%) had a prior Order of Protection at some time Over 1/3 report DV in current year 19% got a protective order on current partner in the past
 had a prior Order of Protection at some time Over 1/3 report DV in current year 19% got a protective order on current partner in the past")
18
Co-Morbidity 45% of high-probability have prior diagnosis of mental illness. 45% of high probability have clinical levels of depression 18% prior hx of mental illness documented in initial record data. 45% Clinically Depressed using CESD measure.

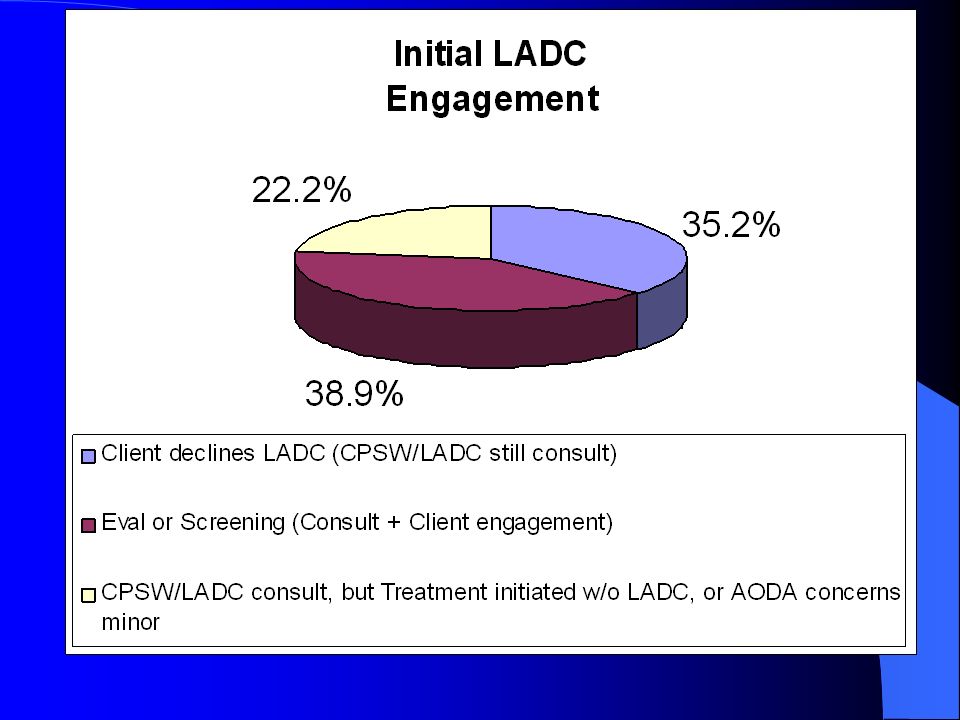
19
Outcomes: Substance Abuse & Assessment

21
Outcomes: Substance Abuse & Child Protection Identification of co-occurring substance abuse by CPS increased by 37% (29-66%). Decreased repeat substantiation (significant decrease in site A) Improved Permanency Outcomes: – Increased kinship care (22% vs 16%) – Decrease in placement changes (1.78 vs 2.72) – Increased reunification (44% vs 39%)* – Less time to TPR (22.7 vs 26.5 months) *Over 50% in site A
 Improved Permanency Outcomes: – Increased kinship care (22% vs 16%) – Decrease in placement changes (1.78 vs 2.72) – Increased reunification (44% vs 39%)* – Less time to TPR (22.7 vs 26.5 months) *Over 50% in site A.")
22
ADULT OUTCOMES

23
Treatment Utilization by Group

24
Womens Treatment Utilization by Groups (Interview Sample) EnhancedStandard % Attend AA T1 (ever) T2 (past yr.) 41% (40/97) 66% (19/29) 45% (39/87) 44% (10/23) % Help for drinking T1 (ever) T2 (past yr.) 24% (23/97) 48% (11/23) 32% (32/100) 43% (6/14) % Hospitalization for drinking T1 (ever) T2 (past yr.) 16% (15/97) 28% (4/14) 18% (18/100) 11% (1/9)
 EnhancedStandard % Attend AA T1 (ever) T2 (past yr.) 41% (40/97) 66% (19/29) 45% (39/87) 44% (10/23) % Help for drinking T1 (ever) T2 (past yr.) 24% (23/97) 48% (11/23) 32% (32/100) 43% (6/14) % Hospitalization for drinking T1 (ever) T2 (past yr.) 16% (15/97) 28% (4/14) 18% (18/100) 11% (1/9)")
25
Womens Education & Employment by Group ( Interview Sample, Self Reports ) EnhancedStandard % Employed FT T1 T2 30% 38% 28% 24%* %Enrolled Educ./Voc. Program T228%17%

26
Case (Child Safety) Outcomes
 Outcomes")
27
Child Outcomes

28
Child Outcomes for Index Children ages 4-17 Children in Enhanced Groups had greater declines key problem categories: –Anxiety & Depression –Withdrawn/Depressed –Somatic Problems –Attention Problems –Aggressive Behavior

29
Child School & Health Outcomes Enhanced Group – Repeated Grade* 10% – Academic/Other School Problems 39% – MD concerns re: health 11% Standard Group – Repeated Grade* 29% – Academic/Other School Problems 43% – MD concerns re: health 14%

30
Conclusions Key Outcomes – Improved documentation and response in assessments. – More Long-Term Substance Abuse Treatment of Adults – Child Safety Outcomes, including: fewer subsequent founded reports*, more stability, decrease in time to TPR – Improved Well Being for Adults & Children – Not cost neutral strictly in terms of IV-E funding

31
First Step Program: Post IV-E Waiver Demo March 2005 Two largest district offices (Manchester & Nashua) composing 25% of the statewide caseload of abuse/neglect assessments. Additional region (Central NH) to be added, increasing First Step to 33% of statewide caseload.
 to be added, increasing First Step to 33% of statewide caseload..")
32
First Step Program: Post IV-E Waiver Demo Local child protection supervisor links LADC and CPSW when: – Child Abuse/Neglect report approved for face:face assessment (Investigation) + – Parental substance abuse idd as a factor. LADC involved as: – CPSW consult, – AODA Assessment, Treatment, Case Management

33
Sustainable funding considerations: PSSF & CAPTA

35
Overview of Treatment Recommendations LADC provides direct treatment and case management: Goal is community based treatment

36
NH Dept. of Health & Human Services Children, Youth, & Families Thank You! University of New Hampshire Family Research Lab

Similar presentations















 Grants Chapter 6.>")



 House Human Services Committee August 8, 2006.>")
