Download presentation
Presentation is loading. Please wait.

1
If I had Chronic Kidney Disease: What would I want my Doctor to Know….. Liam Plant Department of Renal Medicine, Cork University Hospital Department of Medicine, University College Cork School of Medicine

2
Conceptual Framework Pathophysiological Processes Mechanisms Clinical Practice Strategies

3
What happens when kidneys fail? Conceptually best viewed as loss of nephrons Conceptually best viewed as not having any dysfunction of the myriad functions of the renal epithelial cells

4
Where?

5
(One of the) Central Mechanism(s) HypertensionProteinuria InflammationFibrosis Angiotensin II
 Central Mechanism(s) HypertensionProteinuria InflammationFibrosis Angiotensin II")
6
Prevalent ESKD patients (n) 3505 patients 42% HD 5%Home 53% TX 786 p.m.p.
 3505 patients 42% HD 5%Home 53% TX 786 p.m.p.")
7
6 Year Increase in Dialysis Prevalence 31/12/03 – 31/12/09 647 patients 64% All 78%HD 2%PD Mean (95%C.I.) 108 (65,151)All 107 (72,142)HD 1 (-17,19)PD
 108 (65,151)All 107 (72,142)HD 1 (-17,19)PD")
8
Identify the Gold Standard Sensible Default

9
Who gets CKD? Risk Groups 10% of adults (3-4% CKD 3+) 60% male Older adults Racial Groups Diabetes/Vascular Disease/Other How detected Screening – which groups Opportunistic Intercurrent Illness Primary presentation
 60% male Older adults Racial Groups Diabetes/Vascular Disease/Other How detected Screening – which groups Opportunistic Intercurrent Illness Primary presentation.")
10
NeoErica project: 112,215 patients (12 practices) [Creat] in last 10 years - 27.4% – 74% in last 2 years Proteinuria recorded in 9.1% 24.9% had eCrClr <60ml/min (C&G) At least 5.1% of UK population CKD 3-5 (NHANES-III 4.7% of US populationCKD 3-5) Any CKD in adults – up to 10%
![ NeoErica project: 112,215 patients (12 practices) [Creat] in last 10 years % – 74% in last 2 years Proteinuria recorded in 9.1% 24.9% had eCrClr <60ml/min (C&G) At least 5.1% of UK population CKD 3-5 (NHANES-III 4.7% of US populationCKD 3-5) Any CKD in adults – up to 10%](http://images.slideplayer.com/24/7020747/slides/slide_10.jpg " NeoErica project: 112,215 patients (12 practices) [Creat] in last 10 years % – 74% in last 2 years Proteinuria recorded in 9.1% 24.9% had eCrClr <60ml/min (C&G) At least 5.1% of UK population CKD 3-5 (NHANES-III 4.7% of US populationCKD 3-5) Any CKD in adults – up to 10%")
11
Issues What would I fear………………………………….. How would I be evaluated………………………… How would I alter my lifestyle…………………….. What treatments would I wish……………………… How would I wish to be monitored and by whom………

12
What would I fear………..? Premature death from non-renal complications Career, financial, family plans Badly organised care pathways Pain ‘Uraemia’ Renal Replacement Therapy

13
Theoretical Construct Complications DeathESKDGFRCKDRISKHI-RISK

14
How would I be evaluated..? Define presence of CKD Stratify stage of CKD; estimate rate of progression Identify underlying cause (specific measures) Target objectives
 Target objectives.")
15
Chronic Kidney Disease One or more of: Proteinuria Haematuria (not urological) Radiological abnormality Histological abnormality
 Radiological abnormality Histological abnormality")
16
5 Key data points 1.Stage of CKD GFR Hypertension Proteinuria 2.Complications 3.Rate of Progression 4.Comorbidities 5.Cause of CKD

17
K/DOQI Stratification StageGFR (ml/min/1.73m2) Comment 1*>90 Hypertension Structural problem 2*60-89 Hypertension Structural problem 330-59 Complications Progression/Referral 415-29 More Complications Referral/Preparation 50-14 RRT/Conservative
 Comment 1*>90 Hypertension Structural problem 2*60-89 Hypertension Structural problem Complications Progression/Referral More Complications Referral/Preparation RRT/Conservative")
18
Proteinuria Dipstick for Screening 24hr collection if nothing better (worse!) to do Protein/Creatinine or Albumin/Creatinine ratios Express as mg/mmol (x0.0088 for 24h) (divide by 100!) <3.0Normal 3.0 – 34.0Microalbuminuria >34.0Proteinuria
 to do Protein/Creatinine or Albumin/Creatinine ratios Express as mg/mmol (x for 24h) (divide by 100!) <3.0Normal 3.0 – 34.0Microalbuminuria >34.0Proteinuria")
19
How would I alter my lifestyle..? Stop smoking Continue drinking Sensible, healthy diet; passage to ‘elite’ diet only in special circumstances A BMI target to remember……………..

20
What treatments would I wish..? Conservative treatment Specific treatment Dialysis therapies Transplantation Palliative care

21
What treatment is appropriate for these patients? Review medications. Stop NSAID’s. Adjust other medications if needed because of level of CKD. · Treat BP to a target of <130/80. This may require multiple medications. ACEi/ARB are 1 st choice therapies. · If PCR >300mg/mmol – treat to target of <125/75. · If 10year CV risk estimate is >20% - consider anti-platelet agent/statin. · Encourage smoking cessation, exercise, weight loss. · Immunise against influenza and pneumococcus.

22
Stage 4-5 drugs Erythropoeisis-stimulating agents Drugs for secondary hyperparathyroidism Anti-rejection drugs

23
How monitored and by whom..? Conservative treatment Specific treatment Dialysis therapies Transplantation

24
April 2006Corrigan Club

25
‘New Good Practice’ Renal function expressed as eGFR 4-point MDRD Formula CKD classified as Stage 1-5 K/DOQI Classification Protein to Creatinine; Albumin to Creatinine ratio Detection, monitoring, referral criteria www.renal.org/CKDguide/ckd.html www.renal.org/CKDguide/ckd.html Non-visit-based Specialist advice service

26
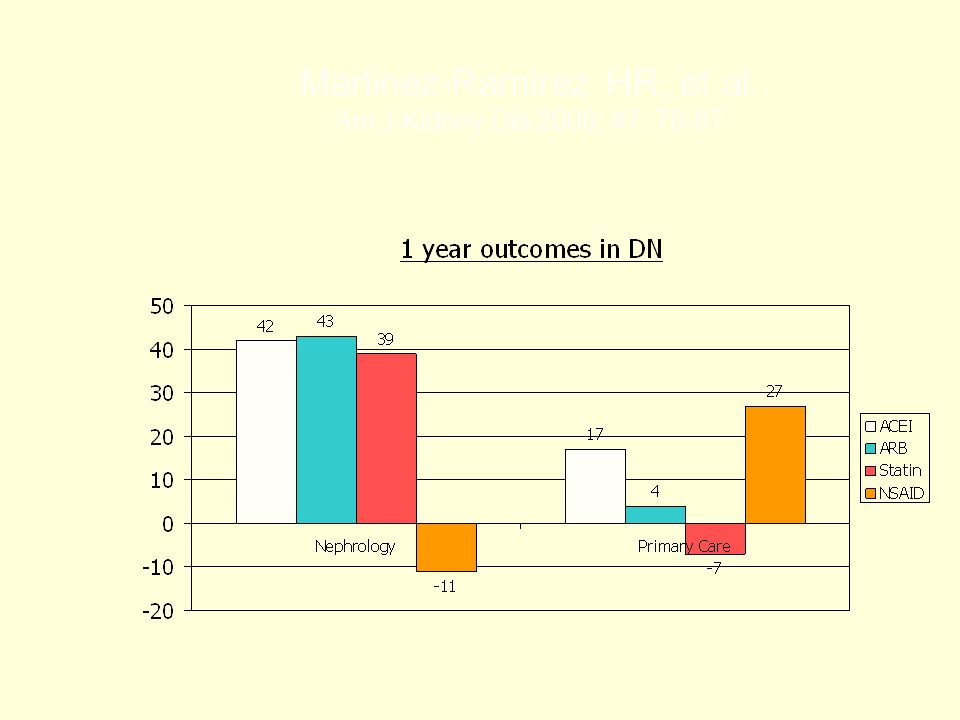
Martinez-Ramirez HR, et al. Am J Kidney Dis 2006; 47: 78-87

28
Conclusion Levey AS, et al. Chronic kidney disease as a global public health problem: Approaches and positions – a position statement from Kidney Diseases Improving Global Outcomes. Kidney Int 2007; 72: 247-59. Taal M, Tomson S. UK Renal Association Clinical Practice Guidelines, 4 th Edition 2007. www.renal.org/guidelines/module1.html Irish Nephrology Society. Irish CKD Guidelines. www.nephrology.ie

Similar presentations






![Chronic kidney disease: [insert title here] Insert name, title, date here Insert acknowledgements here.](/12/3497998/big_thumb.jpg "Chronic kidney disease: [insert title here] Insert name, title, date here Insert acknowledgements here.>")






>")





