Download presentation
Presentation is loading. Please wait.

1
Judith R. Peres, LCSW-C Long Term Care Discussion Group July 23, 2015

2
Dying in America IOM 2013 Committee on Approaching Death Recommendations Role of IOM – Public Policy Opportunities for Long-term Care Overview

3
Dying in the United States Today 2.5 million people die each year 83% are Medicare Beneficiaries Common ways of dying:

4
Dying will always be hard Two fundamental facts ensure that the transition to death will remain difficult: 1.Medicine's inability to predict the future. 2.A widespread and deeply held desire not to be dead.

5
But it doesn’t have to be this hard In the absence of conversations about prognosis, goals, and outcomes of treatment, patients do not have the opportunity to express their values and preferences. Leading clinicians to assume that patients want additional interventions, even late in the illness. JAMA Intern Med.2014;174(12)
.")
6
How Americans Wish to Die

7
“Approaching Death in America: Improving Care at the End of Life” IOM, 1997 Good Death – free from avoidable distress and suffering for patients, families and caregivers, in accord with patients’ and families wishes; and consistent with clinical, cultural & ethical standards Bad death – needless suffering, disregard for patient or family wishes or values and a sense among participants that norms of decency have been offended

8
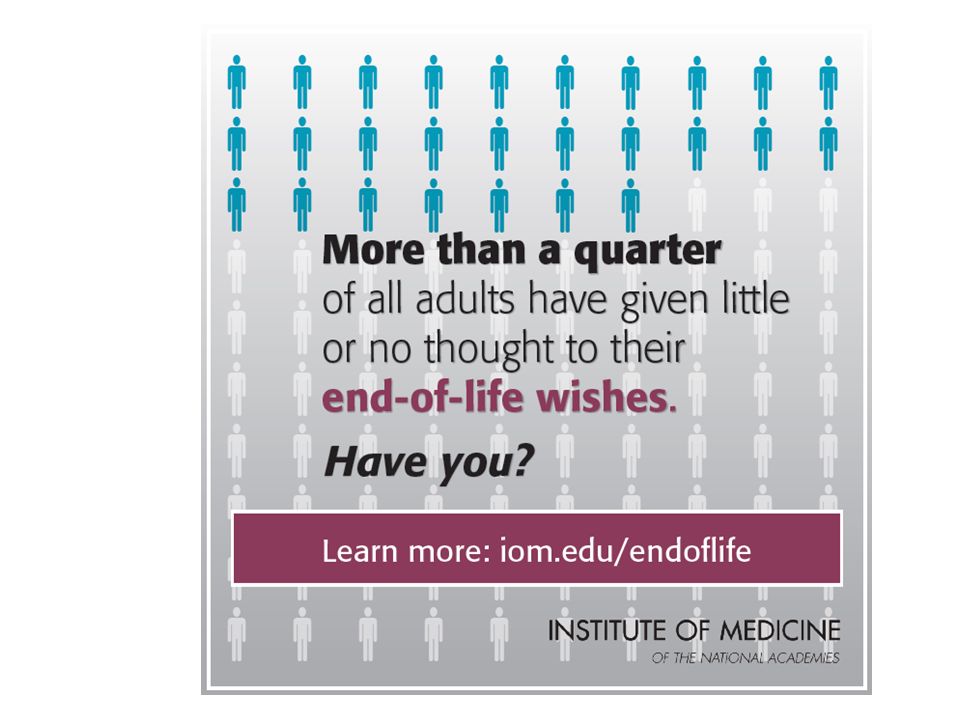
IOM 2013 Committee on Approaching Death: Addressing Key End of Life Issues Current state of end of life care with respect to: Delivery of medical care and social supports Patient-family-provider communication of values and preferences Advance care planning Health care costs, financing, and reimbursement Education of health professionals, patients and loved ones, and the public at large

9
Dying in America Key Conclusions Major gaps in care near end of life Urgent attention needed from numerous stakeholder groups Person-centered, family-oriented approach to care near the end of life should be a high national priority Compassionate, affordable, and effective care is an achievable goal Released September 17, 2014 Report available: www.nap.eduwww.nap.edu

10
Dying in America Five Recommendations 1) Person-centered, family-oriented (palliative) care 2) Clinician-patient communication and advance care planning 3) Professional education and development 4) Policies and payment systems 5) Public education and engagement
 Person-centered, family-oriented (palliative) care 2) Clinician-patient communication and advance care planning 3) Professional education and development 4) Policies and payment systems 5) Public education and engagement")
11
Key Recommendations 1. Person-centered, family-oriented (palliative) care All insurers should cover comprehensive care for individuals with advanced serious illness who are near the end of life. “Comprehensive Care” Seamless, high quality, consistently accessible around the clock; Consider evolving biopsychosocial/spiritual needs; Coordinated –across all sites of care; Consistent with person’s values goals and INFORMED preference.
 care All insurers should cover comprehensive care for individuals with advanced serious illness who are near the end of life. Comprehensive Care Seamless, high quality, consistently accessible around the clock; Consider evolving biopsychosocial/spiritual needs; Coordinated –across all sites of care; Consistent with person’s values goals and INFORMED preference..")
12
One Solution: Palliative Care

13
Key Recommendations 2. Clinician-patient communication and advance care planning Professional and quality organizations should develop standards for clinician-patient communication and advance care planning that are measurable, actionable, and evidence based. Adherence to these standards should be tied to credentialing, licensing, and reimbursement.

14
Welcome to Medicare – 2003 Affordable Care Act - 2010 Wellness Visit – 2011 CPT Editorial Panel -2016 ACP services Codes - 99497 & 99498 Comments Due 9/8/15! Public Policy Attempts to “have the conversation”

15
Workbooks, tools

16
3. Professional Education and Development Establish training, certification, and licensure requirements that strengthen the palliative care knowledge and skills of all clinicians who care for individuals with advanced serious illness… Key Recommendations

18
4. Policies and Payment Systems Federal, state, private insurance and health care delivery programs should integrate the financing and delivery of medical and social services; And require public reporting of quality and costs for care near the end of life. Key Recommendations

19
Policies and Payment Systems Require the use of interoperable electronic health records that incorporate advance care planning to improve communication of individuals’ wishes across time, settings, and providers. Encourage states to develop and implement a Physician Orders for Life-Sustaining Treatment (POLST) paradigm program in accordance with nationally standardized core requirements.
 paradigm program in accordance with nationally standardized core requirements..")
20
5. Public Education and Engagement Every element of society should engage their constituents and provide factual information about care of people with advanced serious illness to encourage advance care planning and informed choice based on the needs and values of individuals. Key Recommendations

22
IOM secures services of eminent professionals to examine policy matters pertaining to the health of the public. IOM under the National Academy of Sciences through its congressional charter as advisor to the federal government. “IOM” recommendations can have a lot of influence in health care policy decision-making. Why does the IOM matter?

23
IOM has now made clear (in 6 reports): Palliative care IS essential to quality Institute of Medicine Quality Cancer Care Report: Charting a New Course for a Health System in Crisis (2013) QOL care
: Palliative care IS essential to quality Institute of Medicine Quality Cancer Care Report: Charting a New Course for a Health System in Crisis (2013) QOL care")
24
Palliative Care and Value-Based, Accountable Care Models Palliative care aligns with new care and innovative payment models – Helps to reduce avoidable hospitalizations and ED use – Strengthens person-centeredness and consumer engagement and satisfaction – Improves coordination along the continuum – Avoids unnecessary and unwanted service utilization and expense

25
Opportunity for Long-term care Educate policy leaders on how to revise existing state and federal legislation encouraging the integration of medical and social service financing. Identify and share LTC quality measures related to palliative and end-of- life care. Support model quality improvement projects focused on the delivery of palliative care in all care settings including LTC. Demonstrate LTC ability to coordinate care across settings and providers, and improve shared decision making and advance care planning. Work toward LTC inclusion of electronic health records including incorporating advance care planning to improve communication of individuals’ wishes across time, settings, and providers.

27
27 Report and Dissemination Report available: http://www.iom.edu/Reports/2014/Dyin g-In-America-Improving-Quality-and- Honoring-Individual-Preferences-Near- the-End-of-Life.aspx Free slide deck for download IOM will engage in 12 month dissemination phase: o Developing materials o Engaging relevant stakeholders and key audiences o Evaluating tactics to inform future activities

28
Good Reads!

Similar presentations













 Presentation to HIT Steering Committee May 24, 2012.>")




>")

