Download presentation
Presentation is loading. Please wait.

1
Fluid management at the ER some practical tips

2
Objectives □ initial fluid management of some very challenging ER disorders (perioperative cases and severe malnutrition in shock) □ rationale
 □ rationale")
3
Hydration status. Normal clinical parameters. sensoriumAlert,awake,oriented Heart rateN for age Nature of pulsesFull crt< 2 sec temperatureNormothermic Skin colorPink. No mottling/pallor uo1 – 2 cc/k/hr or 500 – 600 ml/bsa/24 hrs BPN for age

4
examination3% - 5% Mild dhn 6% - 10% Moderate dhn 10% - 15% Severe dhn Skin turgornormaltentingTenting Skin by touchnormaldryClammy lipsmoistdryCracked eyesnormalDeep setSunken tearspresentreducedNone fontanelleflatsoftSunken sensoriumconsolableirritableObtunded Pulse rateNormal to incincreasedVery rapid Pulse qualitynomalWeakNon-palpable crtnomal2 – 3 sec> 3 sec uonormaldecreasedanuric Physiologic parameters of abnormal hydration status. Berman (2000) and Oski (1999).
 and Oski (1999)..")
5
Fluid and electrolyte management Maintenance fluids + measurable losses + non-measurable losses

6
APA CONSENSUS GUIDELINE ON PERIOPERATIVE FLUID MANAGEMENT IN CHILDREN v 1.1 September 2007

7
Maintenance fluids + measurable loss + non-measurable loss Holliday-Segar Method first 10 kg4 ml/k/hr 11 - 20 kg2 ml/k/hr >20 kg1 ml/k/hr

8
Maintenance fluids + measurable loss + non-measurable loss From tube drains (ogt, ctt, etc) + gastrostomy + urethral catheter + etc
 + gastrostomy + urethral catheter + etc")
9
APA CONSENSUS GUIDELINE ON PERIOPERATIVE FLUID MANAGEMENT IN CHILDREN v 1.1 September 2007

10
Maintenance fluids + measurable loss + non-measurable loss Clinical statemodifying factor fever0.13 per C >38 degrees Simple trauma0.20 Multiple trauma0.40 Burns0.5 – 1.0

11
electrolyte composition of body fluids fluidNa (meq/L)k (meq/L)cl (meq/L)protein gastric20 - 805 - 20100 - 150 pancreatic120 - 1405 - 1590 - 120 small bowel100 - 1405 - 1590 - 130 bile120 - 1405 - 1580 - 120 ileostomy45 - 1353 - 1520 - 115 diarrhea10 - 9010 - 8010 - 110 burn14051103 - 5 g/dL sweat10 - 303 - 1010 - 35
k (meq/L)cl (meq/L)protein gastric pancreatic small bowel bile ileostomy diarrhea burn g/dL sweat")
12
Some commonly used fluids solutionsNa (mEq/L)K (mEq/L) PLR/D5LR1304 PNSS154 D50.45NaCl77 D50.3NaCl51 D5IMB2520 D5NM4013 D5NR1405
K (mEq/L) PLR/D5LR1304 PNSS154 D50.45NaCl77 D50.3NaCl51 D5IMB2520 D5NM4013 D5NR1405")
13
13 Fluids plasma Na ( meq/L) 141 K4K4 Mg 2 Buffer bicarb Ph 7.4 Osm 289 0.9%Nacl1545.7308 LR1304lactate6.4273 Normosol-R / plasmalyte 14053Acetate & gluconate 7.4295
 141 K4K4 Mg 2 Buffer bicarb Ph 7.4 Osm %Nacl LR1304lactate Normosol-R / plasmalyte 14053Acetate & gluconate")
14
APA CONSENSUS GUIDELINE ON PERIOPERATIVE FLUID MANAGEMENT IN CHILDREN v 1.1 September 2007

15
APA CONSENSUS GUIDELINE ON PERIOPERATIVE FLUID MANAGEMENT IN CHILDREN v 1.1 September 2007

16
APA CONSENSUS GUIDELINE ON PERIOPERATIVE FLUID MANAGEMENT IN CHILDREN v 1.1 September 2007

17
APA CONSENSUS GUIDELINE ON PERIOPERATIVE FLUID MANAGEMENT IN CHILDREN v 1.1 September 2007

18
examination3% - 5% Mild dhn 6% - 10% Moderate dhn 10% - 15% Severe dhn Skin turgornormaltentingTenting Skin by touchnormaldryClammy lipsmoistdryCracked eyesnormalDeep setSunken tearspresentreducedNone fontanelleflatsoftSunken sensoriumconsolableirritableObtunded Pulse ratenormalincreasedVery rapid Pulse qualitynomalWeakNon-palpable crtnomal2 – 3 sec> 3 sec uonormaldecreasedanuric Physiologic parameters of abnormal hydration status. Berman (2000) and Oski (1999).
 and Oski (1999)..")
19
APA CONSENSUS GUIDELINE ON PERIOPERATIVE FLUID MANAGEMENT IN CHILDREN v 1.1 September 2007

20
APA CONSENSUS GUIDELINE ON PERIOPERATIVE FLUID MANAGEMENT IN CHILDREN v 1.1 September 2007

21
APA CONSENSUS GUIDELINE ON PERIOPERATIVE FLUID MANAGEMENT IN CHILDREN v 1.1 September 2007

22
APA CONSENSUS GUIDELINE ON PERIOPERATIVE FLUID MANAGEMENT IN CHILDREN v 1.1 September 2007

23
POST OPERATIVE FLUID MANAGEMENT i. Surgery, pain, nausea and vomiting are all potent causes of ADH release. A recent NPSA alert has recommended that hypotonic fluids should not be used for postoperative maintenance as this may cause hyponatraemia due to retention of free water released after metabolism of dextrose from the solution. APA CONSENSUS GUIDELINE ON PERIOPERATIVE FLUID MANAGEMENT IN CHILDREN v 1.1 September 2007

24
ii. Consensus was not agreed on the maintenance fluid rate in the postoperative period. Some would use the full rate as calculated using Holliday and Segar’s formula, while others would fluid restrict to 60-70% of full maintenance and additional boluses of isotonic fluid given as required. iii. In the postoperative period ongoing losses from drains or nasogastric tubes should be replaced with an isotonic fluid such as 0.9% sodium chloride with or without added KCl. iv. Losses should be measured hourly and replaced every 2 to 4 hours depending on the amount. APA CONSENSUS GUIDELINE ON PERIOPERATIVE FLUID MANAGEMENT IN CHILDREN v 1.1 September 2007

25
MONITORING OF FLUID THERAPY i. Serum electrolytes do not need to be measured pre-operatively in healthy children prior to elective surgery where IV fluids are to be given. ii. Serum electrolytes need to be measured pre-operatively in all children presenting for elective or emergency surgery who require IV fluid to be administered prior to surgery. iii. Children should be weighed prior to fluids being prescribed and given. iv. Serum electrolytes should be measured every 24 hours in all children on IV fluids or more frequently if abnormal. v. Although ideally children should be weighed daily while on IV fluids, practically this is difficult in older children, or those who have undergone major surgery. Use of a fluid input/output chart will help with fluid management. APA CONSENSUS GUIDELINE ON PERIOPERATIVE FLUID MANAGEMENT IN CHILDREN v 1.1 September 2007

29
fluid therapy DKA (University of Texas Southern Medical center) 1. correction of shock a. 0.9% NaCl, 10 - 20 cc/kg or b. colloid or 5% albumin, 10 -20 ml/kg 2. 0.9% NaCl, 10 ml/kg for next hour; calculate maintenance and replacement 3. 1.5 x normal maintenance + 1/2 of replacement in first 12 hours 4. 1.5 x normal maintenance + 1/2 of replacement in next 24 hours

30
TIMETHERAPYCOMMENTS 1st hr 10-20 mL/kg IV bolus 0.9% NaCl or LR Insulin drip at 0.05 to 0.10 ?/kg/hr Quick volume expansion; may be repeated. NPO. Monitor I/O, neurologic status. Use flow sheet. Have mannitol at bedside; 1g/kg IV push for cerebral edema. 2nd hr until DKA resolution 0.45% NaCl: plus continue insulin drip 20 mEq/L KPhos and 20 mEq/L KAc 5% glucose if blood sugar >250 mg/dL (14 mmol/L) Iv rate = 85ml/kg + maintenance – bolus 23 hr If K <3 mEq/L, give 0.5 to 1.0 mEq/kg as oral K solution OR increase IV K to 80 mEq/L VariableOral intake with subcutaneous insulin No emesis; CO 2 ≥16 mEq/L; normal electrolytes Note that the initial IV bolus is considered part of the total fluid allowed in the 1st 24 hr and is subtracted before calculating the IV rate. Maintenance (24 hr) = 100 mL/kg (for the 1st 10 kg) + 50 mL/kg (for the 2nd 10 kg) + 25 mL/kg (for all remaining kg) Table 583-4 -- DIABETIC KETOACIDOSIS (DKA) TREATMENT PROTOCOL Nelson’s Textbook of Pediatrics, 19 th ed., 2011
 Iv rate = 85ml/kg + maintenance – bolus 23 hr If K <3 mEq/L, give 0.5 to 1.0 mEq/kg as oral K solution OR increase IV K to 80 mEq/L VariableOral intake with subcutaneous insulin No emesis; CO 2 ≥16 mEq/L; normal electrolytes Note that the initial IV bolus is considered part of the total fluid allowed in the 1st 24 hr and is subtracted before calculating the IV rate. Maintenance (24 hr) = 100 mL/kg (for the 1st 10 kg) + 50 mL/kg (for the 2nd 10 kg) + 25 mL/kg (for all remaining kg) Table DIABETIC KETOACIDOSIS (DKA) TREATMENT PROTOCOL Nelson’s Textbook of Pediatrics, 19 th ed.,")
31
3. Fluids replacement For patients who are severely volume depleted but not in shock, volume expansion (resuscitation) should begin immediately with 0.9% saline to restore the peripheral circulation. The volume and rate of administration depends on circulatory status and, where it is clinically indicated, the volume administered typically is 10 ml/kg/h over 1-2 hours, and may be repeated if necessary, to assure a stable circulatory status. Global IDF/ISPAD Guideline for Diabetes in Childhood and Adolescence
 should begin immediately with 0.9% saline to restore the peripheral circulation. The volume and rate of administration depends on circulatory status and, where it is clinically indicated, the volume administered typically is 10 ml/kg/h over 1-2 hours, and may be repeated if necessary, to assure a stable circulatory status. Global IDF/ISPAD Guideline for Diabetes in Childhood and Adolescence.")
32
In the rare patient with DKA who presents in shock or severe circulatory collapse, rapidly restore circulatory volume with isotonic saline in 20 ml/kg bolus infused as quickly as possible through a large bore cannula. Repeat if necessary, with careful reassessment after each bolus. Global IDF/ISPAD Guideline for Diabetes in Childhood and Adolescence

33
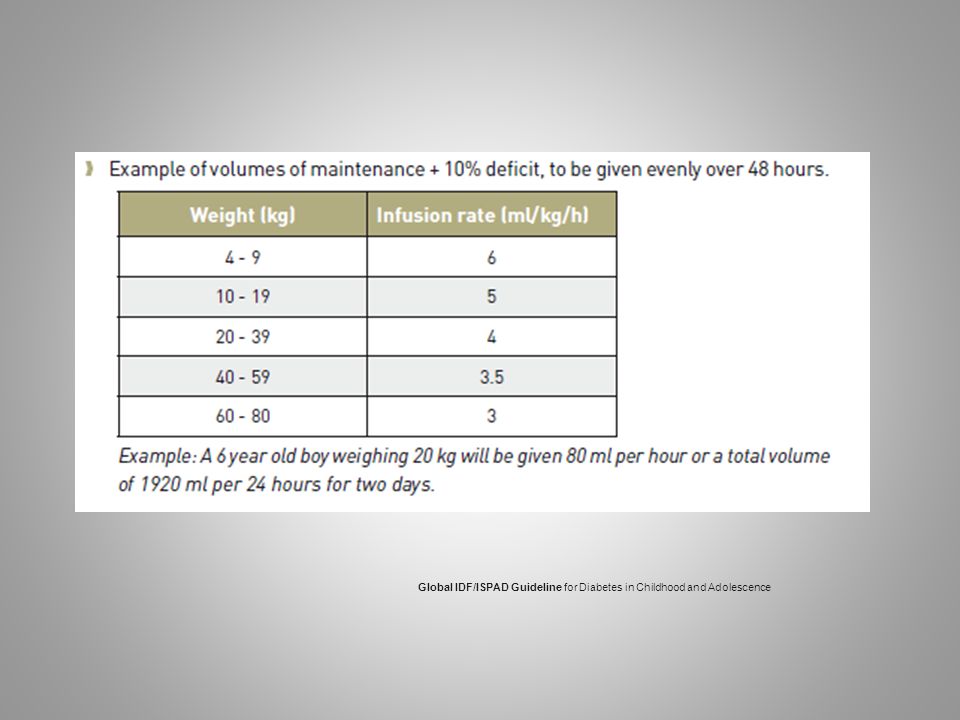
Fluid management (deficit replacement) should be with 0.9% saline for at least 4-6 hours. Thereafter, deficit replacement should be with a solution that has a tonicity equal to or greater than 0.45% saline with added potassium chloride, potassium phosphate or potassium acetate The rate of fluid (IV and oral) should be calculated to rehydrate evenly over 48 hours. Fluid management (deficit replacement) should be with 0.9% saline for at least 4-6 hours Thereafter, deficit replacement should be with a solution that has a tonicity equal to or greater than 0.45% saline with added potassium chloride, potassium phosphate or potassium acetate. The rate of fluid (IV and oral) should be calculated to rehydrate evenly over 48 hours. Global IDF/ISPAD Guideline for Diabetes in Childhood and Adolescence
 should be calculated to rehydrate evenly over 48 hours. Fluid management (deficit replacement) should be with 0.9% saline for at least 4-6 hours Thereafter, deficit replacement should be with a solution that has a tonicity equal to or greater than 0.45% saline with added potassium chloride, potassium phosphate or potassium acetate. The rate of fluid (IV and oral) should be calculated to rehydrate evenly over 48 hours. Global IDF/ISPAD Guideline for Diabetes in Childhood and Adolescence.")
35
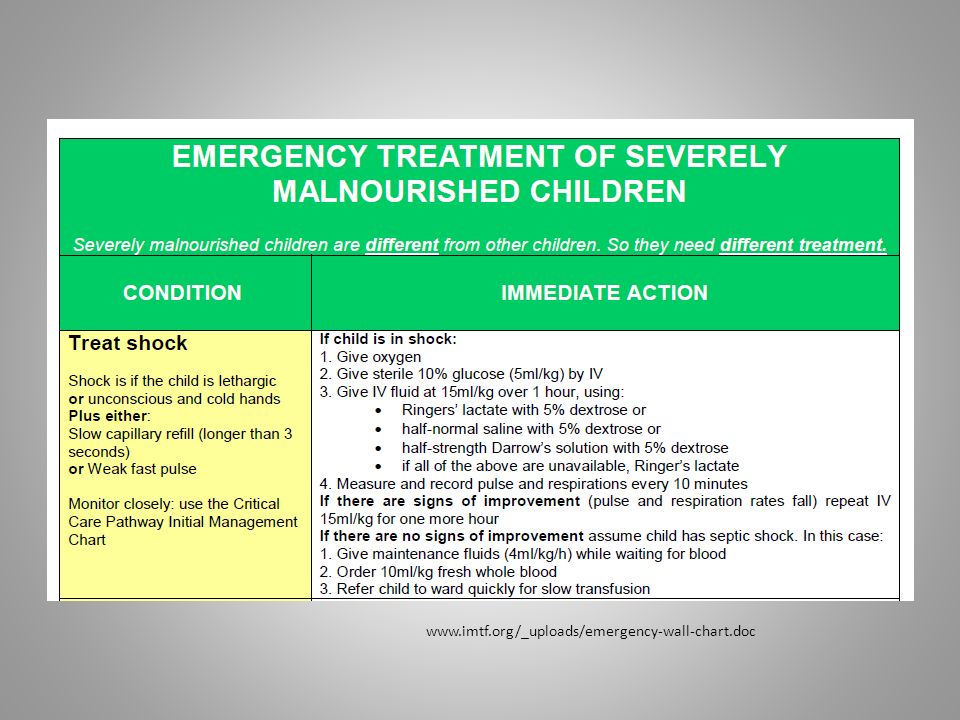
Shock in severely malnourished children Guidelines for the inpatient treatment of severely malnourished children WHO 2003

36
www.imtf.org/_uploads/emergency-wall-chart.doc
37
Severe Dehydration with Shock Dr. Shinjini Bhatnagar, Center for Diarrheal Disease and Nutrition Research

39
Dr. Shinjini Bhatnagar, Center for Diarrheal Disease and Nutrition Research

40
www.imtf.org/_uploads/emergency-wall-chart.doc
41
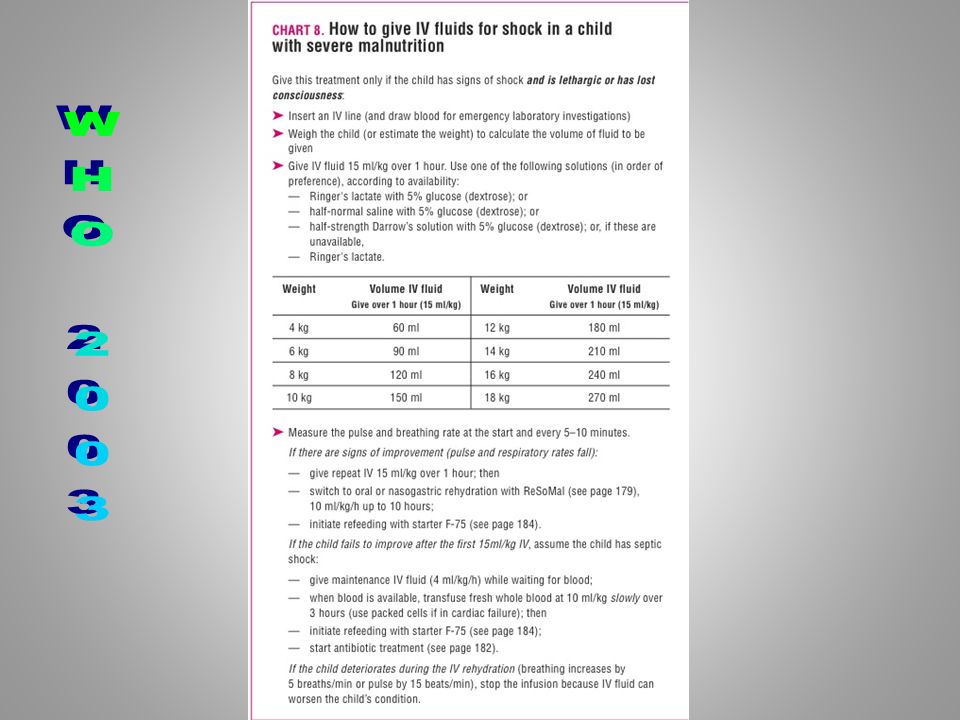
Treatment give oxygen give sterile 10% glucose (5 ml/kg) by IV give IV fluid at 15 ml/kg over 1 hour. Use Ringer’s lactate with 5% dextrose; or half-normal saline with 5% dextrose; or half-strength Darrow’s solution with 5% dextrose measure and record pulse and respiration rates every 10 minutes give antibiotics

42
Treatment If with signs of improvement: repeat IV 15 ml/kg over 1 hour; then switch to oral or nasogastric rehydration with ReSoMal, 10 ml/kg/h for up to 10 hours. (Leave IV in place in case required again); Give ReSoMal in alternate hours with starter F-75, then continue feeding with starter F-75
; Give ReSoMal in alternate hours with starter F-75, then continue feeding with starter F-75.")
43
Treatment If the child fails to improve after the first hour of treatment (15 ml/kg), assume that the child has septic shock. In this case: give maintenance IV fluids (4 ml/kg/h) while waiting for blood, when blood is available transfuse fresh whole blood at 10 ml/kg slowly over 3 hours; then begin feeding with starter F-75 (step 7)
 while waiting for blood, when blood is available transfuse fresh whole blood at 10 ml/kg slowly over 3 hours; then begin feeding with starter F-75 (step 7).")
44
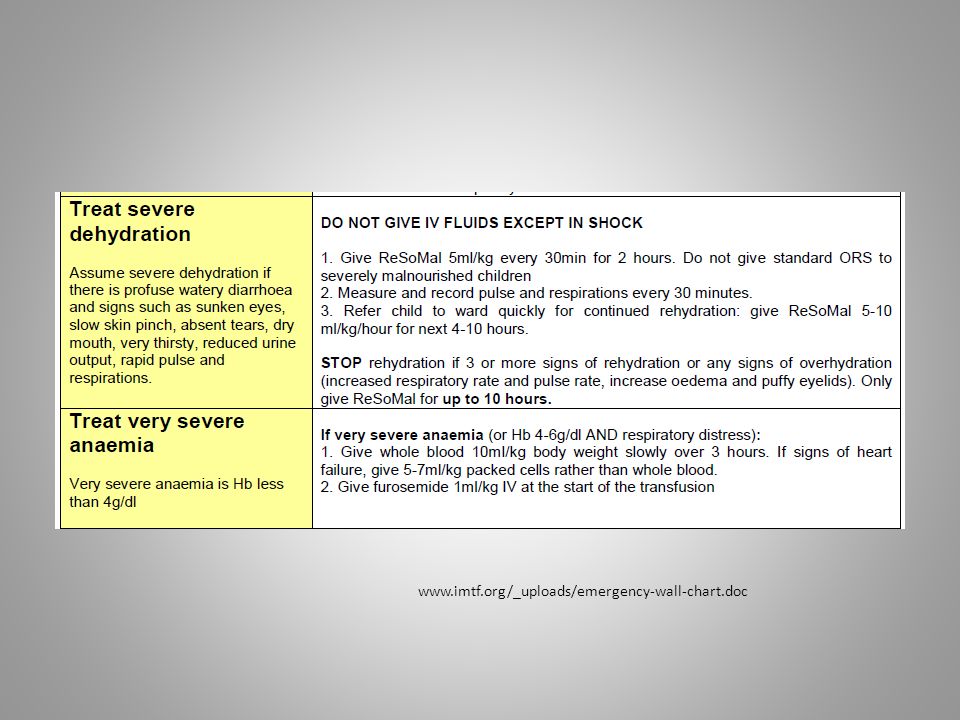
Treatment A blood transfusion is required if: Hb is less than 4 g/dl or if there is respiratory distress and Hb is between 4 and 6 g/dl whole blood 10 ml/kg body weight slowly over 3 hours child has signs of cardiac failure, transfuse packed cells (5-7 ml/kg) rather than whole blood.
 rather than whole blood.")
Similar presentations

>")

















