Download presentation
Presentation is loading. Please wait.

1
Glucose-6-phosphate Dehydration Deficiency Nada Mohamed Ahmed, MD, MT (ASCP)i
i")
2
Objectives Introduction Definition Factors cause G6PD deficiency Factors cause G6PD deficiency Pathophysiology (mechanism) Symptoms Lab findings
 Symptoms Lab findings")
3
Introduction FUNCTION OF G6PD Regenerates NADPH, allowing regeneration of glutathione Protects against oxidative stress Lack of G6PD leads to hemolysis during oxidative stress- infection, medication, fava beans Oxidative stress leads to Heinz body formation, extravascular hemolysis

4
History & Definition It was discovered in 1950s after it was observed that some black soldiers receiving antimalarial drug primaquine developed hemolytic anemia. It is the most common red cell enzymopathy associated with hemolysis. Large no. of abnormal genes code for the G6PD The inheritance of either of them results in this disorder.

5
Definition X-linked disease, sesult in G6PD Deficiency (RBCs enzym deficiency ) asymptomatic unless Oxidative stress causes the RBC’s to break apart. Inherited –, Recessive

6
Genetics The G6PD gene is located on the X chromosome Thus the deficiency state is a sex-linked trait Affected males inherit the abnormal gene from their mothers who are usually carriers (heterozygotes)
")
7
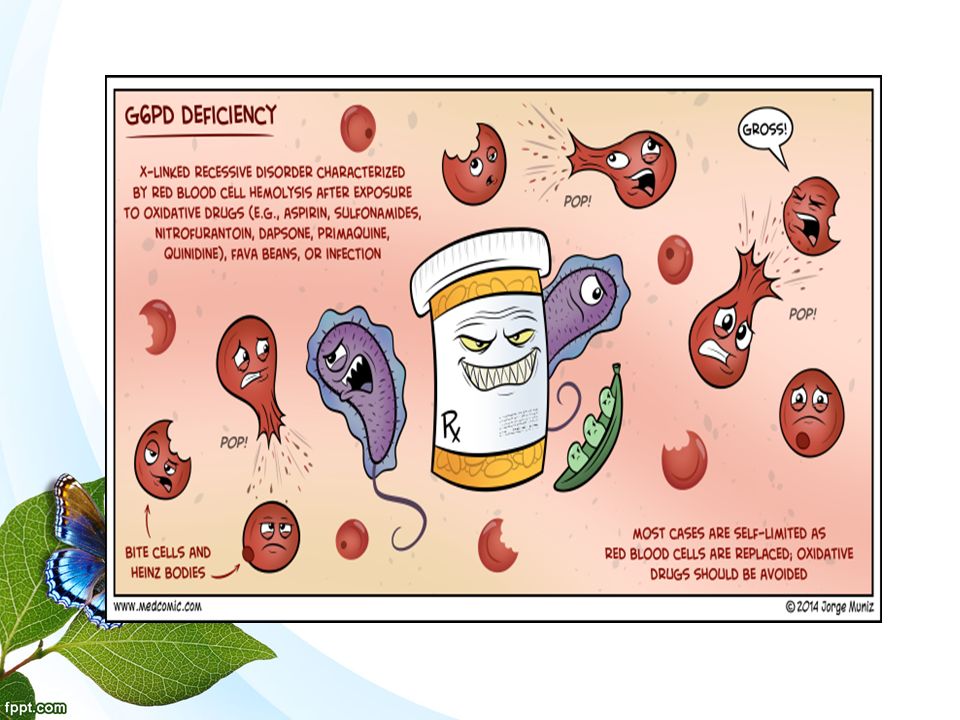
G6PD Deficiency

8
Individuals who have inherited one of the many G6PD mutations do not show clinical manifestation. Some of patients with G6PD develop hemolytic anemia if they are exposed or ingest any of the followings oxidizing agents: 1-Oxidant drugs 1-Oxidant drugs: Remember “AAA”? Antibiotics Antibiotics : e.g. sulfamethoxazole Antimalarias Antimalarias : e.g. primaquine Antipyretics Antipyretics : e.g. acetanilid 2- Favism: The hemolytic effect of ingesting of fava beans is not observed in all individuals with G6PD deficiency but all patients with favism have G6PD deficiency factors cause G6PD deficiency: factors cause G6PD deficiency:

9
G6PD Deficiency Biochemistry – summary G6PD Reduces NADP + to NADPH Which is responsible for Glutathione Which fights Free radicals Which damage blood cells

10
Pathophysiology Oxidative denaturation of hemoglobin is the major cause of H. A in G6PD deficiency It is important in the conversion of glucose-6- P to phosphogluconate For subsequent production of NADPH & reduced glutathione (GSH) GSH protects enzymes & hemoglobin against oxidation by reducing H2O2 & free radicals
 GSH protects enzymes & hemoglobin against oxidation by reducing H2O2 & free radicals.")
11
Pathophysiology H2O2 is generated normally in small amounts during normal red cell metabolism Larger amounts produced when an oxidant drug interacts with oxyhemoglobin Normal red cells have sufficient G6PD activity to maintain adequate GSH levels When deficient, red cells fail to produces sufficient G6PD to detoxify peroxide

12
Pathophysiology Hb is then oxidized to Hi, heme is liberated from globin & globin denatures producing Heinz bodies Heinz bodies attach to membrane sulfhydryl groups inducing cell rigidity At this point red cells can no longer traverse the splenic microcirculation Hence lysis occurs

13
Symptoms Persons with this condition do not display any signs of the disease until their red blood cells are exposed to certain chemicals in food or medicine, or to stress. Symptoms are more common in men and may include: Dark urine Enlarged spleen Fatigue Pallor Rapid heart rate Shortness of breath Yellow skin color (jaundice)
.")
14
G6PD Deficiency Malaria Treatment –c–chloroquine –a–atovaquone-proguanil (Malarone®) –a–artemether-lumefantrine (Coartem®) –m–mefloquine (Lariam®) –q–quinine –q–quinidine –d–doxycycline (used in combination with quinine) –c–clindamycin (used in combination with quinine) –p–primaquine
 –a–artemether-lumefantrine (Coartem®) –m–mefloquine (Lariam®) –q–quinine –q–quinidine –d–doxycycline (used in combination with quinine) –c–clindamycin (used in combination with quinine) –p–primaquine")
15
Diagnosis of G6PD Deficiency Hemolytic Anemia 1-CBC Bite cells, blister cells, irregular small cells, Heinz bodies, polychromasia G-6-PD level Bite” cells Spleen removes portion of RBC that had Heinz body, preventing intravascular hemolysis 2-Screening: Qualitative assessment of G6PD enzymatic activity (UV-based test) 3-Confirmatory test: Quantitative measurement of G6PD enzymatic activity 4-Molecular test: Detection of G6PD gene mutation
 3-Confirmatory test: Quantitative measurement of G6PD enzymatic activity 4-Molecular test: Detection of G6PD gene mutation")
17
Special test Methemoglobin reduction test Methemoglobin reduction

18
Methemoglobin Reduction Test Sodium nitrite converts Hb (hemoglobin) to Hi (methemoglobin) Adding methylene blue should stimulate the pentose phosphate pathway, reducing methemoglobin In G6PD Deficiency, methemoglobin persists
 to Hi (methemoglobin) Adding methylene blue should stimulate the pentose phosphate pathway, reducing methemoglobin In G6PD Deficiency, methemoglobin persists")
19
Methemoglobin Reduction Test Normal blood → clear red color Deficient blood → brown color Deficient blood Normal blood

20
Clinical Manifestations The patient may experience an acute hemolytic crisis within hours of exposure to the oxidant stress Hemolytic crisis is self-limited even if the exposure continues & Only older cell population is rapidly destroyed A minority of patients are sensitive to exposure to fava beans (favism phenomenon)
")
21
What is PNH? Paroxysmal – sudden onset Nocturnal – occuring at night (or early in morning upon awakeneing) Hemoglobinuria Despite the name, most patients do not present this way.
 Hemoglobinuria Despite the name, most patients do not present this way..")
22
What is PNH? A rare and unusual acquired hematologic disorder characterized by – Intravascular hemolysis – Bone marrow failure (cytopenias) – Thrombosis.
 – Thrombosis..")
23
What is PNH? A rare and unusual acquired hematologic disorder characterized by – Intravascular hemolysis – Bone marrow failure (cytopenias) – Thrombosis
 – Thrombosis.")
24
What causes PNH? PNH is due to a change (mutation) in a single gene in a bone marrow “stem” cell. PNH is due to a condition that allows this mutated cell to become the dominant cell in the bone marrow.

25
Paroxysmal nocturnal hemoglobinuria 1. Pathogenesis - an acquired clonal disease, arising from a somatic mutation in a single abnormal stem cell - glycosyl-phosphatidyl- inositol (GPI) anchor abnormality - deficiency of the GPI anchored membrane proteins (decay-accelerating factor =CD55 and a membrane inhibitor of reactive lysis =CD59) - red cells are more sensitive to the lytic effect of complement - intravascular hemolysis 2. Symptoms - passage of dark brown urine in the morning.
 anchor abnormality - deficiency of the GPI anchored membrane proteins (decay-accelerating factor =CD55 and a membrane inhibitor of reactive lysis =CD59) - red cells are more sensitive to the lytic effect of complement - intravascular hemolysis 2. Symptoms - passage of dark brown urine in the morning..")
26
3. PNH –laboratory features: - pancytopenia - chronic urinary iron loss - serum iron concentration decreased - hemoglobinuria - hemosiderinuria - positive Ham’s test (acid hemolysis test) - positive sugar-water test - specific immunophenotype of erytrocytes (CD59, CD55)
 - positive sugar-water test - specific immunophenotype of erytrocytes (CD59, CD55).")
Similar presentations






 vs extracorpuscular Examples of.>")










Sickle-cell anaemia 鐮刀形紅血球貧血症.>")

>")
 Glucose-6-P undergoes two oxidations by NADP +, the second.>")