Download presentation
Presentation is loading. Please wait.

1
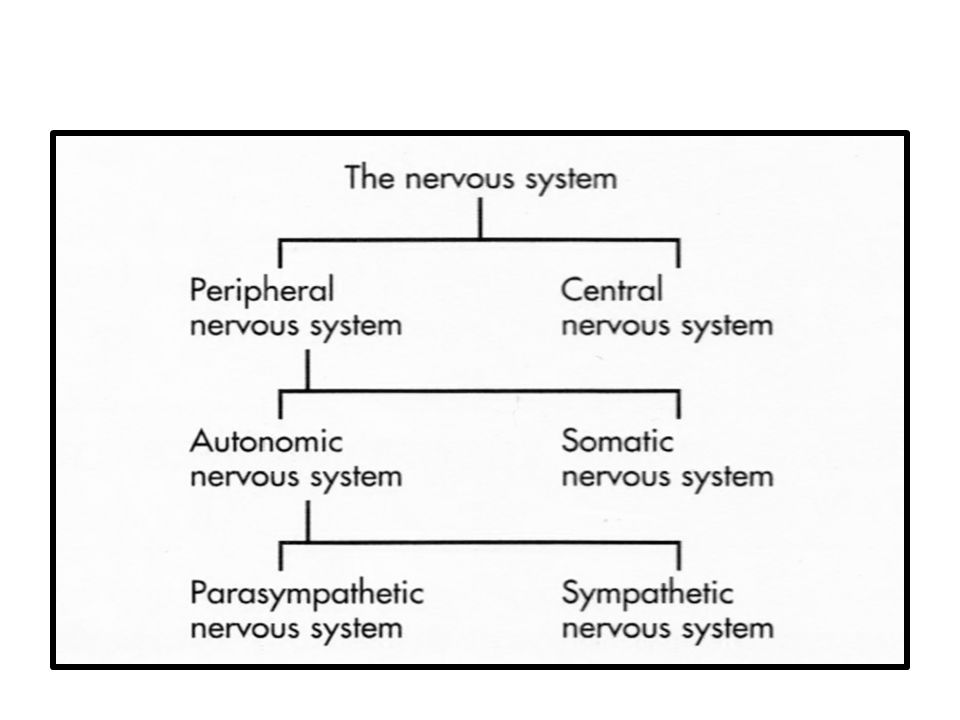
Introduction to Autonomic nervous system

5
Comparison of Somatic and Autonomic Systems

6
TRANSMITTERS OF ANS: Acetylcholine is the neurotransmitter of:
preganglionic nerves of both parasympathetic and sympathetic nervous system. postganlionic nerves of parasympathetic nerves system.

8
TRANSMITTERS OF ANS: Sympathetic nervous system:
Norepinephrine is the major nerve transmitter of postganglionic nerves Acetylcholine is the nerve transmitter of postganlionic nerves of sympathetic nervous system supplying sweat glands.

9
PARASYMPATHETIC NS: SYMPATHETIC NS:
The preganglionic nerves arise from 1. Midbrain – III cranial nerve. 2. Medulla – VII, IX and X cranial nerve. 3. Sacral part of spinal cord – S - 2, 3, 4 SYMPATHETIC NS: The preganglionic fibers originate from the thoracolumbar region of the spinal cord.

12
Drugs affecting ANS Two groups of ANS drugs:
The cholinergic drugs: acetylcholine (ACh) receptors The adrenergic drugs: adrenergic receptors
 receptors. The adrenergic drugs: adrenergic receptors.")
13
Cholinergic Agonists

15
THE CHOLINERGIC NEURON
Fibers using Ach as a neurotransmitter: The preganglionic fibers terminating in the adrenal medulla The autonomic ganglia (both parasympathetic and sympathetic) The post-ganglionic fibers of the parasympathetic division. The postganglionic sympathetic division of sweat glands use acetylcholine. Cholinergic neurons innervate the muscles of the somatic system
 The post-ganglionic fibers of the parasympathetic division. The postganglionic sympathetic division of sweat glands use acetylcholine. Cholinergic neurons innervate the muscles of the somatic system.")
17
Cholinergic neurons in the CNS:
Alzheimer disease: a significant loss of cholinergic neurons in the temporal lobe and entorhinal cortex. Most of the drugs available to treat the disease are acetylcholinesterase (AChE) inhibitors.
 inhibitors.")
18
A. Neurotransmission at cholinergic neurons
Six sequential steps: synthesis storage release binding of ACh to a receptor degradation of the neurotransmitter in the synaptic cleft recycling of choline and acetate

20
Synthesis of acetylcholine:
Choline uptake: by an energy-dependent carrier system that cotransports sodium is the rate-limiting step in ACh synthesis. Choline acetyl-transferase (CAT) Choline + acetyl coenzyme A ACh
 Choline + acetyl coenzyme A. ACh.")
21
2. Storage of acetylcholine in vesicles:
by an active transport process coupled to the efflux of protons. Vesicles contain the primary neurotransmitter (here, ACh) as well as a cotransmitter that will increase or decrease the effect of the primary neurotransmitter. Vesicle contains: ACh, ATP, proteoglycan.
 as well as a cotransmitter that will increase or decrease the effect of the primary neurotransmitter. Vesicle contains: ACh, ATP, proteoglycan.")
22
Release of acetylcholine:
When an action potential arrives at a nerve ending, voltage-sensitive calcium channels on the presynaptic membrane open, causing an increase in the concentration of intracellular calcium. This will promote the fusion of synaptic vesicles with the cell membrane and the release of their contents into the synaptic space.

23
4. Binding to the receptor:
ACh diffuses across the synaptic space and binds: to post-synaptic receptors on the target cell to presynaptic receptors in the membrane of the neuron that released the ACh, or to other targeted presynaptic receptors. The postsynaptic receptors: muscarinic and nicotinic. Binding to a receptor leads to a biologic response within the cell

24
5. Degradation of acetylcholine:
Termination of the signal at the postjunctional effector site : is rapid by AChE Butyrylcholinesterase (pseudocholinesterase), is found in the plasma but does not play a significant role in the termination of ACh’s effect in the synapse. AChE ACh Choline acetate
, is found in the plasma but does not play a significant role in the termination of ACh’s effect in the synapse. AChE. ACh. Choline + acetate.")
25
6. Recycling of choline: Choline may be recaptured by a sodium-coupled, high-affinity uptake system that transports the molecule back into the neuron. There, it is acetylated into ACh that is stored until released by a subsequent action potential.

26
CHOLINERGIC RECEPTORS (CHOLINOCEPTORS)
Two families of cholinoceptors Muscarinic Nicotinic

28
A. Muscarinic receptors
Muscarinic receptors: GPCR They show only a weak affinity for nicotine. Five subclasses of muscarinic receptors: M1, M2, M3, M4, and M5. Only M1, M2, and M3 receptors have been functionally characterized.

29
1. Locations of muscarinic receptors:
Located on: ganglia of the peripheral nervous system the autonomic effector organs, such as the heart, smooth muscle, brain, and exocrine glands. M1: neural, also found on gastric parietal cells (excitatory; Gq) M2: cardiac cells and smooth muscle (inhibitory; Gi) M3: bladder, exocrine glands, and smooth muscle. (excitatory; Gq)
 M2: cardiac cells and smooth muscle (inhibitory; Gi) M3: bladder, exocrine glands, and smooth muscle. (excitatory; Gq)")
30
Mechanisms of acetylcholine signal transduction:
“glandular” “neural” “cardiac” Membrane depolarization (decrease of M1 activity in CNS may be a cause of dementia) Mostly inhibitory (responsible for the vagal inhibition of the heart) Mostly excitatory (stimulation of glandular secretion, contraction of visceral smooth muscle)
 Mostly inhibitory (responsible for the vagal inhibition of the heart) Mostly excitatory (stimulation of glandular. secretion, contraction of visceral smooth muscle)")
31
3. Muscarinic agonists and antagonists:
Development of specific muscarinic agonists and antagonists is underway: Pirenzepine: inhibits M1 muscarinic receptors, such as in the gastric mucosa. Decrease acid secretion Darifenacin is a competitive M3 receptor antagonist. The drug is used in the treatment of overactive bladder. At present, no clinically important agents interact solely with the M4 and M5 receptors.

32
Nicotinic receptors Pentameric receptor comprised of 4 different subunits: α2, β, γ, δ Found in autonomic ganglions, adrenal medulla, neuromuscular junction and CNS Ligand-gated ion (Na+) channel. Ach binds to the α subunits Channel opening requires binding of 2 Ach molecules Blocking gaglionic nAChR blocks all autonomic outflow. These agents lack selectivity and are now used mostly in research laboratories These blocking agents include: Hexamethonium, tetraethylammonium, mecamylamine, and trimethaphan
 channel. Ach binds to the α subunits. Channel opening requires binding of 2 Ach molecules. Blocking gaglionic nAChR blocks all autonomic outflow. These agents lack selectivity and are now used mostly in research laboratories. These blocking agents include: Hexamethonium, tetraethylammonium, mecamylamine, and trimethaphan.")
33
at low concentration stimulates the receptor
Nicotine at low concentration stimulates the receptor at high concentration blocks the receptor. Locations of nicotinic receptors: CNS adrenal medulla autonomic ganglia neuromuscular junction (NMJ). Those at the NMJ are designated NM Receptors at other sites are designated NN.
. Those at the NMJ are designated NM. Receptors at other sites are designated NN.")
35
The nicotinic receptors of autonomic ganglia differ from those of the NMJ.
Ganglionic receptors are selectively blocked by hexamethonium NMJ receptors are specifically blocked by tubocurarine.

37
Cholinergic agonists

39
DIRECT-ACTING CHOLINERGIC AGONISTS (Parasympathomimetics)
Classified into two groups: Choline esters include: Ach, synthetic esters of choline such as carbachol and bethanechol. Naturally occurring alkaloids, such as pilocarpine.

40
All have longer durations of action than ACh.
Some of these drugs (pilocarpine and bethanechol) preferentially bind to muscarinic receptors and are sometimes referred to as muscarinic agents. They show little specificity in their actions, which limits their clinical usefulness.
 preferentially bind to muscarinic receptors and are sometimes referred to as muscarinic agents. They show little specificity in their actions, which limits their clinical usefulness.")
41
A. Acetylcholine a quaternary ammonium compound.
lacks therapeutic importance because: multiplicity of actions (leading to diffuse effects) its rapid inactivation by the cholinesterases. ACh has both muscarinic and nicotinic activity.
 its rapid inactivation by the cholinesterases. ACh has both muscarinic and nicotinic activity.")
42
Actions of ACh: 1. Decreases heart rate and cardiac output (Effect mimic the effects of vagal stimulation) 2. Decrease in blood pressure: Causes vasodilation and lowering of blood pressure by an indirect mechanism of action. Atropine blocks these muscarinic receptors and prevents ACh from producing vasodilation. M3

43
3. Other actions: GI tract: Respiratory tract: Genitourinary tract:
ACh increases salivary secretion ACh stimulates intestinal secretions and motility. Respiratory tract: enhances bronchiolar secretions. Genitourinary tract: ACh increases the tone of the detrusor urinae muscle, causing expulsion of urine. In the eye: ACh causes miosis (marked constriction of the pupil). ACh (1% solution) is instilled into the anterior chamber of the eye to produce miosis during ophthalmic surgery.
. ACh (1% solution) is instilled into the anterior chamber of the eye to produce miosis during ophthalmic surgery.")
44
B. Bethanechol Structurally related to Ach
it is not hydrolyzed by AChE have muscarinic activity only. Its major actions are on the smooth musculature of the bladder and GI tract. Duration of action: 1-hour.

45
Actions of Bethanechol:
It increases intestinal motility and tone. It stimulates the detrusor muscle of the bladder, whereas the trigone and sphincter are relaxed.

46
Therapeutic applications:
Used to stimulate the atonic bladder (A large dilated urinary bladder that does not empty, usually due to disturbance of innervation or to chronic obstruction.), particularly in postpartum or postoperative, nonobstructive urinary retention. to treat neurogenic atony as well as megacolon.
, particularly in postpartum or postoperative, nonobstructive urinary retention. to treat neurogenic atony as well as megacolon.")
47
Atonic neurogenic bladder :
Neurogenic bladder due to destruction of sensory nerve fibers from the bladder to the spinal cord, with absence of control of bladder functions and of desire to urinate, bladder overdistention, and an abnormal amount of residual urine

48
3. Adverse effects of bethanechol:
Generalized cholinergic stimulation: Sweating, salivation, flushing, decreased blood pressure, nausea, abdominal pain, diarrhea, and bronchospasm. Atropine sulfate (antagonist) may be administered to overcome severe cardiovascular or bronchoconstrictor responses to this agent.
 may be administered to overcome severe cardiovascular or bronchoconstrictor responses to this agent.")
50
C. Carbachol (carbamylcholine)
Has both muscarinic & nicotinic actions. Actions: Carbachol has profound effects on both the cardiovascular and GI systems because of its ganglion-stimulating activity, and it may first stimulate and then depress these systems. It can cause release of epinephrine from the adrenal medulla by its nicotinic action. Locally instilled into the eye, it mimics the effects of ACh, causing miosis and a spasm of accommodation in which the ciliary muscle of the eye remains in a constant state of contraction.

51
2. Therapeutic uses of Carbachol:
Rarely used therapeutically because of: its high potency receptor nonselectivity relatively long duration of action Can be used in the eye as a miotic agent to treat glaucoma by: causing pupillary contraction a decrease in intraocular pressure. Onset of action for miosis is 10 to 20 minutes. Intraocular pressure is reduced for 4 to 8 hours.

52
3. Adverse effects of carbachol:
At doses used ophthalmologically, little or no side effects occur due to lack of systemic penetration (quaternary amine).
.")
53
D. Pilocarpine The alkaloid pilocarpine is stable to hydrolysis by AChE. Less potent than ACh Uncharged and will penetrate the CNS at therapeutic doses. Pilocarpine exhibits muscarinic activity and is used primarily in ophthalmology.

54
1. Actions: When applied topically produces rapid miosis and contraction of the ciliary muscle. Potent stimulators of secretions such as sweat, tears, and saliva

56
Therapeutic use of Pilocarpine: 1. in glaucoma:
The drug of choice in the emergency lowering of intraocular pressure of both: narrow-angle (or closed-angle) wide-angle (also called open-angle) glaucoma. It opens the trabecular meshwork around Schlemm’s canal, causing an immediate drop in intraocular pressure as a result of the increased drainage of aqueous humor.
 wide-angle (also called open-angle) glaucoma. It opens the trabecular meshwork around Schlemm’s canal, causing an immediate drop in intraocular pressure as a result of the increased drainage of aqueous humor.")
58
Onset of action: few minutes
Duration of action: 4 to 8 hours The miotic action of pilocarpine is also useful in reversing mydriasis due to atropine.

59
Pilocarpine is used to promote salivation:
in patients with xerostomia. In Sjögren’s syndrome, which is characterized by dry mouth and lack of tears.

60
3. Adverse effects of pilocarpine
Cause CNS disturbances. Poisoning with this agent is characterized by exaggeration of various parasympathetic effects, including profuse sweating (diaphoresis) and salivation. The effects are similar to those produced by consumption of mushrooms of the genus Inocybe. Parenteral atropine is administered to counteract the toxicity of pilocarpine.
 and salivation. The effects are similar to those produced by consumption of mushrooms of the genus Inocybe. Parenteral atropine is administered to counteract the toxicity of pilocarpine.")
63
INDIRECT-ACTING CHOLINERGIC AGONISTS: ACETYLCHOLINESTERASE INHIBITORS (REVERSIBLE)
AChE is located both pre- and postsynaptically in the nerve terminal where it is membrane bound. Inhibitors of AChE results in the accumulation of ACh in the synaptic space. The reversible AChE inhibitors can be classified as: short-acting agents intermediate-acting agents

65
A. Edrophonium The prototype short-acting AChE inhibitor.
It is rapidly absorbed Short duration of action: 10 to 20 minutes due to rapid renal elimination. Edrophonium is a quaternary amine, and its actions are limited to the periphery.

66
Uses of Edrophonium in the diagnosis of myasthenia gravis, which is an autoimmune disease caused by antibodies to the nicotinic receptor at NMJs. This causes their degradation, making fewer receptors available for interaction with the neurotransmitter. Intravenous injection of edrophonium leads to a rapid increase in muscle strength.

67
Edrophonium may also be used:
to assess cholinesterase inhibitor therapy for differentiating cholinergic and myasthenic crises for reversing the effects of nondepolarizing neuromuscular blockers after surgery.

68
Tensilon test Edrophonium is used to differentiate myasthenia gravis from cholinergic crisis.

69
B. Physostigmine Found naturally in plants and is a tertiary amine.
It is a substrate for AChE, and it forms a relatively stable carbamoylated intermediate with the enzyme, which then becomes reversibly inactivated. The result is potentiation of cholinergic activity throughout the body.

70
Actions: Physostigmine stimulates the muscarinic and nicotinic sites of the ANS but also the nicotinic receptors of the NMJ. Its duration of action is about 2 to 4 hours, and it is considered to be an intermediate-acting agent. Physostigmine can enter and stimulate the cholinergic sites in the CNS.

71
2. Therapeutic uses: In atony of intestine and bladder. Placed topically in the eye it produces miosis spasm of accommodation lowering of intraocular pressure. It is used to treat glaucoma, but pilocarpine is more effective. Physostigmine is also used in the treatment of overdoses of drugs with anticholinergic actions, such as atropine, phenothiazines, and tricyclic antidepressants.

72
CNS effects of physostigmine: convulsions with high doses. Periphery:
3. Adverse effects: CNS effects of physostigmine: convulsions with high doses. Periphery: Bradycardia fall in cardiac output Skeletal NMJ: causes the accumulation of ACh and results in paralysis of skeletal muscle.

74
C. Neostigmine Neostigmine reversibly inhibits AChE in similar to that of physostigmine. 2. Therapeutic uses: It is used to stimulate the bladder and GI tract an antidote for tubocurarine and other competitive neuromuscular-blocking agents Used symptomatically to treat myasthenia gravis. Actions: Neostigmine has a quaternary nitrogen. Therefore, it is more polar, is absorbed poorly from the GI tract, and does not enter the CNS. Its effect on skeletal muscle is greater than that of physostigmine, and it can stimulate contractility before it paralyzes. Intermediate duration of action: 30 minutes to 2 hours.

75
3. Adverse effects: Symptoms of generalized cholinergic stimulation, such as salivation, fushing, decreased blood pressure, nausea, abdominal pain, diarrhea, and bronchospasm.

76
D. Pyridostigmine and ambenonium
They used in the chronic management of myasthenia gravis. Durations of action: are intermediate 3 to 6 hours : pyridostigmine 4 to 8 hours: ambenonium Adverse effects: similar to those of neostigmine.

77
E. Tacrine, donepezil, rivastigmine, and galantamine
Centrally acting reversible acetylcholinesterase inhibitors Tacrine : hepatotoxic Used in the treatment of Alzheimer disease The cannot stop the progression of Alzheimer disease Adverse effects: GI distress

78
INDIRECT-ACTING CHOLINERGIC AGONISTS: ANTICHOLINESTERASES (IRREVERSIBLE)
Synthetic organophosphate compounds They bind covalently to AChE. The result is a long-lasting increase in ACh at all sites where it is released. Many of these drugs are extremely toxic and were developed by the military as nerve agents. Related compounds, such as parathion, are used as insecticides.

79
Mechanism of action: A. Echothiophate
Following covalent modification of AChE, the phosphorylated enzyme slowly releases one of its ethyl groups. The loss of an alkyl group, which is called aging, makes it impossible for chemical reactivators, such as pralidoxime, to break the bond between the remaining drug and the enzyme.

80
2. Actions: 3. Therapeutic uses:
Generalized cholinergic stimulation paralysis of motor function (causing breathing difficulties) Convulsions intense miosis Decreases intraocular pressure through the facilitation of outflow of aqueous humor Atropine in high dosages can reverse many of the muscarinic and some of the central effects of echothiophate. 3. Therapeutic uses: Chronic treatment of open-angle glaucoma. Echothiophate is not a first-line agent in the treatment of glaucoma. Has the potential risk for causing cataracts.
 Convulsions. intense miosis. Decreases intraocular pressure through the facilitation of outflow of aqueous humor. Atropine in high dosages can reverse many of the muscarinic and some of the central effects of echothiophate. 3. Therapeutic uses: Chronic treatment of open-angle glaucoma. Echothiophate is not a first-line agent in the treatment of glaucoma. Has the potential risk for causing cataracts.")
82
TOXICOLOGY OF ACETYLCHOLINESTERASE INHIBITORS
AChE inhibitors are commonly used as agricultural insecticides Numerous cases of accidental intoxication with these agents. Toxicity with these agents is manifested as nicotinic and muscarinic signs and symptoms.

83
A. Reactivation of acetylcholinesterase:
Pralidoxime can reactivate inhibited AChE. It is does not penetrate into the CNS. The presence of a charged group allows it to approach an anionic site on the enzyme, where it essentially displaces the phosphate group of the organophosphate and regenerates the enzyme. If given before aging, it can reverse the effects of echothiophate, except for those in the CNS.

84
Pralidoxime is a weak AChE inhibitor and, at higher doses, may cause side effects similar to other AChE inhibitors. In addition, it cannot overcome toxicity of reversible AChE inhibitors (for example, physostigmine).
.")
87
B. Other treatments: Atropine: to prevent muscarinic side effects which include: increased bronchial secretion and saliva Bronchoconstriction bradycardia Diazepam: to reduce the persistent convulsion caused by these agents.

88
C. General supportive measures may be necessary:
maintenance of patent airway oxygen supply artificial respiration, may be necessary as well.

Similar presentations

























 Drugs>")
 AUTONOMIC NERVOUS SYSTEM PHARMACOLOGY.>")











 Sensory.>")


