Download presentation
Presentation is loading. Please wait.

1
Detection and Treatment of Non-Melanoma Skin Cancers
Toby Maurer, MD University of California, San Francisco

2
Basics of Skin Cancer Large majority caused by sun exposure
Often sun exposure before age 20 Persons who burn easily and tan poorly are at greatest risk

5
Sunscreen Don’t forget sun-protective clothing Physical sunscreen
zinc oxide and titanium dioxide thick and more waterproof fewer allergic reactions Chemical sunscreens burns if gets into eyes more comedonegenic

6
Sunscreen Apply 1/2 hr. before going out
May need to reapply every 2-3 hours especially if going in water Be liberal with amount UVA protection probably added benefit

7
Non-Melanoma Skin Cancers
Basal cell carcinoma (BCC) Actinic keratosis (AK) Squamous cell carcinoma (SCC)
 Actinic keratosis (AK) Squamous cell carcinoma (SCC)")
8
Basal Cell Carcinoma (BCC)
Who is at Risk? Age 20+ Fair-skinned persons Sun-exposed sites over 50% on face

15
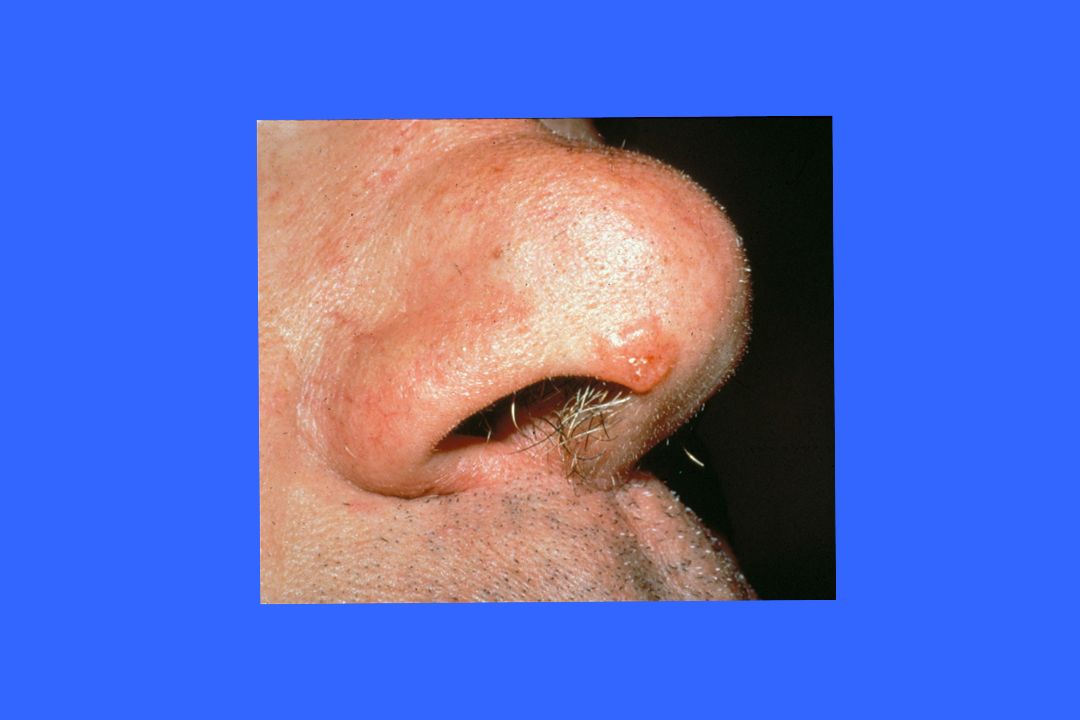
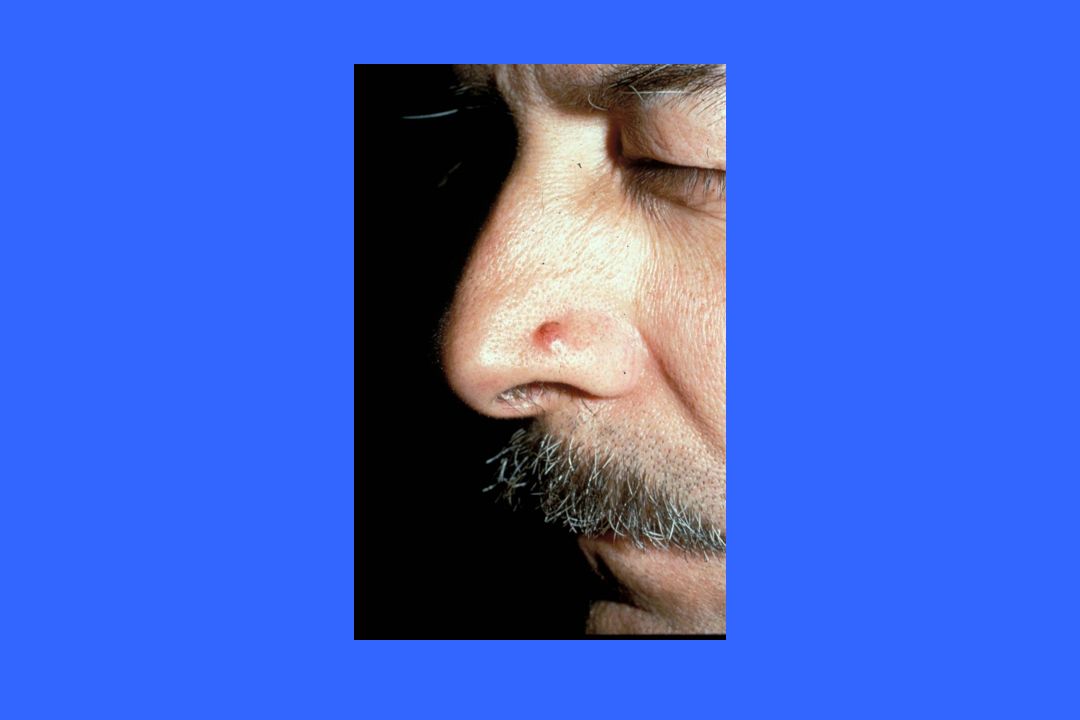
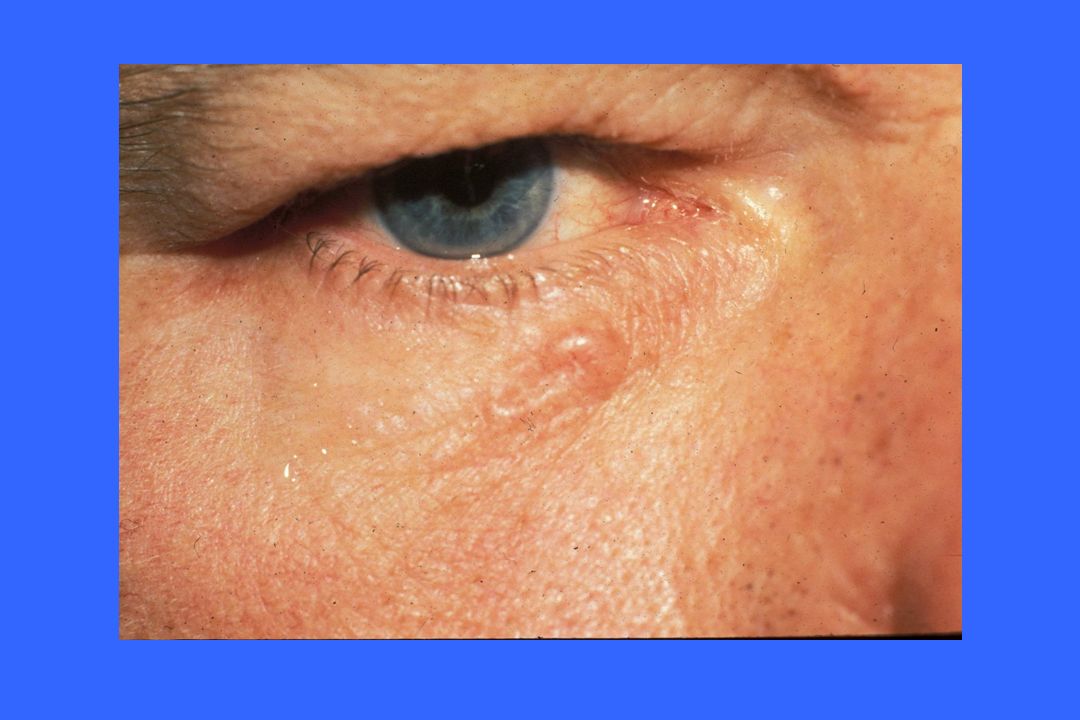
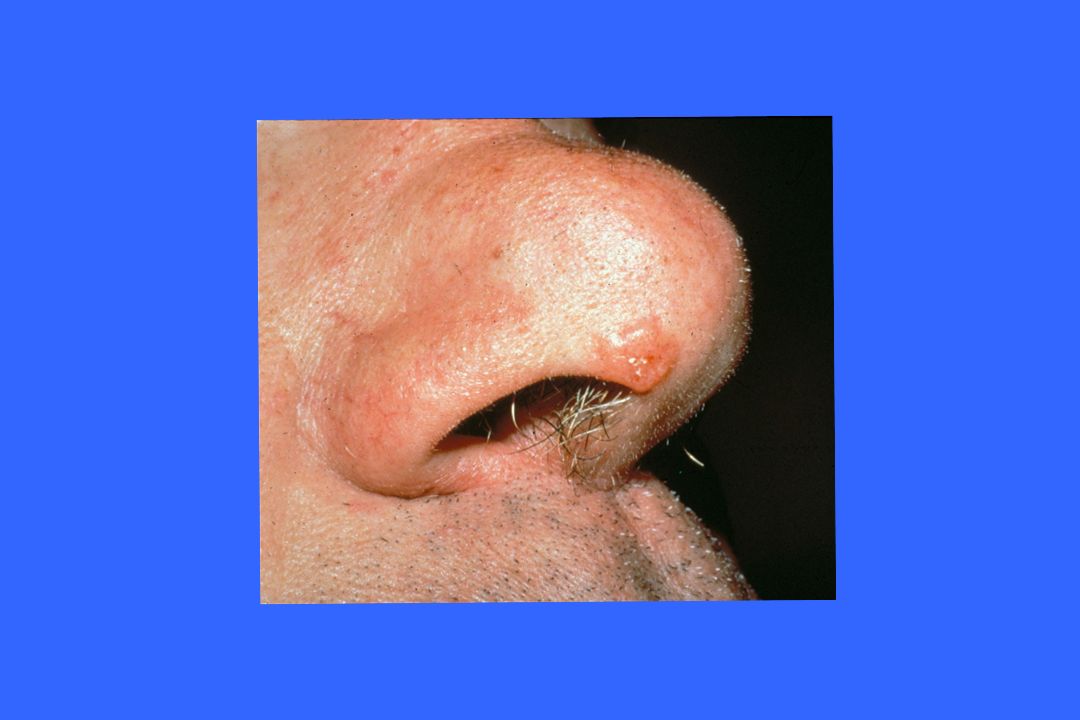
Clinical Features of BCC
Pearly papule with telangiectasia (face, ears forehead, neck) Scaly red patch (back, chest, legs of women) Sclerotic (scarlike) lesion Pigmented in pigmented races (blacks, etc.) May erode or ulcerate
 Scaly red patch (back, chest, legs of women) Sclerotic (scarlike) lesion. Pigmented in pigmented races (blacks, etc.) May erode or ulcerate.")
16
Diagnosis of BCC: Shave or Punch Biopsy

17
Differential Diagnosis of BCC
Intradermal Nevus Sebaceous hypersplasia Fibrous Papule (angiofibroma) Eczema Melanoma
 Eczema. Melanoma.")
28
Recommended Treatment of BCC
Surgical excision (head and neck) Curettage and desiccation (trunk) Radiation therapy (debilitated pt) Microscopically controlled surgery (Mohs) Recurrent/sclerotic BCC’s BCC’s on eyelid and nasal tip
 Curettage and desiccation (trunk) Radiation therapy (debilitated pt) Microscopically controlled surgery (Mohs) Recurrent/sclerotic BCC’s. BCC’s on eyelid and nasal tip.")
29
Aldara (Imiquimod) Topical therapy designed for wart treatment
Upregulates interferon and down regulates tumor necrosis factor Seems to have efficacy in superficial BCC’s Do Not use in BCC’s that are nodular or invasive

30
Topical Treatment of Skin Cancer
Imiquimod 5% cream can effectively treat superficial BCC’s and SCC in situ Treatment regimen is 5X per week for 6-10 weeks depending on the host reaction Efficacy is relatively high (75%-85%) Scarring may be reduced compared to surgery Other possible uses: Extramammary Paget’s, lentigo maligna (trials needed)
 Scarring may be reduced compared to surgery. Other possible uses: Extramammary Paget’s, lentigo maligna (trials needed)")
31
Topical Treatment of Skin Cancer
Patient selection is the key Biopsy to confirm diagnosis before TX

32
Treatments NOT Recommended
Cryotherapy Topical chemotherapy - 5 Fleurourical (Efudex) Radiation therapy (age < 65)
 Radiation therapy (age < 65)")
33
When to Refer It depends on your surgical skills > 1 cm
Sclerotic BCC Recurrent BCC Eyelid BCC

34
Actinic Keratosis (AK)
Who is at risk? Over age 35-40 Fair-skinned persons Sun-exposed sites Face, forearms, hands, upper trunk History of chronic sun exposure

35
Clinical Features of AK
Red, adherent, scaly lesions, usually < 5mm Sandpapery, rough texture Tender when touched or shaved Thick, warty character (cutaneous horn)
")
40
Diagnosis of AK Diagnosis Differential Diagnosis Clinical features
Shave or punch biopsy Differential Diagnosis BCC/SCC Seborrheic keratosis Wart

43
Treatment of AK Cryotherapy Topical chemotherapy/chemical peel
Efudex (5FU crème) 2x’s/day x 6 wks or Imiquimod-3X’s /wk and 3 mos. When to refer? Too extensive for local treatment Consider biopsy or referral with any lesion that doesn’t resolve with cryotherapy
 2x’s/day x 6 wks or Imiquimod-3X’s /wk and 3 mos. When to refer Too extensive for local treatment. Consider biopsy or referral with any lesion that doesn’t resolve with cryotherapy.")
45
Make sure you know what you are treating
Be very careful with pigmented lesions

46
Rule of thumb for cryotherapy:
make sure lesion resolves after one month if not, refer or biopsy to rule out malignancy

47
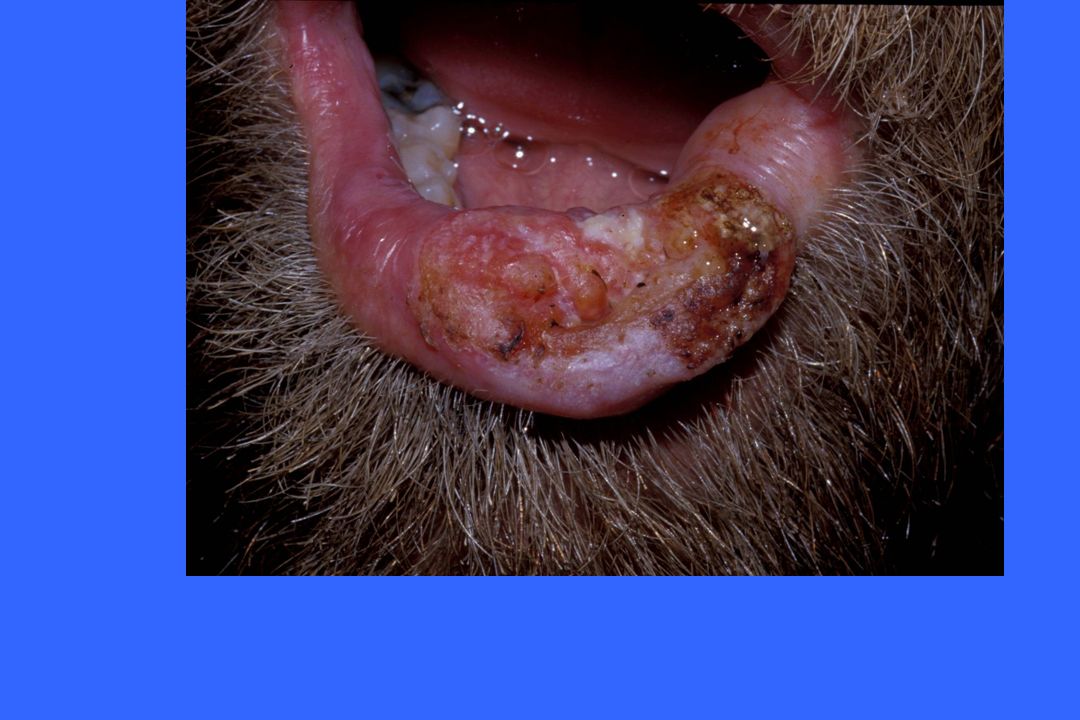
Squamous Cell Carcinoma (SCC)
Who is at risk? Age 50+ Chronic sun exposure Head, neck, lower lip, ears, dorsal hands, trunk Special circumstances Immunosuppression (organ transplant) Radiation therapy
 Radiation therapy.")
48
Clinical Features of SCC
Papule, nodule or tumor Non-healing erosion or ulcer Cutaneous horn (wart-like lesion) Fixed, red, scaling patch/plaque (Bowen’s-SCC-in-situ)
 Fixed, red, scaling patch/plaque (Bowen’s-SCC-in-situ)")
54
Differential Diagnosis of SCC
Actinic keratosis Wart Seborrheic keratosis BCC Eczema or psoriasis

61
How to Diagnose Punch or excisional/incisional biopsy
Shave biopsy for flat, non-elevated lesion

62
Treatment of SCC Recommended treatment Treatments NOT recommended
Excision Radiation therapy ( debilitated pt) Treatments NOT recommended Curettage and desiccation Topical chemotherapy
 Treatments NOT recommended. Curettage and desiccation. Topical chemotherapy.")
63
When to Refer SCC’s may metastasize
Low threshold for biopsy and referral Regularly check draining lymph nodes High risk SCC’s

64
High-risk SCC’s Lip Temple
Immunocompromised host (i.e. organ transplant) Area of previous radiation therapy
 Area of previous radiation therapy.")
Similar presentations