Download presentation
Presentation is loading. Please wait.

1
Hemi-Automated Lamellar Keratoplasty (HALK) Leonard Yuen, MD MPH MRCOphth Jodhbir Mehta, FRCS FRCOphth Li Lim, FRCOphth Donald Tan, FRCS FRCOphth SINGAPORE NATIONAL EYE CENTRE (SNEC) The authors have no financial interest in the subject matter of this poster
 Leonard Yuen, MD MPH MRCOphth Jodhbir Mehta, FRCS FRCOphth Li Lim, FRCOphth Donald Tan, FRCS FRCOphth SINGAPORE NATIONAL EYE CENTRE (SNEC) The authors have no financial interest in the subject matter of this poster")
2
Purpose To describe a novel hybrid technique for anterior lamellar keratoplasty in corneas with topographical irregularities The advantages of Anterior lamellar keratoplasty (ALK) is its lower rejection rate and greater trauma resistance compared to PK, together with a reduced risk of endophthalmitis and expulsive haemorrhage. It is technically more demanding and time consuming, however techniques are constantly evolving with increasingly better outcomes. Microkeratome-assisted lamellar keratoplasty is a well-described technique to prepare both recipient and donor beds which reduces the surgical time and allows the preparation of a smooth graft interface. However corneas with significant topographical abnormalities, areas of elevation or thinning, will be reproduced by the microkeratome when creating the recipient flap. It is therefore limited to patients who have stromal pathologies in the anterior-mid stroma and with regular corneal topographies.

3
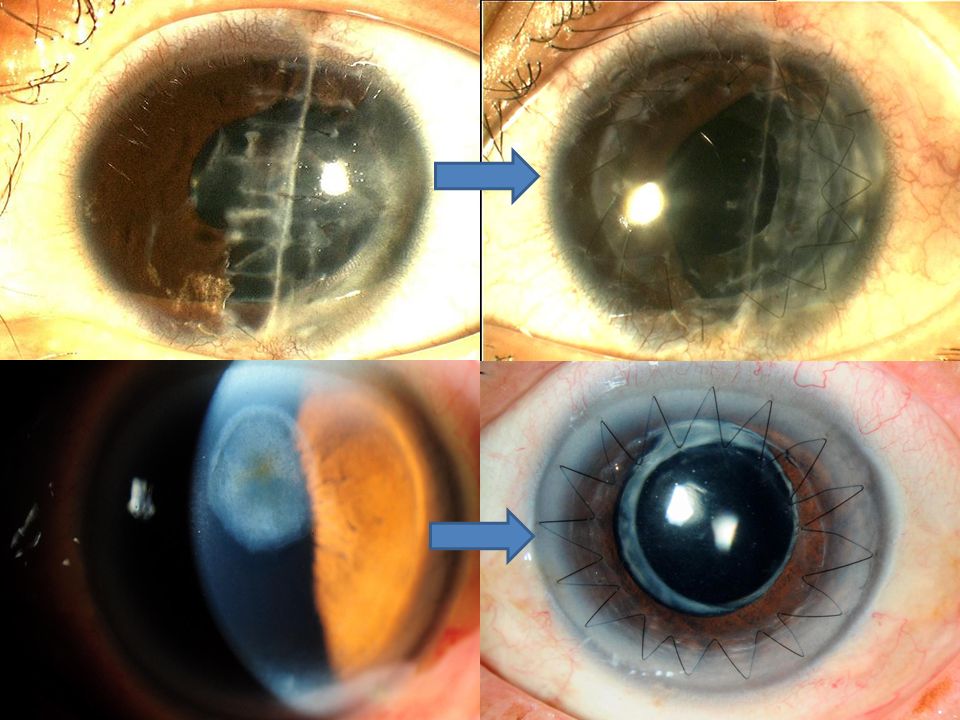
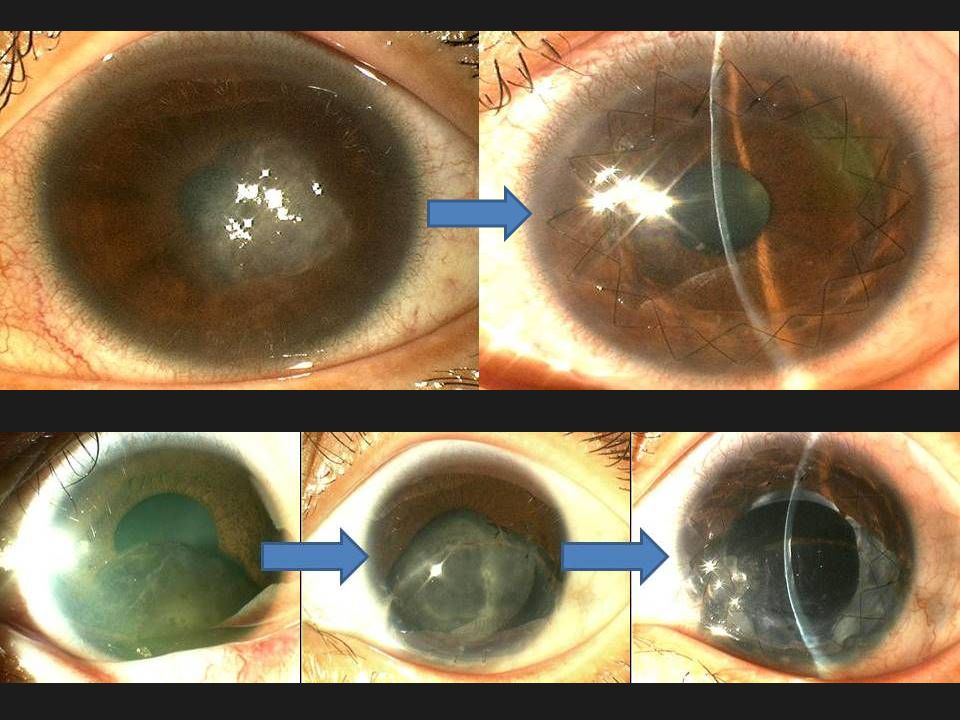
Method Hemi-Automated Lamellar Keratoplasty (HALK), a combined procedure of manual recipient bed lamellar dissection with an automated donor preparation, was performed on 11 eyes of 11 patients with heterogenous causes of anterior stromal scarring All 11 eyes had a minimum of 4 months follow up, with a mean of 9 months (median 8, range, 4 – 12 months) *A subset of 5 eyes had longer follow up of >12 months, with a mean of 19 months (median 17, range, 13-26 months)
, a combined procedure of manual recipient bed lamellar dissection with an automated donor preparation, was performed on 11 eyes of 11 patients with heterogenous causes of anterior stromal scarring All 11 eyes had a minimum of 4 months follow up, with a mean of 9 months (median 8, range, 4 – 12 months) *A subset of 5 eyes had longer follow up of >12 months, with a mean of 19 months (median 17, range, months)")
4
Demographics GenderDate of SurgeryRaceAge Indication 1Female1.Nov.07Indian7 Congenital linear corneal scar 2Male3.Nov.07Vietnamese8 Scar from penetrating injury 3Female31.Jul.07Chinese19 Contact lens keratitis scar (pseduomonas) 4Female31.May.08Chinese10 Post excision of Iris-cornea tumor 5Female9.Jun.08Chinese40 Herpetic disciform keratitis 6Male20.Oct.08Chinese22 Contact lens keratitis scar 7Male2.Jan.09Malay44 Lattice dystrophy 8Male12.Jan.09Indian48 Deep traumatic stromal scar 9Male30.Jun.09Chinese22 Contact lens keratitis scar 10Male11.Jul.09Indian21 Contact lens keratitis scar (pseduomonas) 11Male13.Jul.09Chinese60 Corneal abscess scar Mean age 27.4 years Median 22 (range, 7 – 60)
 4Female31.May.08Chinese10 Post excision of Iris-cornea tumor 5Female9.Jun.08Chinese40 Herpetic disciform keratitis 6Male20.Oct.08Chinese22 Contact lens keratitis scar 7Male2.Jan.09Malay44 Lattice dystrophy 8Male12.Jan.09Indian48 Deep traumatic stromal scar 9Male30.Jun.09Chinese22 Contact lens keratitis scar 10Male11.Jul.09Indian21 Contact lens keratitis scar (pseduomonas) 11Male13.Jul.09Chinese60 Corneal abscess scar Mean age 27.4 years Median 22 (range, 7 – 60)")
5
Results PreoperativePostoperativeP - value Uncorrected Visual Acuity (UCVA, logMAR) 1.23 +/- 0.67 [20/200]* 0.65 +/- 0.28 [20/90]* 0.02 Best Corrected Visual Acuity (BCVA, logMAR) 0.75 +/- 0.63 [20/110]* 0.39 +/- 0.23 [20/50]* 0.10 Sphere (D)0.89 +/- 4.411.66 +/- 2.720.65 Cylinder (D)-3.42 +/- 2.79-3.34 +/- 1.530.94 MRSE (D)-0.82 +/- 3.950.01 +/- 2.760.61 N = 11, mean follow-up time 9 months * Snellen Equivalent
![Results PreoperativePostoperativeP - value Uncorrected Visual Acuity (UCVA, logMAR) / [20/200]* / [20/90]* 0.02 Best Corrected Visual Acuity (BCVA, logMAR) / [20/110]* / [20/50]* 0.10 Sphere (D)0.89 +/ / Cylinder (D) / / MRSE (D) / / N = 11, mean follow-up time 9 months * Snellen Equivalent](http://images.slideplayer.com/23/6671232/slides/slide_5.jpg "Results PreoperativePostoperativeP - value Uncorrected Visual Acuity (UCVA, logMAR) / [20/200]* / [20/90]* 0.02 Best Corrected Visual Acuity (BCVA, logMAR) / [20/110]* / [20/50]* 0.10 Sphere (D)0.89 +/ / Cylinder (D) / / MRSE (D) / / N = 11, mean follow-up time 9 months * Snellen Equivalent")
9
Discussion Postoperative UCVA improved in 82% of eyes Postoperative BCVA improved in 64% of eyes – Mean Snellen BCVA achieved was 20/50 (range, 20/25 – 20/100), comparable with other studies achieving 20/60 1 and 20/70 2 three months after conventional ALTK Postoperative SE was -0.01D – Values between -1.63 and -4.16D have been reported after PK 3,4,5,6 1. Vajpayee RB, Sharma N, Jhanju V, et al. One donor cornea for 3 recipients: a new concept for corneal transplantation surgery. Arch Ophthalmol. 2007 Apr;125(4):552-4. 2. Vajpayee RB, Vasudendra N, Tityal J et al. Automated lamellar therapeutic keratoplasty (ALTK) in the treatment of anterior to mid-stromal corneal pathologies. Acta Ophthalmol Scand. 2006: 84:771-773. 3. Watson SL, Ramsay A, Dart JKG, et al. Comparison of deep lamellar and penetrating keratoplasty in patients with keratoconus. Ophthalmology. 2004;111:1676-1682. 4. Panda A, Bageshwar LMS, Ray M, et al. Deep lamellar keratoplasty versus penetrating keratoplasty for corneal lesions. Cornea 1999;18:172-175. 5. Kirkness C, Ficker L, Steele AD, et al. The success of penetrating keratoplasty for keratoconus. Eye. 1990;4:673-688. 6. Buzard KA, Fundingsland BR. Corneal transplant for keratoconus results in early and late disease. J Cataract Refract Surg. 1997;23:398-406.
: Vajpayee RB, Vasudendra N, Tityal J et al. Automated lamellar therapeutic keratoplasty (ALTK) in the treatment of anterior to mid-stromal corneal pathologies. Acta Ophthalmol Scand. 2006: 84: Watson SL, Ramsay A, Dart JKG, et al. Comparison of deep lamellar and penetrating keratoplasty in patients with keratoconus. Ophthalmology. 2004;111: Panda A, Bageshwar LMS, Ray M, et al. Deep lamellar keratoplasty versus penetrating keratoplasty for corneal lesions. Cornea 1999;18: Kirkness C, Ficker L, Steele AD, et al. The success of penetrating keratoplasty for keratoconus. Eye. 1990;4: Buzard KA, Fundingsland BR. Corneal transplant for keratoconus results in early and late disease. J Cataract Refract Surg. 1997;23:")
10
Discussion In the subset of 5 eyes with >12months follow-up (mean 19 months): – BCVA improves (p = 0.19) – UCVA improves (p = 0.06) The continuing improvement of BCVA and UCVA over time may suggest corneal remodeling
: – BCVA improves (p = 0.19) – UCVA improves (p = 0.06) The continuing improvement of BCVA and UCVA over time may suggest corneal remodeling")
11
Discussion Whilst using donor tissue of less stringent quality than for PK, donor corneas previously discarded due to low endothelial cell count but clear good stroma can now be used, maximizing the use of the donor cornea The mean postoperative pachymetry was 593 microns; a thicker postoperative cornea allows additional secondary corneal refractive procedures to be done to enhance visual outcomes

12
Conclusions HALK is a novel procedure that forms another option in the armamentarium for the treatment of anterior stromal diseases Early results are promising for a heterogenous group of corneal pathologies The main advantages of HALK are: 1. The uniform removal of anterior stromal pathology with an irregular anterior corneal surface from the recipient 2. The ability to customize the size and thickness of the donor grafts resulting in optimal optical and postoperative outcomes

Similar presentations






 Habeeb Ahmad, MD Martin Heur,>")



 Thanh T. Nguyen, OD (Delta Eye.>")









