Download presentation
Presentation is loading. Please wait.

1
Renal Transplantation for HIV/HCV Co-infected Patients Solid Organ Transplantation and People With HIV: Ethics and Policy Conference David Oldach & Robert Redfield Institute of Human Virology, U of MD

2
Our Questions: l Are the inclusion/exclusion criteria adequate to protect our subjects from progressive liver disease? R (Currently, cirrhosis is our study-wide exclusion criterion) l Given the poor efficacy and side effect profile of current therapies, should RX decisions continue to be left to the patient and their primary care provider?
 l Given the poor efficacy and side effect profile of current therapies, should RX decisions continue to be left to the patient and their primary care provider .")
3
Relevant Background Information l Impact of HIV on HCV-attributed disease l HIV & HCV coinfection in Baltimore (Evelyn Jordan center, institute of human virology)
")
4
Eyster ME, et al, Blood 1994;84:1022-23 Bonacini M, Puoti M, Arch Intern Med 2000;160(22): 3365-73. HIV Influence on HCV Infection l Increased HCV viral load as immune deficiency progressesn l Acceleration of natural history of HCV (cirrhosis in 33% vs 11%) l Increased risk of liver failure (40% vs 6.8%) l Increased perinatal transmission of HCV
 l Increased risk of liver failure (40% vs 6.8%) l Increased perinatal transmission of HCV.")
5
HCV-HIV Co-Infection in Baltimore l Among IVDA population, HCV transmission to 90%+ within first year if needle sharing… l Prevalence of HCV co-infection at EJC (Institute of Human Virology HIV clinic) approximately 60%…. l Preliminary results of liver biopsies done to screen for presence of significant liver disease…. ---Biopsies NOT PERFORMED if--- R frank cirrhosis present R HCV RNA negative R treatment not desired, or not reasonable

6
Liver Histology in HIV/HCV Coinfected Patients l Over 36 months, approximately 75 liver biopsies performed at IHV/U of MD for treatment evaluation and clinical staging in HIV/HCV co-infected patients. l Biopsies scored using both the Knodell and modified Ishak systems l ALT, CD4, HIV and HCV viral load data, and alcohol consumption histories reviewed for each patient.

7
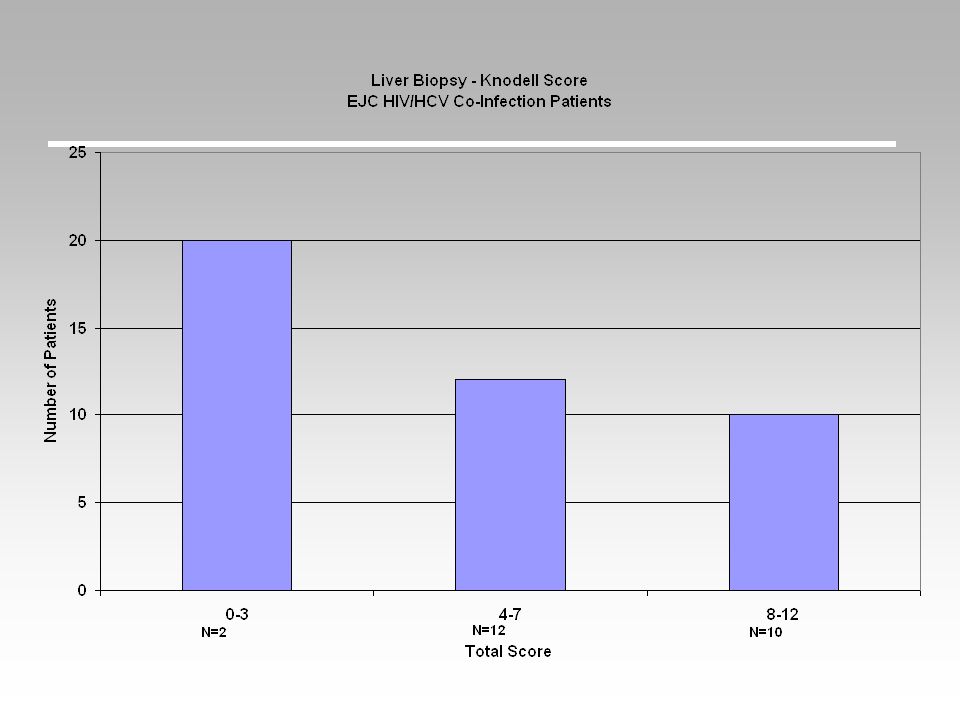
Knodell Scoring system for liver bx: l Four components: Peri-portal piecemeal necrosis (0-10) Intralobular degeneration and necrosis (0-4) Portal inflammation (0-4) Liver Bx Score for fibrosis ( 0-4) l Composite Scores (0-22)
 Intralobular degeneration and necrosis (0-4) Portal inflammation (0-4) Liver Bx Score for fibrosis ( 0-4) l Composite Scores (0-22)")
9
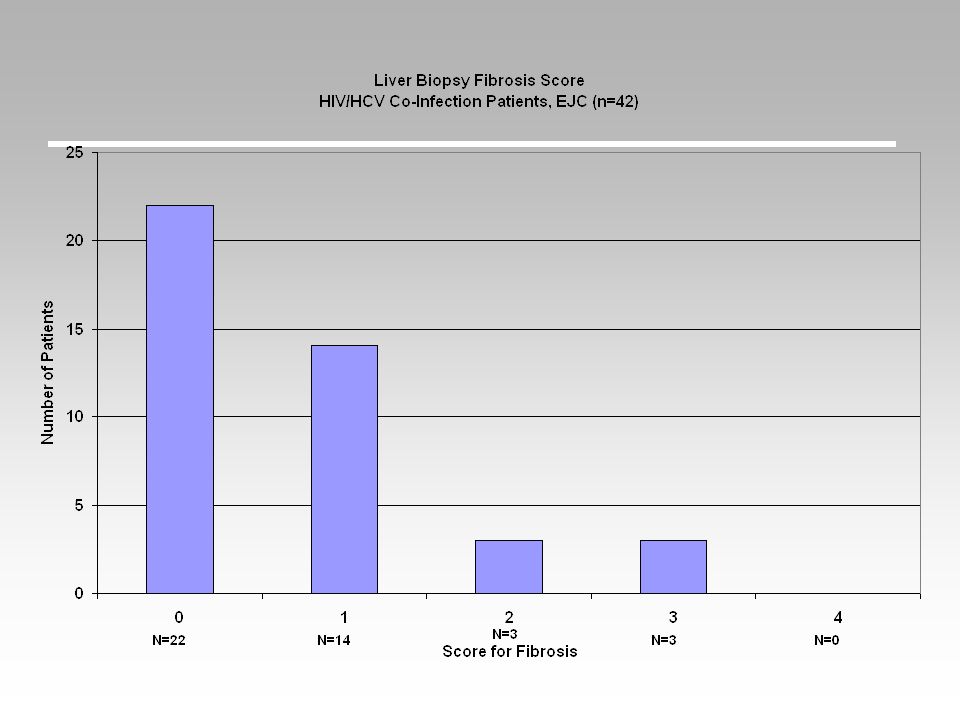
Liver Fibrosis Scores: Ishak N=50 l Grade-0 (no fibrosis)22 (44%) l Grade-1 (portal fibrosis, some)16 (32%) l Grade-2 (portal fibrosis, most) 4 (8%) l Grade-3 (occasional P-P bridging ) 1 (2%) l Grade-4 (marked P-P bridging) 2 (4%) l Grade-5 (incomplete cirrhosis) 3 (6%) l Grade-6 (micronodular cirrhosis) 2 (4%)
22 (44%) l Grade-1 (portal fibrosis, some)16 (32%) l Grade-2 (portal fibrosis, most) 4 (8%) l Grade-3 (occasional P-P bridging ) 1 (2%) l Grade-4 (marked P-P bridging) 2 (4%) l Grade-5 (incomplete cirrhosis) 3 (6%) l Grade-6 (micronodular cirrhosis) 2 (4%)")
14
Summary l Data are preliminary, and are not from HIV/HCV/ESRD population: however l At least 44% of patients studied to date have no evidence of HCV related hepatic fibrosis, the single best predictor of later development of significant HCV related liver disease. l The prognostic significance of Grade-1 fibrosis in these co-infected patients (an additional 32%) remains uncertain.
 remains uncertain..")
15
Significance of Excluding HCV+ Patients From Consideration: If HCV prevalence among HIV/ESRD patients in our population mirrors that in the general HIV population in this urban setting, up to 60% of candidates would be denied therapy…. Among that group, more than 1/3 may have liver histology and ALT profiles that do not warrant a summary exclusion from consideration…. If this patient population (HIV/HCV/ESRD patients) are excluded from consideration, we will most certainly have to return to the question at a later date….
 are excluded from consideration, we will most certainly have to return to the question at a later date…..")
16
Case Presentation for Discussion l 58 y.o. male l HIV (dx, 1986, RF=MSM) R Rx- AZT, 3TC, Indinavir R CD4- 560 (nadir never <200) R HIV VL- 18 months) l ESRD (uncertain etiology)) R Hemodialysis x 4 years l HCV (RF= above, +(transfusions 1973, 1981, 1986) R HCV VL- >1,000,000 RNA copies/ml
 R Rx- AZT, 3TC, Indinavir R CD (nadir never <200) R HIV VL- 18 months) l ESRD (uncertain etiology)) R Hemodialysis x 4 years l HCV (RF= above, +(transfusions 1973, 1981, 1986) R HCV VL- >1,000,000 RNA copies/ml.")
17
Case Presentation for Discussion l Liver biopsy R “chronic HCV with minimal inflammatory activity and no significant fibrosis ” R ISHAK Periportal Necrosis: 1 (0-4) Confluent necrosis: 0 (0-4) Apoptosis: 0 (0-4) Portal inflammation: 1 (0-4) Fibrosis: 0 (0-6)
 Confluent necrosis: 0 (0-4) Apoptosis: 0 (0-4) Portal inflammation: 1 (0-4) Fibrosis: 0 (0-6)")
18
First, Do No Harm (Is withholding tx harmful?) l HCV + ESRD patients (without HIV infection) have higher survival post renal transplant than HCV+ ESRD patients remaining on dialysis therapy…. l (the same is true for patients with ESRD without HIV or HCV infection) l It is unknown whether the same survival benefit can be obtained in HIV/HCV/ESRD patients…..
 l It is unknown whether the same survival benefit can be obtained in HIV/HCV/ESRD patients…...")
19
First, Do No Harm (Is offering tx harmful?) l Significant HCV related disease is more common (occurs earlier, in a higher percentage of patients) in HIV/HCV co-infected patients… l This individual, an HCV ‘carrier’, has no evidence of HCV related disease, despite HIV infection and a demonstrated high HCV viral load… l Would TX-related immunosuppression alter this dynamic? Will accelerated HCV related disease ensue?

20
Back to Question 1: l Are the inclusion/exclusion criteria adequate to protect our subjects from progressive liver disease?

21
Consider: l In general: limit renal transplantation only to those individuals with ‘relatively benign’ histology: i.e., Fibrosis scores of 0, and perhaps stage 1. l Consider pre-transplant HCV treatment for all patients, and require successful treatment for any patient with fibrosis on biopsy (stage 1 or higher). l Consider on case-by-case basis offering renal transplantation to individuals with prior HCV, successfully treated, if with higher fibrosis scores.
. l Consider on case-by-case basis offering renal transplantation to individuals with prior HCV, successfully treated, if with higher fibrosis scores..")
22
Back to Question 2: l Given the poor efficacy and side effect profile of current therapies, should RX decisions continue to be left to the patient and their primary care provider? Until better data are available regarding outcomes of HCV-rx in HIV/HCV/ESRD, we do not believe that we can mandate therapy for inclusion in the transplantation study. However, we believe that most HIV/HCV/ESRD patients should be offered IFN or PEG-IFN rx prior to transplantation. We should approach this problem in the same multi-center study context that we are now proposing for transplantation itself.

Similar presentations










 University of Toronto January 2013.>")









 Act Research Criteria: follow-up discussion Advisory Committee on Organ Transplantation April 13, 2015.>")
