Download presentation
Presentation is loading. Please wait.

1
OVARIAN CANCER New NICE guidelines and the research behind them Journal Club 20/5/11 Natalie Brown and Matthew Parkes

2
Content Summary of NICE guidelines Summary of NICE guidelines Critical appraisal of paper Critical appraisal of paper –Anderson M, Goff B, Lowe K et al. Use of symptom index, CA125 and HE4 to predict ovarian cancer. Gynecol Oncol 2010 March 116(3): 378. Discussion Discussion
: 378. Discussion Discussion.")
3
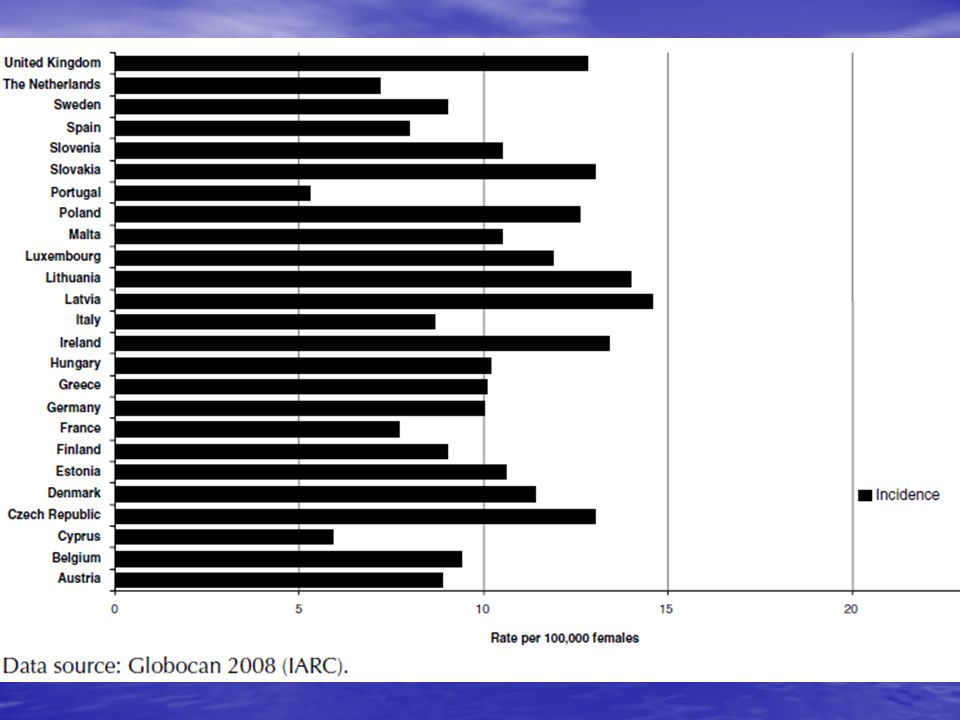
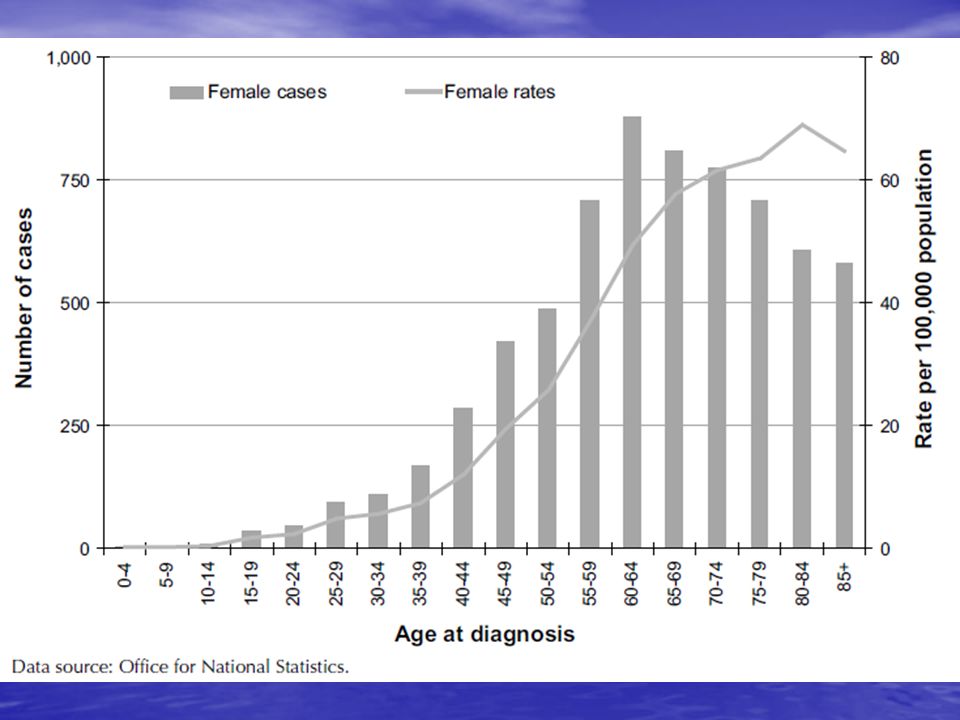
NICE guidelines: Ovarian Cancer The recognition and initial management of ovarian cancer – published April 2011 The recognition and initial management of ovarian cancer – published April 2011 Guidelines produced to focus on areas of uncertainty and when wide variation in clinical practice Guidelines produced to focus on areas of uncertainty and when wide variation in clinical practice Statistics Statistics –5th most common cancer in women (1 in 20 cases of cancer) and rising –Leading cause of death from gynaecological cancer (4,300 women die from ovarian cancer each year in the UK) –Overall 5 year survival 35% –Approximately 6,700 new cases of ovarian cancer were diagnosed every year in United Kingdom between 2004 and 2007
 and rising –Leading cause of death from gynaecological cancer (4,300 women die from ovarian cancer each year in the UK) –Overall 5 year survival 35% –Approximately 6,700 new cases of ovarian cancer were diagnosed every year in United Kingdom between 2004 and 2007")
8
Clinical question: What are the symptoms and signs of ovarian cancer?

9
Recognition in primary care : when to measure CA-125 Symptoms present particularly >12 times per month (especially if >50yo) Symptoms present particularly >12 times per month (especially if >50yo) –Persistent abdominal distension (‘bloating’) –Early satiety and/or loss of appetite –Pelvic or abdominal pain –Increased urinary urgency and/or frequency Alternatively, suspect in a woman over 50 who has developed ‘IBS’ symptoms in the last year Alternatively, suspect in a woman over 50 who has developed ‘IBS’ symptoms in the last year Also measure if experiencing weight loss, change in bowel habit or fatigue and ovarian cancer is suspected Also measure if experiencing weight loss, change in bowel habit or fatigue and ovarian cancer is suspected
 Symptoms present particularly >12 times per month (especially if >50yo) –Persistent abdominal distension (‘bloating’) –Early satiety and/or loss of appetite –Pelvic or abdominal pain –Increased urinary urgency and/or frequency Alternatively, suspect in a woman over 50 who has developed ‘IBS’ symptoms in the last year Alternatively, suspect in a woman over 50 who has developed ‘IBS’ symptoms in the last year Also measure if experiencing weight loss, change in bowel habit or fatigue and ovarian cancer is suspected Also measure if experiencing weight loss, change in bowel habit or fatigue and ovarian cancer is suspected")
10
When to avoid CA-125 in primary care If a woman has ascites and/or an abdominal or pelvic mass on clinical examination that is ‘not obviously due to uterine fibroids’ If a woman has ascites and/or an abdominal or pelvic mass on clinical examination that is ‘not obviously due to uterine fibroids’ Refer urgently (2 week referral) to secondary care Refer urgently (2 week referral) to secondary care
 to secondary care Refer urgently (2 week referral) to secondary care")
11
Investigation after CA-125 results in primary care If CA-125 > 35, arrange USS abdomen and pelvis If CA-125 > 35, arrange USS abdomen and pelvis –If USS suggestive of ovarian cancer, refer urgently (2ww) –If normal USS consider other causes If CA-125<35, consider other causes If CA-125<35, consider other causes
 –If normal USS consider other causes If CA-125<35, consider other causes If CA-125<35, consider other causes")
13
Establishing the diagnosis in secondary care Need to have USS or CA-125 if not already done Need to have USS or CA-125 if not already done If under 40 years old, measure beta-hCG and AFP to identify those who may not have epithelial ovarian cancer If under 40 years old, measure beta-hCG and AFP to identify those who may not have epithelial ovarian cancer Next calculate RMI score and refer to MDT if score >250 Next calculate RMI score and refer to MDT if score >250

14
Risk of malignancy index (RMI) RMI = score based on combination of USS findings, menopausal status and CA-125 level RMI = score based on combination of USS findings, menopausal status and CA-125 level USS score; 1 point if one of the following present, 3 points if 2-5 of the following present USS score; 1 point if one of the following present, 3 points if 2-5 of the following present –Multilocular cysts –Solid areas –Metastases –Ascites –Bilateral lesions
 RMI = score based on combination of USS findings, menopausal status and CA-125 level RMI = score based on combination of USS findings, menopausal status and CA-125 level USS score; 1 point if one of the following present, 3 points if 2-5 of the following present USS score; 1 point if one of the following present, 3 points if 2-5 of the following present –Multilocular cysts –Solid areas –Metastases –Ascites –Bilateral lesions")
15
RMI continued Menopausal status Menopausal status –1 point if pre-menopausal –3 points if post-menopausal CA-125 CA-125 –Use the value itself Eg a post menopausal lady with ascites and solid areas on USS, and CA-125 of 50 has an RMI of 3 x 3 x 50 = 300 Eg a post menopausal lady with ascites and solid areas on USS, and CA-125 of 50 has an RMI of 3 x 3 x 50 = 300 If RMI is 250 or greater, must be referred to specialist MDT If RMI is 250 or greater, must be referred to specialist MDT

16
Further investigation in secondary care If overall picture suggestive of ovarian cancer, needs CT pelvis, abdomen +/- thorax to assist with staging If overall picture suggestive of ovarian cancer, needs CT pelvis, abdomen +/- thorax to assist with staging MRI not routinely advised MRI not routinely advised Tissue diagnosis – generally recommend if contemplating chemotherapy Tissue diagnosis – generally recommend if contemplating chemotherapy –Percutaneous image guided biopsy –Laparoscopic biopsy

17
Summary of clinical management Stage I Stage I –Oophorectomy –Retroperitoneal lymph node assessment –1a and 1b – no chemotherapy –1c and above – adjuvant chemotherapy Stage II-IV Stage II-IV –Surgical objective = complete removal of all macroscopic disease –Intraperitoneal chemotherapy only used in Trials at present

18
Summary of holistic management Fertility Fertility Sexuality Sexuality Genetics Genetics Physiotherapy Physiotherapy Self-help strategies Self-help strategies Counselling Counselling Support groups Support groups

19
Further research recommendations Further research should be undertaken on the relationship between the duration and frequency of symptoms in women with ovarian cancer before diagnosis, the stage of disease at diagnosis and subsequent survival. Further research should be undertaken on the relationship between the duration and frequency of symptoms in women with ovarian cancer before diagnosis, the stage of disease at diagnosis and subsequent survival. Large multicentre case–control studies should be conducted to compare the accuracy of CT versus MRI for staging in women with ovarian cancer. Large multicentre case–control studies should be conducted to compare the accuracy of CT versus MRI for staging in women with ovarian cancer.

20
Critical Appraisal of journal article Anderson M, Goff B, Lowe K et al. Use of symptom index, CA125 and HE4 to predict ovarian cancer. Gynecol Oncol 2010 March 116(3): 378. Anderson M, Goff B, Lowe K et al. Use of symptom index, CA125 and HE4 to predict ovarian cancer. Gynecol Oncol 2010 March 116(3): 378. Using ‘CASP’ framework via BWH Trust library homepage Using ‘CASP’ framework via BWH Trust library homepage
: 378. Anderson M, Goff B, Lowe K et al. Use of symptom index, CA125 and HE4 to predict ovarian cancer. Gynecol Oncol 2010 March 116(3): 378. Using ‘CASP’ framework via BWH Trust library homepage Using ‘CASP’ framework via BWH Trust library homepage.")
21
Did the study address a clearly defined issue? To evaluate to use of symptom index with serum HE4 or Ca-125 alone and in combination to predict ovarian cancer To evaluate to use of symptom index with serum HE4 or Ca-125 alone and in combination to predict ovarian cancer

22
Did the authors use an appropriate method to answer their question? Prospective case-control study Prospective case-control study –74 women with ovarian cancer –137 ‘healthy’ women as controls

23
Were the cases recruited in an acceptable way? Cases were recruited from a group that had positive imaging suggesting ovarian cancer and were surveyed prior to surgery and before receiving a definitive diagnosis of ovarian cancer Cases were recruited from a group that had positive imaging suggesting ovarian cancer and were surveyed prior to surgery and before receiving a definitive diagnosis of ovarian cancer

24
Were the controls recruited in an acceptable way? All controls have family histories consistent with inherited susceptibility for ovarian cancer All controls have family histories consistent with inherited susceptibility for ovarian cancer

25
Was exposure accurately measured to avoid bias?

26
What confounding factors have the authors accounted for? Control group selection bias and the ability to record and recall symptoms more specific to ovarian cancer Control group selection bias and the ability to record and recall symptoms more specific to ovarian cancer Recall bias of patients awaiting surgery and ability to remember recent symptoms than a high risk control group Recall bias of patients awaiting surgery and ability to remember recent symptoms than a high risk control group Study does not have detailed information for imaging results Study does not have detailed information for imaging results The study did not look at case notes to see if symptoms had been clinically reported – only took results from their own survey The study did not look at case notes to see if symptoms had been clinically reported – only took results from their own survey

27
What are the results? As a single marker CA-125 had the highest overall sensitivity 81.1% and specificity of 95% As a single marker CA-125 had the highest overall sensitivity 81.1% and specificity of 95% HE4 had the highest sensitivity in high risk cases, overall sensitivity 77% and specificity 95% HE4 had the highest sensitivity in high risk cases, overall sensitivity 77% and specificity 95% Symptom index alone showed sensitivity of 63.5% and specificity of 88.3% Symptom index alone showed sensitivity of 63.5% and specificity of 88.3% Any 2 of 3 above positive sensitivity 83.8% and specificity of 98.5% Any 2 of 3 above positive sensitivity 83.8% and specificity of 98.5%

28
How precise are the results? Wide confidence intervals for results Wide confidence intervals for results

29
Do you believe the results? Unable to comment on quality and appropriateness of ‘survey’ Unable to comment on quality and appropriateness of ‘survey’ Measuring of serum markers appropriate Measuring of serum markers appropriate

30
Can the results be applied to the local population? USA study USA study Symptom reporting different across Atlantic? Symptom reporting different across Atlantic? Tumour markers ? Universal across populations Tumour markers ? Universal across populations

31
Do the results fit with other available evidence? HE4 - - Consistent evidence across studies suggesting HE4 better than Ca-125 - - Also suggests that the combination of HE4 and CA125 is more specific, but less sensitive than either marker in isolation.

Similar presentations



Fabian Lee, Foundation Year 2. (2) Gbolahan.>")

















