Download presentation
Presentation is loading. Please wait.

1
Colorectal carcinoma Dr.Mohammadzadeh

2
Epidemiology (Risk Factors)
Aging Hereditary Risk Factors Environmental and Dietary Factors Inflammatory Bowel Disease Other Risk Factors

3
Genetic Defects

4
Polyps Any projection from the surface of the intestinal mucosa regardless of its histologic nature adenoma–carcinoma sequence : The majority of colorectal carcinomas evolve from adenomatous polyps

5
Types of Colorectal polyps
Neoplastic (tubular adenoma, villous adenoma, tubulovillous adenomas) Hamartomatous (juvenile, Peutz-Jeghers, Cronkite-Canada) Inflammatory (pseudopolyp, benign lymphoid polyp) Hyperplastic
 Hamartomatous (juvenile, Peutz-Jeghers, Cronkite-Canada) Inflammatory (pseudopolyp, benign lymphoid polyp) Hyperplastic.")
6
Neoplastic Polyps Adenomatous polyps are common, occurring in up to 25% of the population older than 50 years of age The risk of malignant degeneration is related to both the size and type of polyp. Tubular adenomas are associated with malignancy in only 5% of cases, whereas villous adenomas may harbor cancer in up to 40%. Tubulovillous adenomas are at intermediate risk (22%).
.")
7
Polyps may be pedunculated or sessile.
Most pedunculated polyps are amenable to colonoscopic snare excision. Removal of sessile polyps often is more challenging Complications of polypectomy include perforation and bleeding

8
Hamartomatous Polyps (Juvenile Polyps)
In contrast to adenomatous polyps, hamartomatous polyps (juvenile polyps) usually are not premalignant. Bleeding is a common symptom and intussusception and/or obstruction may occur.
 usually are not premalignant. Bleeding is a common symptom and intussusception and/or obstruction may occur.")
9
Juvenile Polyposis Familial juvenile polyposis Peutz-Jeghers syndrome
Cronkite-Canada syndrome Cowden syndrome

10
Inflammatory Polyps (Pseudopolyps)
Inflammatory polyps occur most commonly in the context of inflammatory bowel disease May also occur after amebic colitis, ischemic colitis, and schistosomal colitis. These lesions are not premalignant

11
Hyperplastic Polyps Hyperplastic polyps are extremely common in the colon. These polyps usually are small (<5 mm) and show histologic characteristics of hyperplasia without any dysplasia. They are not considered premalignant Hyperplastic polyposis
 and show histologic characteristics of hyperplasia without any dysplasia. They are not considered premalignant. Hyperplastic polyposis.")
12
Inherited Colorectal Carcinoma
Familial Adenomatous Polyposis Attenuated FAP Hereditary Nonpolyposis Colon Cancer (Lynch Syndrome) Familial Colorectal Cancer
 Familial Colorectal Cancer.")
13
Familial Adenomatous Polyposis
autosomal dominant about 1% of all colorectal adenocarcinomas The genetic abnormality in FAP is a mutation in the APC gene, located on chromosome 5q. Once the diagnosis of FAP has been made and polyps are developing, treatment is surgical. Four factors affect the choice of operation: age of the patient; presence and severity of symptoms; extent of rectal polyposis; and presence and location of cancer or desmoid tumors.

14
Attenuated FAP Patients present later in life with fewer polyps (usually 10 to 100) dominantly located in the right colon Colorectal carcinoma develops in more than 50% of these patients, but occurs later (average age 55 years).
.")
15
Lynch Syndrome(HNPCC)
HNPCC (or Lynch syndrome) is more common than FAP, but is still extremely rare (1 to 3%). Approximately 70% of affected individuals will develop colorectal cancer (average age: 40 to 45 years). Cancers appear in the proximal colon more often than in sporadic colorectal cancer and have a better prognosis regardless of stage.
 is more common than FAP, but is still extremely rare (1 to 3%). Approximately 70% of affected individuals will develop colorectal cancer (average age: 40 to 45 years). Cancers appear in the proximal colon more often than in sporadic colorectal cancer and have a better prognosis regardless of stage.")
16
Familial Colorectal Cancer
Nonsyndromic familial colorectal cancer accounts for 10 to 15% of patients with colorectal cancer The lifetime risk of colorectal cancer in a patient with no family history of this disease (average-risk population) is approximately 6%, but rises to 12% if one first-degree relative is affected and to 35% if two first-degree relatives are affected.
 is approximately 6%, but rises to 12% if one first-degree relative is affected and to 35% if two first-degree relatives are affected.")
19
Routes of Spread

20
Clinical Presentation
Nonspecific and generally develop when the cancer is locally advanced. The classic first symptoms are a change in bowel habits and rectal bleeding. Abdominal pain, bloating, and other signs of obstruction typically occur with larger tumors . Because of the caliber of the bowel and the consistency of the stool, left-sided tumors are more likely to cause obstruction than are right-sided tumors. Rectal tumors may cause bleeding, tenesmus, and pain. unexplained anemia, weight loss, or poor appetite

24
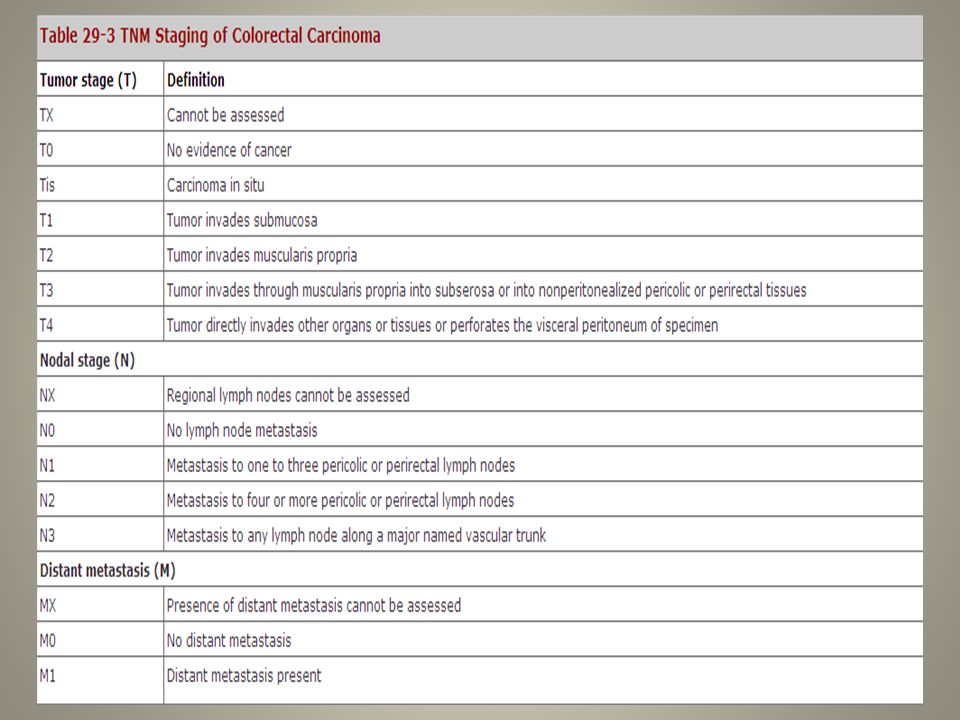
Stage-Specific Therapy
Stage 0 (Tis, N0, M0) : these polyps should be excised completely and pathologic margins should be free of dysplasia. In cases where the polyp cannot be removed entirely, a segmental resection is recommended
 : these polyps should be excised completely and pathologic margins should be free of dysplasia. In cases where the polyp cannot be removed entirely, a segmental resection is recommended.")
25
Stage I: The Malignant Polyp (T1, N0, M0)
Invasive carcinoma in the head of a pedunculated polyp with no stalk involvement carries a low risk of metastasis (<1%) and may be completely resected endoscopically. However, lymphovascular invasion, poorly differentiated histology, or tumor within 1 mm of the resection margin greatly increases the risk of local recurrence and metastatic spread. Segmental colectomy is then indicated. Invasive carcinoma arising in a sessile polyp extends into the submucosa and is usually best treated with segmental colectomy
 and may be completely resected endoscopically. However, lymphovascular invasion, poorly differentiated histology, or tumor within 1 mm of the resection margin greatly increases the risk of local recurrence and metastatic spread. Segmental colectomy is then indicated. Invasive carcinoma arising in a sessile polyp extends into the submucosa and is usually best treated with segmental colectomy.")
27
Stages I and II: Localized Colon Carcinoma (T1–3, N0, M0)
The majority of patients with stages I and II colon cancer will be cured with surgical resection Adjuvant chemotherapy does not improve survival in these patients Adjuvant chemotherapy has been suggested for selected patients with stage II disease (young patients, tumors with "high-risk" histologic findings)
")
28
Stage III: Lymph Node Metastasis (Tany, N1, M0)
Patients with lymph node involvement are at significant risk for both local and distant recurrence, and adjuvant chemotherapy has been recommended routinely in these patients

29
Stage IV: Distant Metastasis (Tany, Nany, M1)
Survival is extremely limited in stage IV colon carcinoma Of patients with systemic disease, approximately 15% will have metastases limited to the liver. Of these, 20% are potentially resectable for cure Metastasis of the lung, occurring in approximately 20% of patients and 1-2% will be resectable

Similar presentations




















>")


