Download presentation
Presentation is loading. Please wait.

2
sensory event of both PNS and CNS emotional component cognitive component

3
acute pain chronic pain

4
pain can be modulated, enhanced or diminished by both central and peripheral mechanisms ◦ peripheral aspect – non steroidal antiinflammatory drugs ◦ central aspects – opioid analgesics Roxicet, Tylox (acetaminophen and oxycodone) Percocet – (oxycodone with paracetamol)
 Percocet – (oxycodone with paracetamol)")
5
opium extracted from opium poppy ◦ used for thousands of years to produce euphoria, analgesia, sleep and relief from diarrhea and cough ancient times – primarily for constipating effects Homer, Hippocrates, et ◦ sleep producing effects

6
Early 1800’s – morphine isolated from opium as its active ingredient ◦ treating severe pain 1856- invention of the hypodermic syringe ◦ Civil War – “soldiers disease” 1910 – concern about dangers of opioids and dependence 1914- Harrison Narcotic Act ◦ use of most opioids strictly controlled

7
1970 – ◦ established current schedules of drugs

12
opium – juice or sap from the poppy opiate – drug extracted from the sap morphine codeine

13
opioid – any exogenous drug (natural, semisynthetic or synthetic) that binds to an opiate receptor and produces agonist or morphine-like effects endorphin – endogenous substance that exhibits pharmacological properties like morphine 3 familes of endogenous opioid peptides
 that binds to an opiate receptor and produces agonist or morphine-like effects endorphin – endogenous substance that exhibits pharmacological properties like morphine 3 familes of endogenous opioid peptides")
14
enkephalins dynorphins beta endorphins

15
opioids occur in nature in 2 places the juice of the poppy in our bodies…… all other opioids are either prepared from morphine (semisynthetic opioids like heroin) or synthesized from other precursors (synthetic opioids such as fentanyl)
 or synthesized from other precursors (synthetic opioids such as fentanyl)")
16
analgesic potency of the agonist correlates with affinity of agonist for opioid receptor at least 3 types of opioid receptors ◦ mu- ◦ kappa ◦ delta

17
some areas have all 3 types of opioid receptors ◦ (spinal cord) some have predominantly one type of receptor
 some have predominantly one type of receptor")
18
brain, sc, and periphery morphine – mu agonist ◦ exerts effects in thalamus and striatum ◦ brain stem (affects respiration) ◦ spinal cord (analgesic effects) PAG, brain stem, nucleus accumbens,
 ◦ spinal cord (analgesic effects) PAG, brain stem, nucleus accumbens,")
19
may modulate mu receptors

20
minor analgesic effects; pinpoint pupils modest analgesia no addiction potential dysphoria

21
pure agonists – mu agonists ◦ produces analgesia, reward, respiratory depression

22
morphine codeine heroin meperidine (Demerol) methadone (Dolophine) oxymorphone (Numorphan) hydromorphone (Dilaudid) fentanyl (Sublimaze) oxycodone
 methadone (Dolophine) oxymorphone (Numorphan) hydromorphone (Dilaudid) fentanyl (Sublimaze) oxycodone")
23
produces agonist effects at one receptor and antagonist at another clinically useful mixed drugs – kappa agonist and weak mu antagonist useful for moderate pain not good if someone is dependent on opiates

24
binds to opioid receptors but has low intrinsic activity (low efficacy) can produce analgesia – but ceiling lower than pure agonist buprenorphine (Suboxone) binds to all 3 receptors
 can produce analgesia – but ceiling lower than pure agonist buprenorphine (Suboxone) binds to all 3 receptors")
25
block opiate receptors naloxone, naltrexone depot injections of naltrexone

26
pure agonist more potent and represents about 10% of crude sap codeine much less potent

27
usually administered via injection although rectal or oral is possible intranasal system under development absorption from GI slow and incomplete compared to other routes morphine crosses bbb fairly slowly (more H20 soluble than lipid soluble) ◦ heroin, fentanyl – cross bbb much more quickly
 ◦ heroin, fentanyl – cross bbb much more quickly")
28
liver metabolizes morphine; one metabolite is actually 10 – 20X more potent than morphine for analgesia

29
analgesia euphoria respiratory depression cough suppression pupillary constriction nausea and vomiting GI symptoms endocrine symptoms immune system effects histamine release

30
codeine – ◦ one of the most commonly prescribed opioid ◦ usually combined with aspirin or acetaminophen for relief of mild to moderate pain

31
heroin ◦ (diacetylmorphine) ◦ 3X more potent than morphine ◦ produced by a slight modification of morphine structure ◦ increased lipid solubility ◦ metabolized to monoacetylmorphine and morphine ◦ legally available in Great Britain
 ◦ 3X more potent than morphine ◦ produced by a slight modification of morphine structure ◦ increased lipid solubility ◦ metabolized to monoacetylmorphine and morphine ◦ legally available in Great Britain")
32
(Percodan, OxyContin)- semisynthetic opioid percodan short-acting; oxycontin – long- acting current abuse high;
- semisynthetic opioid percodan short-acting; oxycontin – long- acting current abuse high;")
33
hydromorphone (Dilaudid), oxymorphone (Numorphan) both structurally related to morphine as effective but 6 – 10X more potent meperidine (Demerol) ◦ structurally different from morphine – different side effect profile
, oxymorphone (Numorphan) both structurally related to morphine as effective but 6 – 10X more potent meperidine (Demerol) ◦ structurally different from morphine – different side effect profile")
34
rate at which tolerance develops can vary widely; pattern of use plays a role cross-tolerance physical dependence can develop

35
many of the effects observed are opposite of opiate

36
Opiate withdrawal: ◦ Acute symptoms: restlessness, lacrimation, runny nose, yawning, perspiration, goose flesh ("cold turkey"), restless sleep and dilated pupils during the first 24 hours (onset usually 8 to 12 hours after a reduction in dose or cessation of use)
, restless sleep and dilated pupils during the first 24 hours (onset usually 8 to 12 hours after a reduction in dose or cessation of use)")
37
◦ 5 – 7 days into withdrawal; symptoms can become more severe can be characterized by twitching and spasms of muscles; kicking movements (“kicking the habit”), severe aches in the back, abdomen, and legs; abdominal and muscle cramps; hot and cold flashes; insomnia; nausea, vomiting, and diarrhea; sneezing; fever
, severe aches in the back, abdomen, and legs; abdominal and muscle cramps; hot and cold flashes; insomnia; nausea, vomiting, and diarrhea; sneezing; fever")
38
Jittery, high pitched cry, hyperactive reflexes, restlessness, GI upset, etc. heroin withdrawal occurs within 48-72 hours in 50-80% of infants Methadone withdrawal may be delayed up to 6 days after birth

39
1935 - first federal "narcotics farm" (U.S. Public Health Prison Hospital) opens in Lexington, Kentucky Role of cues
 opens in Lexington, Kentucky Role of cues.")
40
substitution therapy What are the advantages of substitution therapy?

41
methadone – ◦ synthetic mu agonist ◦ 2 primary legitimate users substitution for opiate dependent heroin users long acting analgesic for chronic pain syndromes Physicians who are not in licensed methadone programs cannot prescribe methadone for opioid dependence methadone clinics locations diversion

42
Oral administration – reaches peak levels in ~ 2 hrs; Half life – the amount of time necessary for ½ of the drug to be metabolized in the body; for methadone – very variable but for most people ~ 24-25 hours ◦ When used for treating addiction – 1/day ◦ For pain management – more likely 3 – 4 times/day

43
levo-alpha acetylmethadol approved in mid 1993 for clinical management of opioid dependence longer ½ life not currently available because of possible serious cardiac complications

44
Subutex – advantages – longer ½ life Suboxone- buprenorphine/naloxone advantages of buprenorphine

45
naloxone (Narcan) ◦ treating overdose what happens in opiate dependent individuals? ◦ must be given by injection- short ½ life naltrexone (Trexan, ReVia) ◦ longer duration of action and can be taken orally ◦ downside to naltexone
 ◦ longer duration of action and can be taken orally ◦ downside to naltexone.")
48
How was it discovered--- 1982 – San Francisco Designer Drug that was supposed to mimic heroin Seven heroin addicts at ER All showed signs of severe Parkinsons like Disease Found that the drug had been contaminated with a toxin called MPTP First human cohort of MPTP- induced parkinsonism

49
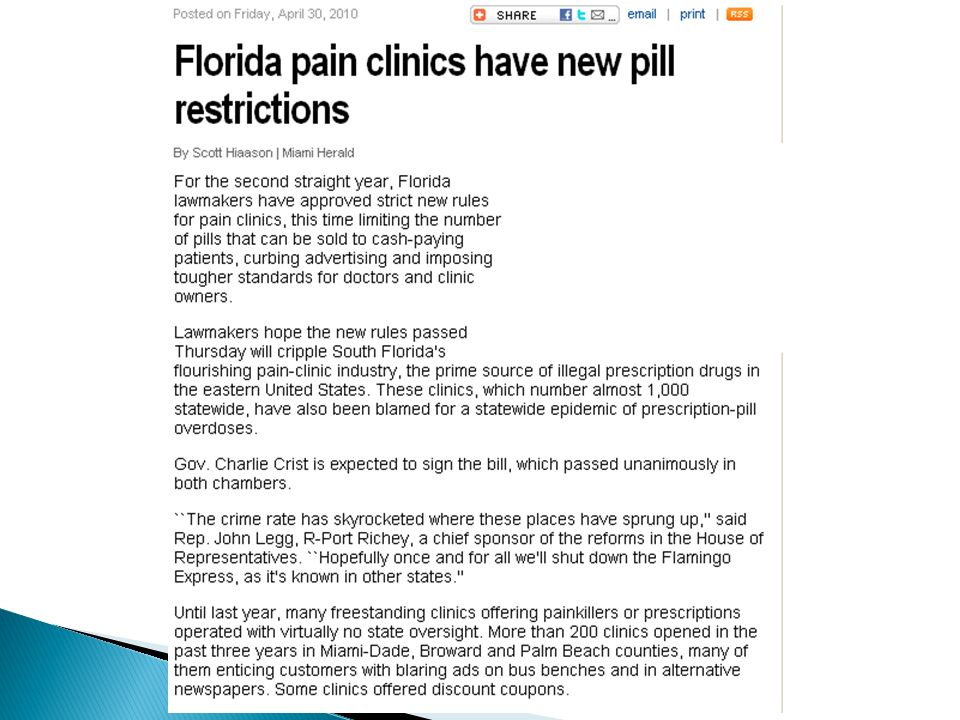
Vanguard ◦ “The Oxycontin Express” ◦ Can be found on Hulu

54
June 2010

55
July 1, 2001, nationwide law in Portugal decriminalized all drugs, including cocaine and heroin ◦ drugs were "decriminalized," not "legalized.” ◦ drug possession for personal use and drug usage itself are still legally prohibited FINES BUT NOT JAIL ◦ trafficking still a criminal offense

Similar presentations

















 Medical University of Sofia, Faculty of Medicine Department of Pharmacology and Toxicology.>")
 Analgesics and Antagonists.>")
![Pharmacology – II [PHL 322] Opioids Analgesics Dr. Mohd Nazam Ansari.](/18/6188558/big_thumb.jpg "Pharmacology – II [PHL 322] Opioids Analgesics Dr. Mohd Nazam Ansari.>")
 Chapter 9>")

 Chapter 9>")