Download presentation
Presentation is loading. Please wait.

1
Adrenal Physiology and Hypofunctioning States
Heidi Chamberlain Shea, MD Endocrine Associates of Dallas

2
Goals of Discussion Review Adrenal Physiology
Identify the clinical features of Adrenal Insufficiency Etiologies of Adrenal Insufficiency Understand testing of adrenal function Treatment of Adrenal Insufficiency

3
Adrenal Development Derived
Neuroectodermal cells (medulla) Mesenchymal cells (cortex) Fetal adrenal is present by 2 months gestation Mostly cortex Glomerulosa and fasiculata are present at birth Reticularis develops during first year of life
 Mesenchymal cells (cortex) Fetal adrenal is present by 2 months gestation. Mostly cortex. Glomerulosa and fasiculata are present at birth. Reticularis develops during first year of life.")
4
Adrenal Anatomy Adult adrenal Located Vascular supply 2-3cm wide
1cm thick 4-6 grams Located Upper pole of kidneys Vascular supply 12 small arteries from aorta

5
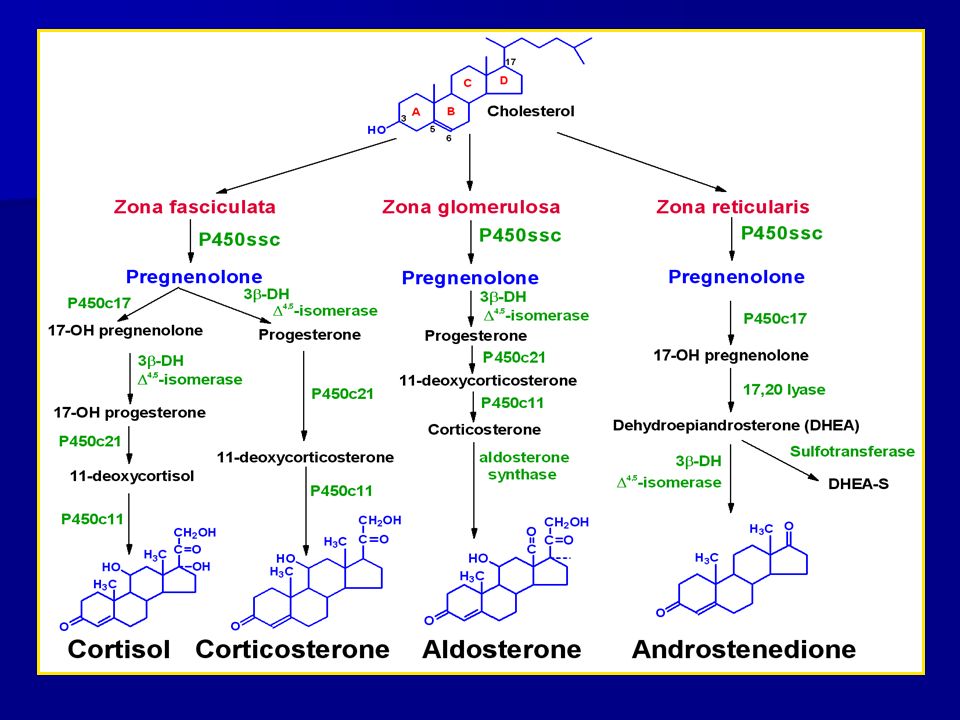
Adrenal Physiology Glomerulosa Fasciulata Reticularis Medulla
15% of cortex Aldosterone Renin-Angiotensin Fasciulata 75% of cortex Cortisol DHEA ACTH Reticularis Androgens and estrogens Medulla Catecholamines

7
Congenital Adrenal Hyperplasia
Most adrenal biosynthetic defects result in Virilized female Normally virilized male Deficiencies Mineralocorticoid Glucocorticoid 21-OH deficiency 11-OH deficiency

8
Congenital Adrenal Hyperplasia
Deficiency of CYP 17 17α- hydroxylase and lyase deficiency Rare cause Diagnosed due to delayed pubertal development 46xx Hypertensive +/- Hypokalemic Primary amenorrhea Absent secondary sex characteristics

9
Congenital Adrenal Hyperplasia
Deficiency of CYP 17 46XY Complete male pseudohermaphroditism Female external genitalia Blind-ended vagina No mullerian structures Testes intra-abdominal Leydig cell hyperplasia Hypertensive +/- Hypokalemic Cortisol sufficient Tolerates general anesthesia and surgery Treatment Steroids to suppress excess Gonadal replacement

11
Congenital Adrenal Hyperplasia
3 β-Hydroxysteroid Dehydrogenase Presents early infancy Adrenal insufficiency Females can be virilized due to DHEA Males Normal genital development Hypospadias Pseudohermaphroditism Can present in puberty Hyperandrogenemia Hirsuitism Oligomenorrhea Treatment Cortisol replacement

12
Congenital Adrenal Hyperplasia
Congenital Lipoid Adrenal Hyperplasia StAR Deficiency Transports cholesterol to inner mitochondrial membrane Rarest form Autosomal recessive All adrenal steroids are deficient Present with adrenal insufficiency Typically fatal infancy Males Female external genitalia

13
Renin and Aldosterone Renin Aldosterone
Enzyme released from the kidneys (macula densa) Activates Angiotensinogen Angiotensin Angiotensin 2 Increased secretion Low blood pressure Low sodium High potassium Upright posture Aldosterone Sodium homeostasis Regulates arterial pressure Regulated Angiotensin 2 Increases Renal sodium retention Renal potassium excretion Low Aldosterone Adrenal insufficiency High renin Hyperkalemia
 Activates Angiotensinogen Angiotensin 1 Angiotensin 2. Increased secretion. Low blood pressure. Low sodium. High potassium. Upright posture. Aldosterone. Sodium homeostasis. Regulates arterial pressure. Regulated. Angiotensin 2. Increases. Renal sodium retention. Renal potassium excretion. Low Aldosterone. Adrenal insufficiency. High renin. Hyperkalemia.")
14
Renin and Aldosterone

15
Mineralocorticoid Deficiency
Hyporeninemic Hypoaldosteronism Impaired renin release 50-70 years Chronic assymptomatic hyperkalemia Mild-moderate renal insufficiency Muscle weakness Cardiac arrhythmias

16
Mineralocorticoid Deficiency
Other diseases SLE Multiple myeloma Renal amyloidosis Cirrhosis Sickle Cell AIDS POEMS Transient with drugs NSAID Cyclosporin A Mitomycin C Cosyntropin 50% of patients with Diabetes Type IV RTA Metabolic acidosis Decreased renal ammoniagenesis Decreased H ion secretion Decreased bicarbonate resorbtion Polyneuropathy, organomegaly, endorinopathy, Mprotein, skin changes- Diabetes, bone lesions, hypogonadism, hepatomegaly, LAD

17
Mineralocorticoid Deficiency Primary Hypoaldosteronism
Aldosterone synthase deficiency (CYP11B2) Autosomal recessive Diagnosed in infancy Recurrent dehydration Failure to thrive Salt wasting Treatment Florinef Acquired Heparin Suppresses aldosterone Increase in renin Healthy person, asymptomatic Critically ill, can be symptomatic
 Autosomal recessive. Diagnosed in infancy. Recurrent dehydration. Failure to thrive. Salt wasting. Treatment. Florinef. Acquired. Heparin. Suppresses aldosterone. Increase in renin. Healthy person, asymptomatic. Critically ill, can be symptomatic.")
18
Mineralocorticoid Deficiency Primary Hypoaldosteronism
Pseudohypoaldosteronism Salt wasting syndrome Infancy Renal tubular insensitivity to mineralocorticoids Autosomal Dominant Resistance to aldosterone at the renal tubule Autosomal Recessive Severe Also affects sweat and salivary glands Colon Features of hypoaldosteronism Hyopnatremia Hyperkalemia Hyper-reninemia Increased aldosterone levels Many kindreds Homozygous mutation in amiloride-sensitive epithelial sodium channel Treatment NaCl K+ binding resins

19
CRH HYPOTHALAMUS HYPOTHALAMIC- PITUITARY PORTAL SYSTEM (-) (-) (+) POSTERIOR PITUITARY ANTERIOR ACTH PITUITARY CORTISOL Adrenal Fasiculata

20
Adrenal Physiology Increase in response to stress ACTH and cortisol
Hypoglycemia Surgery Illness Hypotension Smoking Cold exposure Blunted response Chronic illness ACTH and cortisol Pulsatile secretion Highest in AM at wakening Lowest late afternoon and evening Nadir is 1-2 hrs after the start of sleep Circadian Blind patient Reverts to a hr DHEA and Androstenedione regulated by ACTH

21
Circulation of Cortisol and Adrenal Androgens
Secreted unbound In circulation bind to plasma proteins Unbound is active Cortisol Free (10%) Corticosteroid-binding globulin (CBG) (75%) Albumin Androgens Albumin Testosterone Sex Hormone binding (SHBG)
 Corticosteroid-binding globulin (CBG) (75%) Albumin. Androgens. Albumin. Testosterone. Sex Hormone binding (SHBG)")
22
Cortisol Effects Connective Tissue Bone Calcium metabolism
Inhibit fibroblasts Loss of collagen Thinning of skin Bone Inhibit bone formation Stimulate bone resorption Potentiate actions of PTH Increased resorption Calcium metabolism Decrease intestinal calcium absorption Stimulates renal 1α-hydroxylase Increases 1,25 OH vitamin D synthesis Increased calciuria Increased phosphaturia

23
Cortisol Effects Immunologic Growth Inhibit prostaglandin synthesis
Accelerate development of fetal tissues Lung maturity Inhibit linear growth Decreased growth hormone Erythrocytes Minimal effect Leukocytes Increase PMN by increasing release from bone marrow Decreases lymphocytes, monocytes and eosinophils Immunologic Inhibit prostaglandin synthesis Phospholipase A2 Decreases IL-1 IL-1 stimulates CRH and ACTH Impairs AB production and clearance

24
Cortisol Effects Cardiovascular Renal function Nervous system
Increase CO Increase peripheral vascular tone Hypertension Renal function Mineralocorticoid receptors Na retention Hypokalemia HTN Glucocorticoid receptors Increased GFR Nervous system Enters the brain Euphoria Irritability, depression and emotional lability Hyperkinetic or manic behavior Overt psychosis Increased appetite Impaired memory or concentration Decreased libido Insomnia Decreased REM and increased Stage II sleep

25
Cortisol Effects Metabolism
Glycogen Activates glycogen production\ Deactivates glycogen breakdown Glucose Increase hepatic glucose production Inhibits peripheral tissue utilization of glucose Lipids Activate lipolysis in adipose tissue Redistributes body fat Sparing of the extremities

26
Adrenal Insufficiency
Incidence 6 cases per 1 million adults/year Prevalence cases per 1 million adults More common in females 2.6:1 Diagnosed in the 3-5th decades

27
Adrenal Insufficiency Presentation
Signs and symptoms Rate and degree of loss of adrenal function Degree of physiologic stress Primary Mineralocorticoid deficiency Secondary/Tertiary Mineralocorticoid sufficient

28
Adrenal Insufficiency Presentation
Dehydration Hypotension/shock Syncope Abdominal pain Recurrent and unexplained Mental status changes Nausea and vomiting Weight loss Fatigue Hyperpigmentation Vitiligo

29
Adrenal Crisis Presentation
Unexplained hypoglycemia Hyponatremia Hyperkalemia Hypercalcemia Eosinophilia Other autoimmune deficiencies Hypothyroid Hypogonadal

30
Adrenal Crisis Populations at Risk
Secondary adrenal insufficiency Exogenous steroid use Joint injections Herbals from Mexico High dose inhaled steroids Congenital Adrenal Hyperplasia

31
Primary Adrenal Insufficiency Etiology
Autoimmune adrenalitis 70% of cases Polyendocrinopathy-candidiasis-ectodermal dystrophy (APECED)- PGA I Autosomal recessive disorder Mutation in zinc finger protein Adrenal failure, hypoparathyroidism, mucocutaneous candidiasis, dental enamel hypoplasia, dystrophy of the nails
- PGA I. Autosomal recessive disorder. Mutation in zinc finger protein. Adrenal failure, hypoparathyroidism, mucocutaneous candidiasis, dental enamel hypoplasia, dystrophy of the nails.")
32
Primary Adrenal Insufficiency Etiology
Autoimmune adrenalitis Polyglandular autoimmune II Primary adrenal insufficiency, Autoimmune thyroid disease (hypo and hyper), Type I Diabetes, hypogonadism Infectious Tuberculosis 5% of cases Rifampin will increase cortisol metabolism-higher dose needed Histoplasmosis Ketoconazole inhibits steroid synthesis
, Type I Diabetes, hypogonadism. Infectious. Tuberculosis. 5% of cases. Rifampin will increase cortisol metabolism-higher dose needed. Histoplasmosis. Ketoconazole inhibits steroid synthesis.")
33
Primary Adrenal Insufficiency Etiology
Bilateral adrenal hemorrhage Ill patients on anticoagulants Coagulopathies Heparin Thrombosis and thrombocytopenia Primary antiphospholipid antibody syndrome

34
Primary Adrenal Insufficiency Etiology
Adrenoleukodystrophy and adrenomyeloneuropathy X-linked Defect in β-oxidation Mutations in gene encoding a peroxisomal membrane protein of the ABC superfamily of membrane transporters Demyelination of central and peripheral nervous system High levels of very long chain fatty acids (VLCFA)
")
35
Primary Adrenal Insufficiency Etiology
Familial glucocorticoid Deficiency Autosomal recessive ACTH resistance High plasma ACTH concentrations Cortisol and androgen deficiency Aldosterone is normal Presents in childhood Hyperpigmentation Muscle weakness Hypoglycemia and seizures Low epinephrine

36
Primary Adrenal Insufficiency Etiology
HIV/AIDS Adrenal necrosis Infiltrative etiologies CMV or TB Bilateral metastatic infiltration Breast cancer Bronchogenic carcinoma Renal malignancies

37
Primary Adrenal Insufficiency Etiology
Drugs that inhibit cortisol synthesis Aminoglutethimide Etomidate Ketoconazole Metyrapone Suramin Mitotane Accelerate cortisol metabolism Phenytoin Barbituates Rifampin

38
Secondary Adrenal Insufficiency Etiology
Glucocorticoid use Pituitary Tumors Hemorrhage Pituitary necrosis (Sheehan Syndrome) Metastatic malignancies Lymphocytic hypophysitis Sarcoidosis Histiocytosis X Developmental abnormalities Pit-1 Prop-1 Septo-optic dysplasia
 Metastatic malignancies. Lymphocytic hypophysitis. Sarcoidosis. Histiocytosis X. Developmental abnormalities. Pit-1. Prop-1. Septo-optic dysplasia.")
39
Adrenal Insufficiency Diagnosis
Always test for thyroid sufficiency Insulin Hypoglycemia test Tests anterior pituitary function Insulin 0.15U/kg/body Cortisol and growth hormone drawn at baseline Repeat when glucose <35 mg/dl Contraindicated Elderly, CAD, seizures

40
Adrenal Insufficiency Diagnosis
Overnight Metyrapone testing Tests for secondary or tertiary abnormalities Blocks 11β-deoxycortisol to cortisol Can initiate adrenal crisis Useful in determining return of function from steroid suppression Normal result Increased ACTH Increased 11β-deoxycortisol Metyrapone is difficult to obtain

41
Adrenal Insufficiency Diagnosis
High dose- 250 mcg ACTH Evaluates primary disease Critically ill Inpatient setting Low dose 1 mcg ACTH Evaluates primary Secondary if long standing Outpatient setting Evaluating for return of adrenal function Secondary cause Normal renin-angiotensin system Normal kalemia No hyperpigmentation Baseline critical samples Hypoglycemia or hypotension Metabolic panel, CBC, Cortisol, ACTH Thyroid function studies

42
Anti-Inflammatory Action
Steroids Potency Steroid Anti-Inflammatory Action HPA Suppression Salt Retention Cortisol 1 Prednisolone 3 4 0.74 Methylprednisolone 6.2 0.5 Dexamethasone 26 17 Fludrocortisone 12 125

43
Adrenal Crisis Inpatient Treatment
Fluid resuscitation Saline and dextrose Hydrocortisone (Solucortef) 100 mg IV bolus then 100mg IV Q6hrs Once stable Wean hydrocortisone 50 mg IV Q6-8hrs Taper and transition to oral therapy If primary Once saline heplocked Start Florinef (fludrocortisone 0.1 mg PO QD)
 100 mg IV bolus then 100mg IV Q6hrs. Once stable. Wean hydrocortisone. 50 mg IV Q6-8hrs. Taper and transition to oral therapy. If primary. Once saline heplocked. Start Florinef (fludrocortisone 0.1 mg PO QD)")
44
Outpatient Treatment Cortisol
Hydrocortisone 10mg AM and 5 mg PM 6-8 mg/m2/day Stress dosing Fever, illness, surgery 20 mg/m2/day Double or triple daily dose 100 mg x1 then mg Q6-8hrs All adrenal insufficient patients need a medic alert bracelet

45
Outpatient Treatment Alternative glucocorticoid replacement
Dexamethasone 0.5 mg ( ) per day Prednisone 5 mg ( ) per day Florinef dosing Usual production 100mcg per day mg (50-200mcg) per day
 per day. Prednisone 5 mg ( ) per day. Florinef dosing. Usual production 100mcg per day mg (50-200mcg) per day.")
46
Questions?

Similar presentations

, FRCP Consultant Endocrinologist>")

 By: Anna Heideman & Angela Mullins.>")




 are the triangle-shaped and orange- colored endocrine.>")







… gluconeogenesis in the liver.. Hyperglycemia… increased insulin output…>")

 glucocorticoids (2)mineralocorticoids (3) adrenal androgens.>")

