Download presentation
Presentation is loading. Please wait.

2
High risk population in GI field how we can find them? Ahmad Shavakhi MD Associate professor of gastroenterology

3
Gastric cancer Alarm sign in dyspepsia Weight loss Blood in stool Vomiting FHx positive for gastric cancer Dysphagia Mass in PH/E

5
Fist degree relatives of gastric cancer patients?

6
Colon cancer Second most commonly diagnosed cancer in women and third most common in men 90 percent of cases occurring after age 50

7
Colon cancer : preventable

9
Age over 50 years old

12
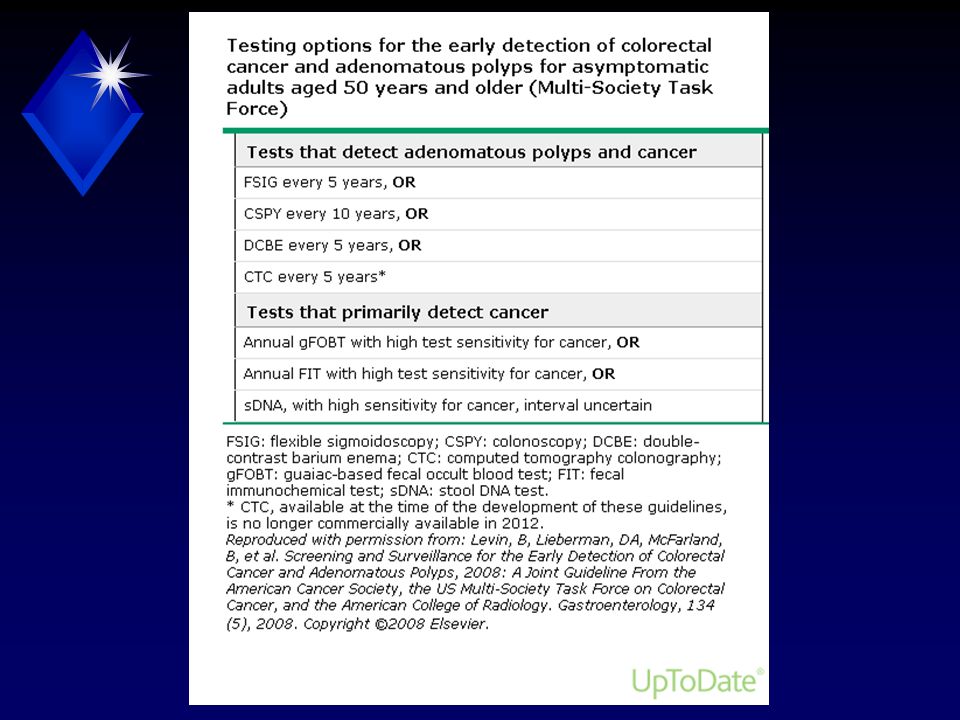
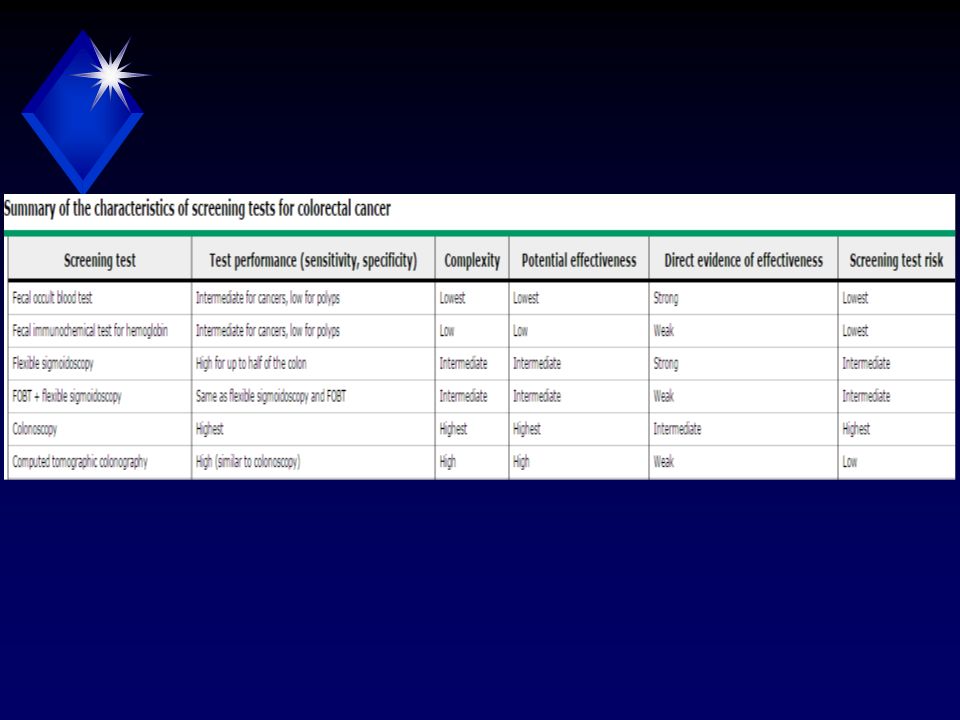
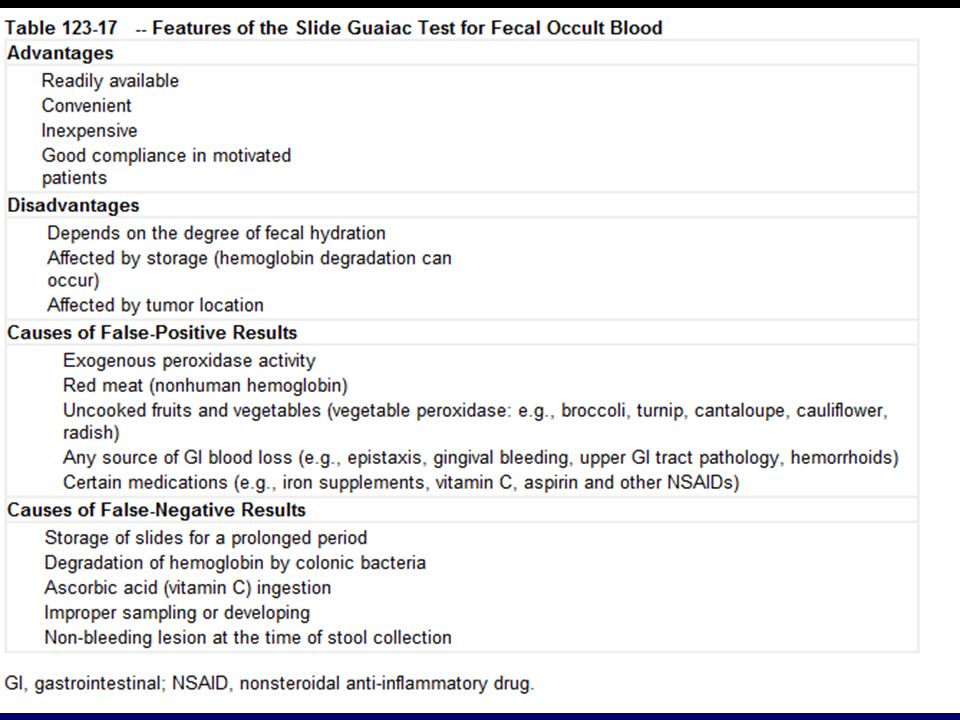
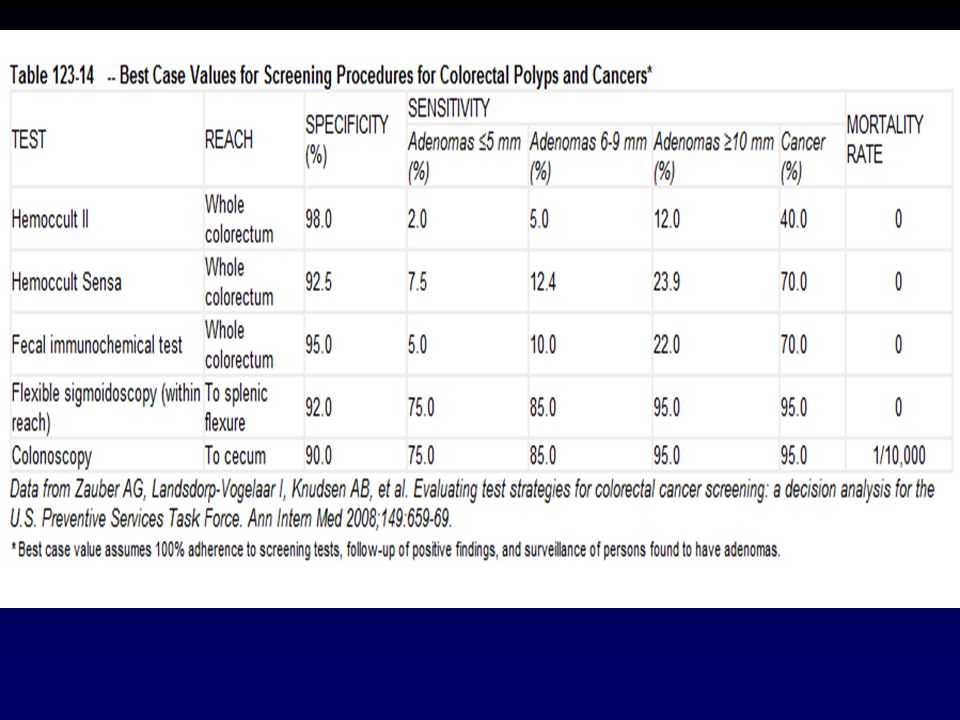
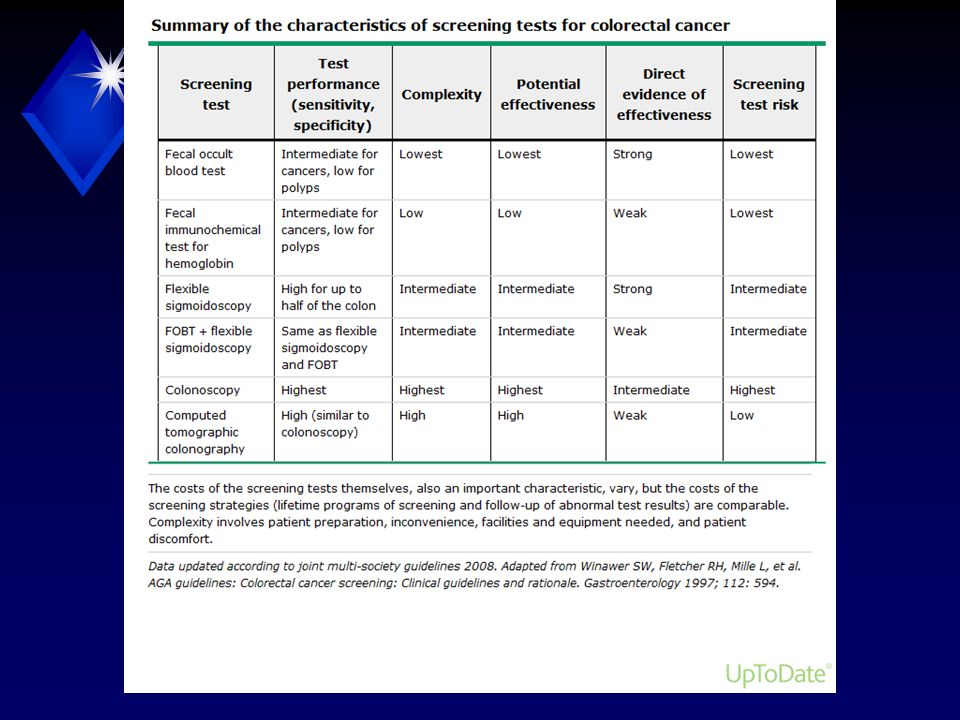
FOBT

15
Ct colonograghy

16
Colon cancer RISK ASSESSMENT: Have any blood relatives had colorectal cancer or a precancerous polyp? If so: How many Were these first-degree relatives or second-degree relatives At what age were the cancers or polyps diagnosed?

17
Advanced adenoma ≥1 cm, or high-grade dysplasia, or villous elements

18
single first-degree relative was diagnosed before 60 years with CRC or an advanced adenoma Colonoscopy is recommended at age 40 or 10 years before the youngest relative's diagnosis, to be repeated every five years

19
two or more first-degree relatives had colorectal cancer or advanced adenomas at any age colonoscopy is recommended at age 40 or 10 years before the youngest relative's diagnosis, to be repeated every five years

20
Single first-degree relative was diagnosed at age 60 years or older with CRC or an advanced adenoma

22
Digital rectal examination One in four colorectal cancers is in the rectum, and many are within an examiner’s reach on digital rectal examination. Little evidence to support the effectiveness of digital rectal examination for the detection of rectal cancer It is not recommended in current colorectal screening guidelines

23
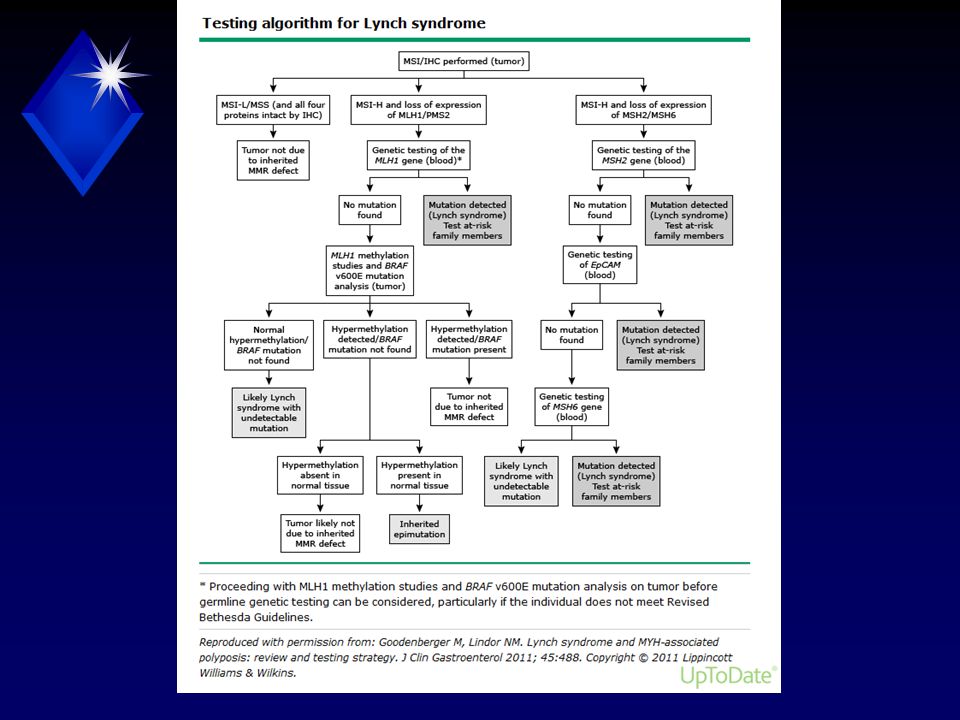
2 or more first degree relatives with hnpcc cancer

25
Annual colonoscopy ages of 20 and 25 years, or 10 years prior to the earliest age of colon cancer diagnosis in the family (whichever comes first Annual endometrial biopsy and CA 125 and transvaginal ultrasound beginning at age 30 to 35 years, or 5 to 10 years earlier than the earliest age Discussion of prophylactic hysterectomy and salpingo- oophorectomy at the end of childbearing years. Annual urinalysis beginning at age 25 to 35 years Annual skin surveillance Periodic upper endoscopy

26
survivors of childhood cancer who received 30 Gy or more of abdominal radiation Colonoscopy every five years Screening beginning 10 years after radiation or at age 35 years

27
IBD left-sided UC colonoscopy after 12 years of disease; examinations are then performed every year thereafter Proctits Do not performing surveillance Pancolitis

28
Polyp 1 or 2 small tubular adenomas with LGD 5-10 yr after initial polypectomy 3 to 10 adenomas or 1 adenoma >1 cm or any adenoma with villous features or HGD 3 yr after initial polypectomy >10 adenomas on a single examination <3 yr after initial polypectomy Patients with sessile adenomas that are removed piecemeal to 6 months to verify complete removal

30
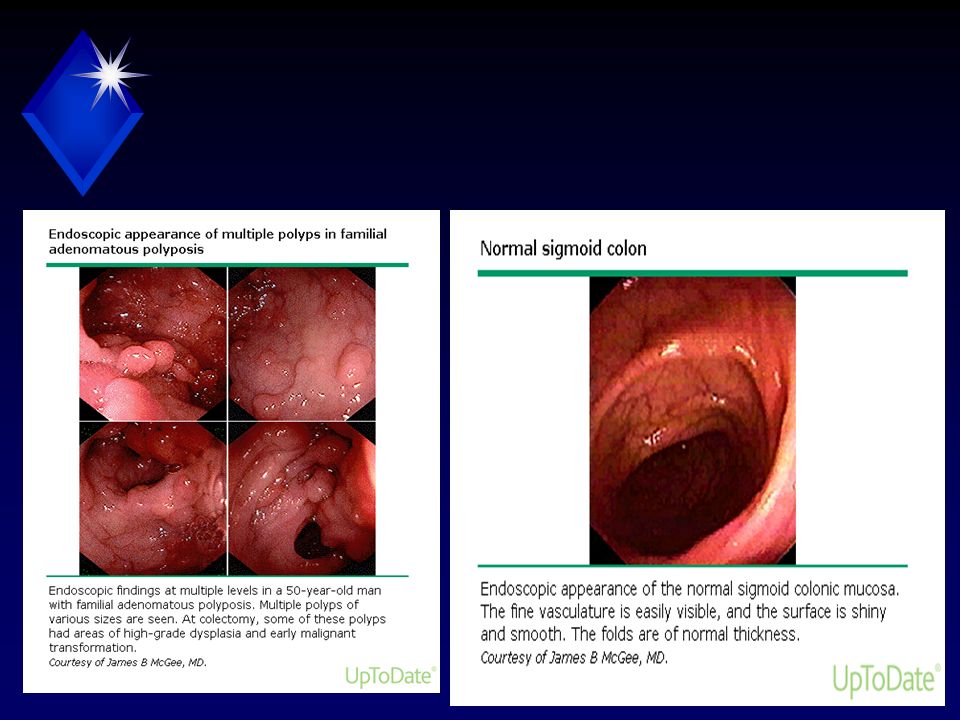
Fap Classic FAP is characterized as the presence of 100 or more adenomatous colorectal polyps

Similar presentations